Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
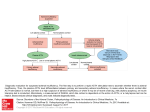
Adrenal Problems Anatomy Pathophysiology Adrenal OVERLOAD (Cushing’s syndrome) Aldosterone OVERLOAD Zona glomerulosa: outer; aldosterone Zona fascitulata: middle; cortisol Zona reticularis: inner; androgens CRH from hypothalamus ACTH from APG Cortisol from adrenal cortex Effects of cortisol: release of CRH and ACTH Gluconeogenesis, lipolysis ketogenesis, insulin release BSL effects of cytokines, cell mediated immunity, anti-inflammatory RAA aldosterone from adrenal cortex Effects of aldosterone: Na ( reabsorption), H20 excretion K ( excretion) in DCT alkalosis ( H excretion) Cause: Iatrogenic (steroids, ACTH; most common cause) Pituitary adenoma (Cushing’s disease) Adrenal adenoma / cancer / hyperplasia Ectopic CRH (eg. Pancreas, bronchial carcinoid, thymic cancer) Ectopic ACTH (20%; eg. Oat cell cancer lung) Examination: moon face, buffalo hump, truncal obesity, acne, striae, hursutism, atrophic skin, osteoporosis, HTN, peri oedema, diabetes, psych (>70%), bitemporal hemianopia, adrenal cancer If 2Y to ACTH – no Cushingoid fetaures, but HTN, oedema, prox myopathy, hyperpigmentation, cachexia Investigations: hyper HTN / glycaemia Hypo K Metabolic alkalosis Hb, neutrophils Cortisol: at 00:00; >200 = Cushings 24hr urinary cortisol: 85% sensitivity; false –ive if dilute urine Corticotropin Dexamethasone suppression test: 24hr urine for 2/7; cortisol and ACTH blood test at 09:00; dexamethason 1mg given at 11pm; normal should be to <50% baseline level Cause: 1Y: Conn’s syndrome (F:M 2:1; adenoma in F, hyperplasia in M) 2Y: due to RAA from blood flow or perfusion pressure; underlying oedematous disorder; congestive cardiac failure, chronic liver / renal failure, renal artery stenosis; Bartter’s syndrome (normal BP, no oedema, hypoNa) Examination: HTN, weakness, paraesthesia, polyuria Investigation: hyper Na / volaemia / HTN Hypo K / Ca Metabolic alkalosis Renin and aldosterone mid-morning Adrenal Insufficiency Cause: can be precipitated by: surgery, MI, general anaesthetic, hypoglycacemia, hypothermia, trauma, psych illness, drugs 1Y: there is an aldosterone deficiency hypovolaemia, high K adrenal haem (anticoagulants, neonates, sepsis – Freidrich-Waterhouse syndrome) Addison’s disease (80%) Autoimmune diseases (70%; eg. Antiphospholid syndrome) Surgical removal Drugs (long term steroids most common cause – recovery post-steroids takes 1-12/12; ketoconazole) Infection (TB – most common infectious cause worldwide, AIDS – mot common infectious cause in USA (20%), protozoa, CMV, HSV); 60% patients with sepsis have decr cortisol Cancer (usually 1Y; lung and lymphoma most common cause of 2Y) Congenital adrenal hyperplasia: vague presentation at 2wks; look for virilisation Other (sarcoidosis, haemochromatosis, hereditary) 2Y: aldosterone is normal euvolaemia, low K pituitary failure, hypothalamic failure, head trauma, meningitis, irradiation / post op, Sheehan syndrome Pathophysiology: 90% of gland must be destroyed to cause hypoadrenalism Results in: 1Y: Hypo Cl / Na / osmolality / volaemia (Na rarely <120; total body depletion + intracellular movement) Hyper K (rarely >7; extracellular mvmt + decr excretion) Non- anion gap metabolic acidosis Always consider if fluid-resistant hypotension 2Y: no volume depletion; low K; high / low Na; little other change in elecrolytes as aldosterone normal Symptoms: anorexia, nausea and vomiting, diarrhoea, abdominal pain, lethargy, weight loss, weakness, postural syncope Examination: pigmentation if 1Y; SBP <100 with postural drop Investigation: as above + creatinine, mild Ca (in 10-20%), mild hypoglycaemia; anti-adrenal antibodies Cortisol: within 1hr of waking; <200 = insufficiency; 200-500 = needs ACTH stimulation test ACTH stimulation test: bloods Synacthen IM bloods 30mins bloods 60mins cortisol >550 = normal; if normal response = 2Y ACTH: high = 1Y; low = 2Y Mng: IV fluid (may need ++); treat hypoglycaemia; treat K if needed; vasopressors may be needed If uncertain diagnosis: Dexamethasone 10mg IV stat 4mg QID If certain: hydrocortisone 250mg IV stat 100mg QID; 25mg IV if neonate, 50mg IV toddler to school child, 100mg to adolescents