Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Vaccination wikipedia , lookup
Duffy antigen system wikipedia , lookup
Molecular mimicry wikipedia , lookup
DNA vaccination wikipedia , lookup
Immune system wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Innate immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Autoimmunity wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
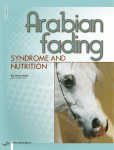
Regression of Nevi After Candida Injection for the Treatment of Verruca Vulgaris Emily Kollmann DO, David Cleaver DO, Lloyd Cleaver DO Northeast Regional Medical Center, ATSU-KCOM Abstract Discussion Importance: Many treatments exist for verruca vulgaris. The most common treatment methods are destructive methods that are often painful and treat individual verruca. Thus immune modulators including, Candida immunotherapy, are used to treat persistent recalcitrant and multiple verruca simultaneously. Observation: Very few serious side effects are reported with Candida immunotherapy including vitiligo and now halo nevi. Conclusions and Relevance: Physicians need to be aware and discuss side effects with patients receiving Candida immunotherapy. Candida antigen is a commonly used immune modulator used to treat recurrent, recalcitrant or multiple verruca. However, the same immunomodulating technique has been conducted using paramxyovirus and trichophyton. Other immune modulators include imiquimod and contact sensitizers such as diphencyprone and squaric acid dibutyl ester. There are accounts of Candida immunotherapy inducing vitiligo (2). The induction of vitiligo may occur secondary to immune modulators that may induce cytotoxic effects on melanocytes or by revealing occult disease through koebnerization (3, 4, 5). It has also been proposed through a murine model that vitiligo is induced secondary to a local inflammatory response secondary to the trauma of the injection (6). Similarly, the regression of nevi in our patient could be secondary to the induction of cytotoxic effects on the nevus cells as distant nevi began to regress. Thus physicians should educate patients and their parents that regression of nevi and the onset of vitiligo are possible side effects from Candida immunomodulating therapy. Figure 2 – Regression of nevi at third visit Introduction Case Report Verruca vulgaris is a viral induced disease frequently seen in children. Treatment is often difficult for both the patient and the physician. Destructive methods such as cryotherapy, cantharidin, laser ablation and excision are used most commonly to treat verruca. Destructive methods are often painful and treat only individual lesions. Methods such as Candida immunotherapy were developed to treat numerous verruca simultaneously with less pain. Candida immunotherapy presumably enhances recognition of the virus by the immune system allowing for distant recognition and clearing (1). It is possible that alerting the immune system to the human papillomavirus could alert the immune system to other entities such melanocytes or nevus cells. Thus, resulting in the onset of vitiligo and halo nevi. A seven year old female with no significant past medical history presented with a single verruca vulgaris on the left anterior medial malleolus. The lesion was pared with a 15 blade and treated with liquid nitrogen. The lesion was also injected with 0.1 ml of Candida antigen. At the first visit, a normal appearing congenital nevus was also noted on the right distal posterior upper arm measuring 3.5 cm by 1.5 cm. The patient returned for follow up a month later. The verruca vulgaris was treated with a second 0.1 ml Candida antigen injection. Her congenital nevus developed a surrounding area of depigmentation. At her third follow up visit a month later; her verruca was treated with a third Candida antigen injection of 0.1 ml. At this visit, her other benign appearing nevi developed areas of surrounding depigmentation in addition to her congenital nevus seen in Figure 1 and 2. At her fourth follow up appointment one month later, the verruca was again treated with a fourth Candida antigen injection of 0.1 ml. The patient did not return for five months. At that time, the verruca had resolved. The perilesional depigmentation of the congenital nevus remained and the pigmented area had regressed to measure 3.1 cm by 1.2 cm. Similarly, her other small nevi showed perilesional depigmentation and regression. Two of her nevi had completely regressed leaving areas of depigmentation seen in Figure 3. She was seen six months later in which her congenital nevus continued regressing, seen in Figure 4. She also began to develop larger areas of depigmentation in which topical steroids were prescribed to halt the progression. Figure 1 – Regression of her congenital nevus at third visit RESEARCH POSTER PRESENTATION DESIGN © 2015 www.PosterPresentations.com Figure 4 – Regression of her congenital nevus at the sixth visit Figure 5 - Depigmented patch from the sixth visit References Figure 3 - Complete regression of nevi at fourth visit Johnson SM, Roberson PK, Horn TD. Intralesional injection of mumps or Candida skin test antigens: a novel immunotherapy for warts. Arch Dermatol. 2001; 137:451-455. Wilmer E, Burkhart C, Morrell, D. Goodbye Warts, Hello Vitiligo: Candida Antigen-Induced Depigmentation. Ped Dermatol. 2013; 30(6): e214-e215. Mashiah J, Brenner S. Possible mechanisms in the induction of vitiligolike hypopigmentation by topical imiquimod. Clin Exp Dermatol. 2008; 33:74-76. Brown T, Zirvi M, Cosarelis G et al. Vitiligo-like hypopigmentation associated with imiquimod treatment of genital warts. J Am Acad Dermatol. 2005; 52:715-716. Lane C, Leitch J, Tran X et al. Vaccination-induced autoimmune vitiligo is a consequence of secondary trauma to the skin. Cancer Res. 2004; 64:1509-1514.