Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
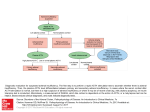
Adrenal Insufficiency HALEY MINNEHAN, MD Adrenal Insufficiency Definition A disease state that is caused by lack of glucocorticoids(GC) and/or mineralcorticoids (MC) by interruption at any level of the hypothalamus-pituitaryadrenal axis. Hypothalamus-Pituitary-Adrenal Axis Adrenal Insufficiency Primary? Secondary? Tertiary? Primary (Addisons) Destruction Of the Adrenal Cortex Primary=Primary Gland Failure = No cortisol or MC 1. Autoimmune 2. Infectious 3. Drugs >Most Common TB Ketoconazole >Lymphocytic infiltration destroys entire adrenal cortex CMV Rifampin Histoplasmosis Etomidate >Antibodies are detectable Primary Causes continued….. 4.Deposition Diseases 5. Metastatic Disease Sarcoidosis 6. Congenital Adrenal Hyperplasia Amyloidosis Hemochromatosis 7. Adrenal Surgery 8. Bilateral adrenal gland hemorrhage Secondary= Lack of ACTH =Pituitary Problem Secondary Causes Autoimmune - Lymphocytic hypophysitis Postpartum hemorrhage-Sheehan’s syndrome Head Trauma Tumor Infiltrative Process Pituitary surgery Tertiary Causes 1. Exogenous 2. Megestrol 3. Opiates Has some GC properties so will affect the axis Affects the axis at the CRH level. Glucocorticoids Prolonged therapy that is withdrawn What does cortisol do? MAINTAINS GLYCOGEN (cause of hypoglycemia) REGULATES IMMUNE FUNCTION (more infections) PART OF HEPATIC NEOGENESIS (gut absorption, nausea, diarrhea, vomiting) VASCULAR TONE (cause of hypotension) What does MC =Aldosterone do? • Regulates Na and K at the level of the kidney/ renin-angiotensin system (Very little aldosterone secretion comes from ACTH stim) Lack of aldosterone as in Primary AI a) renal wasting of Na b) retention of K c)volume loss >>severe intravascular depletion>>>hyptotension and shock Renin-Angiotensin-Aldosterone Loop What does AI feel like? Chronic AI Symptoms GI Unexplained abdominal pain Weight loss Chronic Nausea Constipation Vomiting CNS OTHER Headache Fatigue Cognitive clouding Weakness Hypersomnia Chills Depression Recurrent infxns Anxiety Tan skin (Primary) Hypotension Normal vs SAI Cortisol Pattern JFK had Addisons Hyperpigmented Chronically ill How sick was JFK? ALWAYS BE IN YOUR DIFFERENTIAL OF SHOCK LOOK FOR: Acute Adrenal Crisis 1.HYPOGLYCEMIA 2. ACIDOSIS 3. HYPONATREMIA 4. HYPERKALEMIA PRIMARY=LOW NA, HIGH K #1 IS GI FROM VOMITING/DIARRHEA SURGERY ACUTE ADRENAL CRISIS CAUSES HEAT EMOTIONAL DISTRESS TRAUMA PREGNANCY INFECTION ACUTE ADRENAL CRISIS TREATMENT STEROIDS AND FLUIDS 100 mg IV Hydrocortisone stat then Q8 hours x 24 hours Normal Saline Correct hypoglycemia D5 with 100 mg IV HC if needed Laboratory Diagnosis 8-9 am cortisol with ACTH Cortisol Level: >18 mcg/dl excludes AI <3 is virtually diagnostic < or =10 is suggestive and should start therapy before get further testing 11-18 hold therapy and obtain ACTH stim test (cosyntropin) Sepsis workup without AI baseline cortisol < or = to 10 think AI ACTH Level: >or = to 22 is virtually diagnostic of primary AI ACTH STIM TEST (Cosynotropin) Give 250 mcg IV Cosynotropin Measure serial cortisol serum levels at 30 and 60 minutes Cortisol < 5 = Adrenal Failure Cortisol >20 = Normal Cortisol 5-20 = Pituitary Failure Goals of Treatment #1 #2 #3 Physiological Improve QOL Prevent Adrenal Replacement Of GC/MC Crisis Glucocorticoid Replacement Options 1) HYDROCORTISONE 2) PREDNISONE 3) DEXAMETHASONE Glucocorticoids are not all created equal NONE ARE IDEAL IN AVOIDANCE OF RISKS OF OVER OR UNDER REPLACEMENT MOST PHYSIOLOGICAL = HC PREDNISONE POTENCY= 4XHC DEXAMETHASONE=NO EFFECT ON VASCULAR TONE LAST 24-36 HRS Chronic AI Treatment Primary Hydrocortisone 20-30 mg/day Secondary Hydrocortisone 10-25 mg/day Most physiologic Divide doses up to TID Divide doses up to TID 7.5/5/2.5 (all combinations) 10/5/5=7am/12 pm/5 pm Fludocortisone 0.05-0.1 mg/day No need for fludocortisone because aldosterone not under ACTH influence Chronic AI Treatment cont… Tertiary Removal of the offending drug with a taper if possible (reversible) Treat with maintenance HC if not able to d/c drug As little as 20 mg/day prednisone for 7 days can cause AI Be suspicious in asthmatics, COPD, rheumatology pts Hydrocortisone GOOD Restores physiology and relieves some symptoms Nausea, weakness, headache, abdominal pain, hypotension Allowed longer life span of AI patients Prior to GC pts lived max 2 years after diagnosis BAD Cannot replace the physiologycircadian rhythm ie TIMING Side effects: depression, irritability, insomnia, bone metabolism Short acting- peaks at 1-2 hours then rapid decline until next dose at hr 4-5 Absorption rate variable Treatment is Challenging Physiological demands change throughout the day depending on the day. No objective measurement of cortisol that is “normal” for that individual. Ideal world = fingerstick rapid test so with symptoms know what to treat Symptoms checklist: bp, fluids, low blood sugar, stress not accouneted for, infection, sleep deprived Treatment is often trial and error Despite treatment morbidity is high and life expectancy is reduced WHY? Non-physiological nature of replacement therapy Compliance with twice-three times daily dosing is difficult Overexposure to GC> 30 mg per day=Cardiovascular Complications, Osteoporosis, Infections, Glucose Intolerance, Insomnia, Obesity Underexposure= Infections, adrenal crisis, feel “post call” all the time, hypersomnia, significant impairment in physical, emotional and cognitive functioning affecting work, family, social Stress Dosing! Ideal to “anticipate” the upcoming stressful event Travel, holidays, call, prolonged exercise (football game), emotional distress, illness, surgery, pregnancy Double or Triple the maintenance dose for 3 days then taper for 3 days until reach maintenance doses Challenging- again How much? How long? Stress dose for prolonged exercise Patient and Family Education on Management Life threatening disease that requires lifelong replacement Educate and Reiterate the importance of stress dosing and how to avoid v adrenal crisis ID Emergency bracelet>>”Adrenal Failure- Need steroids” Emergency kit with 100 mg HC vials, needles, syringes for vomiting/diarrhea or other illness and cannot keep oral down Give Prevnar and Pneumovax to prevent recurrent sinusitis/bronchitis PATIENTS REPORT POOR QOL WORLDWIDE SURVEY OF 1245 PTS: Despite treatment…. 64% REPORTED COMPROMISED HEALTH STATUS 40% MISSED SCHOOL OR WORK IN LAST 3 MONTHS 38% HOSPITALIZED IN LAST YR 25% DISABILITY Patients need support Support groups NADF (National adrenal disease foundation) Website: www.nadf.org provides information on emergency kits, patient information, newsletter and online support group- inspire.com Quality of Life Discussions: stress, exercise, routine, dosing compliance, sleep (no dosing after 6 pm), relationships, family life, work Journaling dosing times, bp, hours of sleep, stress What is in the Pipeline? Cortisol pumps Long acting/IR Cortisol Adrenal Insufficiency after 4 years of Treatment Thank you IAFP.