Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Molecular mimicry wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
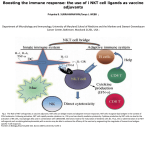
Am J Physiol Gastrointest Liver Physiol 294: G1–G8, 2008. First published October 18, 2007; doi:10.1152/ajpgi.00437.2007. Themes Role of NKT cells in the digestive system. IV. The role of canonical natural killer T cells in mucosal immunity and inflammation Gerhard Wingender and Mitchell Kronenberg La Jolla Institute for Allergy and Immunology, San Diego, California Submitted 24 September 2007; accepted in final form 18 October 2007 innate immunity; colitis TO BE OR NOT TO BE: THE MANY NAMES OF NKT CELLS Natural killer T (NKT) cells are a unique subset of T lymphocytes found in mice, humans, and other mammals. Like natural killer (NK) cells, they exhibit features of innate immunity, but they also share properties with conventional T lymphocytes. They were originally defined by their coexpression of an ␣ T cell antigen receptor (TCR) and NK cell receptors, especially NK1.1 (NKR-P1C) in certain mouse strains and CD161 (NKR-P1A) in humans. However, this classification is an oversimplification, as conventional T cells can express NK cell receptors, especially after activation. Moreover, the expression of NK cell receptors by NKT cells varies with their maturity and activation state and, in mice, with the genetic background. As knowledge of the properties of NKT cells has increased, these cells have been subdivided according to their TCR ␣-chain, the selecting antigen-presenting molecule, and the expression of various surface molecules (for reviews, see Refs. 30, 62, 68). However, despite attempts, the lack of a generally accepted nomenclature has made the field confusing. Here, we propose Address for reprint requests and other correspondence: M. Kronenberg, La Jolla Institute for Allergy and Immunology (LIAI), 9420 Athena Circle, San Diego, CA 92037 (e-mail: [email protected], URL:http://www.liai.org). http://www.ajpgi.org a classification based on TCR usage and the antigen-presenting molecule recognized. Thereby, four populations of NKT cells can be distinguished (see Table 1). The first two NKT cell populations have a canonical TCR and are specific for a nonpolymorphic major histocompatibility complex (MHC) class I-like molecule. “Canonical” and “invariant” have been used synonymously, but historically the mouse V␣14 invariant (V␣14i) NKT cells, along with their human homologs that express a V␣24i TCR, have been termed invariant (iNKT). Therefore, we will use the expression “canonical (c)NKT cell” to include both the V␣14/V␣24i NKT cells and a second population that expresses a fixed V␣7.2i TCR in mice and a homologous V␣19i in humans, named here mucosal (m)NKT cells. A third group, termed variant (v)NKT cells, encompasses T lymphocytes reactive to CD1d but that do not have a restricted TCR usage. The fourth group is more heterogeneous because it combines all other T cells that express NK receptors. This group has been termed xNKT cells or tgNKT cells (when they express a TCR transgene). Not listed in Table 1 are T lymphocytes with a ␥␦-TCR that express NK receptors. There are also T cell subsets reactive with other MHC class I-like or nonclassical class I molecules. Examples include T cells reactive with the human group I CD1 molecules, CD1a, -b, -c, which also present lipid-containing antigens, and T cells specific for the mouse H2-M3 molecule, which present peptides with a formylated amino terminus derived from bacteria. Although these cells may share some properties with the NKT cells described above, they generally do not express NK receptors. In this review, we focus on the two populations of cNKT cells, particularly on their role in mucosal immunology. THE JANUS-LIKE CHARACTER OF iNKT CELLS The largest and best-studied fraction of NKT cells carries a canonical V␣14 to J␣18 TCR rearrangement (V␣14i) in mice and an orthologous V␣24-J␣18 TCR chain (V␣24i) in humans. These are coexpressed with a limited set of V-chains, predominantly V8.2 in mice and V11 in humans, although these have highly diverse rearrangements to J-segments. V␣14i and V␣24i iNKT cells recognize glycolipid structures, presented by CD1d, a nonpolymorphic MHC class I homolog. There is a surprising degree of interspecies cross-reactivity, with mouse V␣14i NKT cells recognizing human CD1d and vice versa. The recently described trimolecular structure of a glycosphingolipid (GSL) bound to human CD1d, which is recognized by a V␣24i TCR (6), illustrates the importance of The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 0193-1857/08 $8.00 Copyright © 2008 the American Physiological Society G1 Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 Wingender G, Kronenberg M. Role of NKT cells in the digestive system. IV. The role of canonical natural killer T cells in mucosal immunity and inflammation. Am J Physiol Gastrointest Liver Physiol 294: G1–G8, 2008. First published October 18, 2007; doi:10.1152/ajpgi.00437.2007.—Lymphocytes that combine features of T cells and natural killer (NK) cells are named natural killer T (NKT) cells. The majority of NKT cells in mice bear highly conserved invariant V␣ chains, and to date two populations of such canonical NKT cells are known in mice: those that express V␣14 and those that express V␣7.2. Both populations are selected by nonpolymorphic major histocompatibility complex class I-like antigen-presenting molecules expressed by hematopoietic cells in the thymus: CD1d for V␣14-expressing NKT cells and MR1 for those cells expressing V␣7.2. The more intensely studied V␣14 NKT cells have been implicated in diverse immune reactions, including immune regulation and inflammation in the intestine; the V␣7.2 expressing cells are most frequently found in the lamina propria. In humans, populations of canonical NKT cells are found to be highly similar in terms of the expression of homologous, invariant T cell antigenreceptor ␣-chains, specificity, and function, although their frequency differs from those in the mouse. In this review, we will focus on the role of both of these canonical NKT cell populations in the mucosal tissues of the intestine. Themes G2 cNKT, canonical natural killer T (NKT); iNKT, invariant NKT; mNKT, mucosal NKT; vNKT, variant NKT; DN, double negative; DP, double positive; ␣GalCer, ␣-galactosylceramide; ␣ManCer, ␣-mannosylceramide; BbGL, Borrelia burgdorferi glycolipid; GSL, glycosphingolipid; iGb3, isoglobotrihexosylceramide; MHC, major histocompatibility complex; nd, not determined; TCR, T cell antigen receptor. NK1.1 Effector/memory nd Liver, spleen NK1.1 CD56, CD161 Effector/memory IL-15 Liver, thymus, spleen, bone marrow NK1.1 Common NK cell receptor Peripheral phenotype Peripheral requirements Prominent steady-state location CD161 Effector/memory MR1 on B cells, gut flora Lamina propria, lung, liver MR1 ␣ManCer Thymus hematopoietic cell DN, few CD4 DN, few CD4, CD8a␣ Restriction Reactivity Positive selection Coreceptors CD1d ␣GalCer, GSL, BbGl2, iGb3 DP thymocytes CD4 or DN CD4 or DN, CD8a␣ CD1d Sulfatide and nd Thymus, cell unknown CD4 or DN Diverse (xNKT), transgenic (tgNKT) MHC I and II Diverse peptides Thymus, cell unknown CD4, CD8␣ (mostly CD8a␣) or DN DX5 and/or NK1.1 Naive and effector/memory nd Spleen, bone marrow, liver Diverse Invariant V␣24-J␣18 Invariant V␣14-J␣18 Invariant V␣7.2-J␣33 Invariant V␣19-J␣33 Human Mouse Human Mouse iNKT Cells (also known as V␣14i or V␣24i, NKT type I or classical NKT cells) mNKT Cells (also known as V␣19i or V␣7.2i NKT, mucosal-associated invariant T cells or NKT-like cells) cNKT Cells Table 1. Features of different NKT cell subsets TCR repertoire AJP-Gastrointest Liver Physiol • VOL contacts made by the J␣18 segment with the antigen protruding form the CD1d groove. V␣14i iNKT cells have the highest frequency in the liver and the bone marrow (⬎10%), followed by significant numbers in thymus, peripheral blood, and spleen (1–3%), whereas they are relatively rare in other lymphoid organs (⬍0.5%). Interestingly, in humans the frequency of iNKT cells is generally much lower, although a high degree of interindividual variability has been reported. As noted above, there is inherent ambiguity in the term “NKT cell.” However, since the development of CD1d tetramers loaded with ␣-galactosylceramide (␣GalCer), it has been possible to unequivocally identify the iNKT cell subpopulation (33). As summarized in Fig. 1, ␣GalCer is a synthetic GSL compound that is able to strongly activate iNKT cells when bound to CD1d. Furthermore, researchers have been able to probe the functions of these cells using iNKT cell-deficient mice, either J␣18⫺/⫺ mice, which lack only iNKT cells, or Cd1d⫺/⫺ mice, which lack iNKT and the vNKT cells that have more diverse TCRs. Even as they differentiate in the thymus, iNKT cells express a pattern of cell surface markers (CD69⫹, CD44high, CD11ahigh, CD62Llow, CD122⫹) typically associated with activated or memory T cells. After activation, iNKT cells rapidly gain cytotoxic activity and produce both T helper type 1 (TH1) cytokines, such as IFN-␥ and TNF, and T helper type 2 (TH2) cytokines, such as IL-4, IL-10, and IL-13. Recent evidence suggests that subsets of iNKT cells can also produce IL-17 (34). Because of their rapid initiation of effector functions, iNKT cells have been reported to be crucially involved in the early phases of a dazzling variety of different immune reactions, ranging from self-tolerance and development of autoimmunity to include responses to pathogens and tumors (30, 62). In the different studies, iNKT cell have been shown to be either beneficial or harmful, depending on whether they polarize the immune response either toward a TH1 or TH2 direction, and the beneficial or detrimental effects of such a cytokine polarization in the context of different models. For this reason, others have referred previously to their “Janus-like” character. Fig. 1. Pictorial representation of some of the main features of canonical natural killer T (cNKT) cells. DN, double negative; ␣GalCer, ␣-galactosylceramide; iNKT, invariant natural killer T cells; ␣ManCer, ␣-mannosylceramide; mNKT, mucosal natural killer T cells. 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 vNKT Cells (also known as type II or nonclassical NKT cells) xNKT or tgNKT Cells (also known as NKT-like cells) CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION Themes CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION iNKT CELL ACTIVATION BY SELF ANTIGENS iNKT CELL ACTIVATION BY MICROBIAL ANTIGENS Abundant evidence has established an important role for iNKT cells in the host defense against several pathogens, especially in the early phases of infection (30, 62, 68). Before the discovery of iGb3, however, the only compound presented by CD1d known to activate most iNKT cells was ␣GalCer (see Fig. 1) and its derivatives. ␣GalCer, originally derived from a marine sponge, contains an unusual ␣-anomeric linkage of the sugar to the ceramide lipid, and this ␣-linkage is crucial for its stimulatory capacity. Most GSLs have -linked sugars, which do not form an epitope for iNKT cells because the hexose ring of the sugar is oriented differently. Notwithstanding the highly conserved recognition of the apparently marine sponge-derived ␣GalCer, a prevalent hypothesis was that iNKT cells recognize natural glycolipid structures derived from pathogens. However, as with the endogenous iNKT cell antigens, the first reports of exogenous iNKT cell antigens, in purified components derived from Leishmania donovani and from Mycobacterium bovis, stimulated only a minority (⬍2%) of V␣14i NKT cells. Only recently have bacterial antigens that stimulate the majority of iNKT cells been characterized, including glycolipids from environmental bacteria, Sphingomonas spp., and from Borrelia burgdorferi, the causative agent of Lyme disease (for review, see Refs. 30, 62, 68). We expect that additional bacterial species will be found to have natural iNKT cell antigens, although some bacteria, such as Salmonella spp., apparently do not have antigens. Activation of iNKT cells by TCR-mediated recognition of a foreign antigen bound to CD1d has been referred to as direct or foreign antigen-dependent activation. Apart from this, a second pathway of iNKT cell activation is currently recognized. iNKT cells can be activated by proinflammatory cytokines, such as type I IFN, IL-12, and IL-18, alone or in combination, which AJP-Gastrointest Liver Physiol • VOL are produced early after viral or bacterial infections by dendritic cells and macrophages. In some cases, it has been shown that iNKT cells additionally require the recognition of endogenous or self-ligands presented by CD1d for activation in this cytokine-dependent context (7). This type of activation leads to the production of IFN-␥ but not IL-4 by the stimulated iNKT cells. These pathways of iNKT cell activation that are independent of foreign antigen have been termed indirect activation. NKT CELLS IN THE INTESTINE Many of the studies reporting the presence of NKT cells in the intestine have relied on the coexpression of the TCR/CD3ε complex and NK cell receptors, such as NK1.1 in mice and CD161 in humans, which does not allow for the distinction of the four NKT cell populations shown in Table 1. An unequivocal identification is to date only possible for the cNKT cells, either by measuring mRNA for the canonical ␣-chain TCRs (mNKT and iNKT cells) or by flow cytometry using CD1d tetramers loaded with ␣GalCer (iNKT cells). Up to 4% of mouse small intestine (SI) intraepithelial lymphocytes (IELs) (4, 18, 25, 39), 8 –10% of large intestine (LI) IELs (4, 25), and 7% of LI lamina propria lymphocytes (LPLs) (20) have been reported to coexpress the TCR-CD3ε complex and NK cell receptors. Most of these cells were CD8␣⫹, and two-thirds thereof were CD8␣␣⫹ (4, 25). It has been noted that a significant portion of these CD3ε/NK1.1⫹ cells were ␥␦ T cells (25) and therefore not part of the four NKT cell populations defined here. Furthermore, most of these cells were CD1d independent (4, 25). With the use of CD1d tetramers loaded with ␣GalCer, a few (1%) iNKT cells have been detected in SI IELs (33), but they were more prevalent (2%) in LPLs (49). Furthermore, cells derived from colitic LI LPLs responded to ␣GalCer (20). Interestingly, 80% of the iNKT cells were NK1.1⫺ (33). However, in other studies, no tetramer-positive cells, invariant mRNA, or responsiveness to ␣GalCer could be detected in IELs (49). From these reports, one might conclude that the majority of NKT cells in the mouse intestine are CD1d independent (xNKT cells) and that iNKT cells are mainly found in LPL. In humans, the values for NKT cells have been expressed as percentages of CD3ε⫹ cells, rather than total lymphocytes. The following proportions of T cells were also positive for CD161: 50 –70% for SI IELs (23, 41), 40 – 45% for LI IELs (23, 41), and 9% for LI LPLs (14). Of these cells, 60 – 80% were CD8␣⫹ (23, 41). The dependence on CD1d could not be addressed; however, only 1.6 –1.7% of the CD3ε/CD161⫹ IEL cells expressed V␣24 (23, 41), and immunhistochemistry data suggested that the majority of the V␣24⫹ cells in the SI are actually located in the lamina propria (16). Furthermore, the majority of these V␣24⫹ cells did not express the V11 TCR chain associated with the invariant TCR (41). Therefore, the great majority of CD161⫹ T cells in human intestine are not iNKT cells, similar to results obtained by analysis of human peripheral blood mononuclear cells (PBMCs). Together with ␣GalCer-loaded CD1d tetramer data from LPL (14), one can estimate that the proportion of iNKT cells in the human intestine is ⬍0.4% of all T cells and that they are, like in the mouse, mainly localized in the lamina propria. Nonetheless, 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 The effector or memory phenotype of iNKT cells and their constitutive expression of mRNA for IL-4 and IFN-␥ suggest that they undergo a strong antigenic stimulation during their differentiation. This is consistent with the hypothesis that true TCR agonists mediate their positive selection (30). In line with this idea is the observation that mature iNKT cells can, under some circumstances, recognize endogenous glycolipids bound to CD1d. However, elucidation of the glycolipids involved in this endogenous recognition process has proven to be quite challenging. Several suggestions have been put forward (for reviews, see Refs. 30, 68); however, for these cases, only a minor fraction of the iNKT cells were responsive. The best candidate to date for a more general endogenous ligand or autoantigen for iNKT cells is isoglobotrihexosylceramide (iGb3), a GSL found in the lysosomes of some cell types. The majority of iNKT cells can recognize iGb3 when bound to CD1d (69). The inability of mutant mice to synthesize iGb3 in lysosomes, through catabolism of a tetrasaccharide precursor, has been linked to V␣14i NKT cell deficiency (69). However, recent data have raised doubts about whether iGb3 is the only endogenous antigen driving iNKT cell development (31). Particularly striking is the finding that mice deficient for iGb3 synthase have normal iNKT cell number and function (47). It seems possible that several different self-antigens can drive CD1d-restricted iNKT cell development. G3 Themes G4 CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION these iNKT cells were functionally active and produced cytokines after ␣GalCer stimulation (41). CD1d EXPRESSION IN THE MUCOSAL IMMUNE SYSTEM AJP-Gastrointest Liver Physiol • VOL NKT CELLS IN INFLAMMATORY BOWEL DISEASE Most studies addressing the role of iNKT and vNKT cells in the intestine were concerned with inflammatory bowel disease (IBD) model systems. IBD denotes a variety of what are likely to be T cell-dependent diseases of different parts of the intestine, as a consequence of an inflammatory response to antigens derived from the gut lumen. This inflammation may follow perturbation of the epithelial layer, either through genetic alterations or the administration of exogenous agents. NKT cells have been implicated in several animal models of IBD, and, although the data are not entirely consistent, the findings correlate with a protective role for NKT cells in TH1-mediated IBDs and a deleterious one in TH2 IBDs. Crohn disease is characterized by a chronic and discontinuous inflammation of both the SI and LI, with high levels of TH1 cytokines. Clinical studies have reported a significant reduction of iNKT cells, measured as V␣24/V11⫹ or ␣GalCer-loaded CD1d tetramer-positive cells, in the peripheral blood of affected patients (17, 65) and reduced V␣24 mRNA levels and V␣24-expressing cell numbers in the intestine (17). A decrease of iNKT cells in the PBMC and of V␣24⫹ T cells in the intestine has also been reported for patients with celiac disease (16). However, as noted above, the majority of these V␣24⫹ cells were not iNKT cells, as judged by the absence of V11 expression (41). For three mouse colitis models characterized by a TH1 immune response, the involvement of NKT cells has been reported, including 1) adoptive cell transfer of naive CD4 T cells into immune-deficient hosts, 2) oral challenge with dextran sodium sulfate (DSS), and 3) rectal instillation of the hapten trinitrobenzene sulfonic acid (TNBS). In the transfer model of colitis, cotransfer of T cells expressing the NK receptor DX5 with the pathogenic CD4 T cells ameliorated disease, and this effect could be blocked by injection of an anti-CD1d antibody (21). However, because only a minority of DX5⫹ NKT cells are CD1d dependent (45), it is not certain which NKT cell population was responsible for the protection, and, given the induction of IL-10 by anti-CD1d, it is possible that the antibody triggered CD1d functions independent of their interactions with subsets of NKT cells. DDS-induced colitis could be ameliorated by treatment with the iNKT cell agonists ␣GalCer (38, 50) or the closely related compound OCH (63). OCH has been reported to shift the immune response stimulated by iNKT cell activation to the TH2 cytokine pattern (36); consistent with this, the protection in the DSS colitis model was directly linked to the increased production of IL-4 and IL-10 and decreased production of IFN-␥ (63). A similar protection by OCH treatment was observed for TNBSinduced colitis; importantly, treatment with OCH was even effective at ameliorating an ongoing disease in the DSS model (63). Although in one study a single injection of ␣GalCer led to a shift to a protective TH2 response (50), two later studies reported that repetitive challenges were necessary (38, 63). This is in line with the reported TH2 shift by repetitive ␣GalCer treatment (9). These data clearly demonstrate the protective 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 As noted above, an important role for iNKT cells is possible even in the absence of CD1d expression within the local environment because of cytokine-mediated or indirect activation. However, CD1d expression obviously is a prerequisite for the local, antigen-specific activation of iNKT and vNKT cells. Because most hematopoietic cells express CD1d, CD1d also is likely to be found on antigen-presenting cells in the intestine. An example of biologically relevant CD1d expression on antigen-presenting cells in the intestine is provided by studies of mesenteric lymph node B cells. It had been found that colitis in TCRa⫺/⫺ mice is exacerbated when these mice are also deficient for B lymphocytes (37). There also was an increase in colitis when the TCRa⫺/⫺ mice were Cd1d⫺/⫺, and a subset of B cells in the mesenteric lymph node increased their expression of CD1d under inflammatory conditions (37). Transfer of this B cell subset to TCRa⫺/⫺ mice that were also B cell deficient prevented the increased colitis observed in these mice (37). Transfer of mesenteric lymph node B cells also prevented colitis induction in the Gai2⫺/⫺ model (66); however, in both of these cases, it is uncertain whether T cell reactivity to the CD1d abundantly expressed by the B cells was required for their beneficial effect. Conflicting reports have been made regarding the expression of CD1d on human and mouse intestinal epithelial cells (IECs). One reason for the controversy is the unusual form of CD1d that IECs were reported to express. Interestingly, the majority of the CD1d expressed by IECs is nonglycosylated and not associated with 2-microglobulin, and it is localized mainly inside the cells, with surface expression restricted to the apical surface (2, 28, 29, 56). Its function remains to be elucidated, and there is no evidence for the recognition of this form of CD1d by iNKT cells, although it has been suggested that some T cells, presumably vNKT cells, recognize 2-microglobulinindependent CD1d molecules (3, 10, 43). Mouse monoclonal antibodies that recognize native CD1d made by several groups do not detect this 2-microglobulin-independent form of CD1d; consequently, they do not detect CD1d expression by IECs, contributing to the above-mentioned controversy. The native 2-microglobulin-associated CD1d molecule is weakly expressed by human IECs with a preference for the basal surface (56). IECs have been reported to bind (50) and present ␣GalCer (64), suggesting that this low amount of native CD1d expression is significant, but IECs could not present derivatives requiring carbohydrate antigen processing in lysosomes (64). Contradictory data regarding the expression of CD1d in patients with colitis have been reported. Whereas one study reported higher expression of CD1d in affected tissue (42), two other reports found lower expression (15, 46). The production of the anti-inflammatory cytokine IL-10 has been linked to CD1d expression by IEC lines and primary cells, and this required an intact cytoplasmic domain of CD1d, implying a signaling function for this molecule (11, 37). Furthermore, mice lacking microsomal triglyceride transfer protein, an endoplasmic reticulum resident lipid transfer protein, display a defective loading and presenting capability of CD1d and were largely protected against oxazolone-induced colitis (8). This protection was linked to IECs, as microsomal triglyceride transfer protein within the intestine is preferential expressed by IECs; however, the authors did not directly address the role for CD1d expressed by IEC. Themes CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION NKT CELL RESPONSES DURING INTESTINAL INFECTIONS There is evidence for a role for iNKT and/or vNKT cells after oral infections with several pathogens. Listeria monocytogenes, the causative agents of listeriosis, is a Gram-positive, facultative, intracellular pathogen. It is acquired by food-borne infection, and it is cleared by the immune system via a TH1 immune response. After intragastric infection of L. monocytogenes in mice, iNKT cells produced IFN-␥ but not IL-4 within 1–2 days, and they stimulated IFN-␥ production by NK cells (1, 48). Although iNKT cells were not essential for survival, they participated in the protective immune response, as indicated by the reduced hepatic bacterial load and increased systemic IFN-␥ in mice that have iNKT cells (1, 48), and this protection could be transferred by purified iNKT cells (48). Furthermore, CD1d-deficient mice displayed higher levels of pathology in the intestine and to a lesser extent in the liver and spleen (1), suggesting that iNKT cells were important in limiting the spread of bacteria. However, another study reported the opposite effect of iNKT cell deficiency, as J␣18deficient mice displayed a higher resistance to L. monocytogenes infection (13). A protective contribution of iNKT cells after an intravenous or intraperitoneal challenge with Salmonella spp. has been established (62, 68). However, after intragastric challenge, no major impact of iNKT cell deficiency on the course of infection could be found, despite activation and cytokine production by iNKT cells (5). Note that activation of iNKT cells after AJP-Gastrointest Liver Physiol • VOL Salmonella infection is by the indirect route, as these bacteria do not have antigens that engage the V␣14i TCR (7). Toxoplasma gondii is an obligate intracellular protozoan parasite acquired by ingestion of parasitic cysts or oocysts contained in food or water. In immune-competent hosts, this infection is reliably controlled by a TH1 immune response. However, in infected C57BL/6 mice, but not in other strains, this TH1 immune response leads to lethal acute ileitis, due to overwhelming IFN-␥ production. The potential of iNKT cells to produce copious amounts of IFN-␥ after stimulation makes them a candidate for the source of the pathogenic IFN-␥ in T. gondii-infected C57BL/6 mice. In accordance with this, it has been shown that J␣18⫺/⫺ C57BL/6 mice are less susceptible to ileitis after infection with T. gondii (49). The deleterious effect of iNKT cells in wild-type C57BL/6 mice could almost entirely be blocked by pretreatment with ␣GalCer (49). Systemic challenge of the mice with ␣GalCer 1 day before T. gondii infection led to a pronounced TH2 cytokine shift of the iNKT cells, with markedly reduced IFN-␥ and increased amounts of IL-4 and IL-10 (49). IL-10, produced mainly by iNKT cells and by CD4/CD25⫹ regulatory T cells, was shown to be the main agent for protection from runaway inflammation (49). Surprisingly, however, the same report also showed that Cd1d⫺/⫺ mice had entirely the opposite phenotype compared with the J␣18⫺/⫺ mice. After T. gondii infection, the Cd1d⫺/⫺ animals had an increased mortality (49), and similar data on Cd1d⫺/⫺ C57BL/6 mice were reported by another group (55). Both reports are examples of the surprising differences between J␣18⫺/⫺ animals, specifically lacking iNKT cells, and Cd1d⫺/⫺ mice, which not only lack all CD1d-reactive iNKT and vNKT cells but also other potentially important CD1ddependent pathways, for example those based on CD1d-mediated signal transduction (see above). Despite the clear involvement of iNKT and vNKT cells in many different systemic and intestinal infections and their rapid activation by pathogenic and even nonpathogenic microbes such as Sphingomonas spp., iNKT cell-deficient mice have not been reported to be more susceptible to spontaneous infections with what are normally commensal bacteria. Furthermore, iNKT cells themselves are not dependent on commensal bacteria, as even in germ-free animals iNKT cells are phenotypically activated/memory T cells that function normally after antigenic stimulation (44). mNKT CELLS Less is known about a second population of canonical NKT cells found in humans and mice. As noted, these cells express an invariant V␣19-J␣33 (mouse)- or V␣7.2-J␣33 (human)rearranged TCR ␣-chain (for reviews, see Refs. 60, 61). The invariant TCR contains only a few N-nucleotide additions, and the coexpressed V usage is skewed to V13 and V2 in human and V8.1/8.2 and V6 in mice (51, 57). Although mNKT cells have been detected in blood, lymph nodes, liver, spleen, and bone marrow (27, 51, 53, 58), they are most prominent under steady-state conditions in mucosal sites of the gut and the lung (27, 59 – 61), hence the appellation mNKT cells, also called mucosal-associated invariant T (MAIT) cells (59). By PCR analysis for the invariant rearrangement, mNKT cells are especially enriched in the lamina propria and mesenteric lymph node and virtually absent in the 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 potential of iNKT cells that have been activated by potent agonists to shift the immune response from the deleterious TH1 cytokine pattern in these diseases to a protective TH2 response. There is also a profound lack of IL-4 production by mononuclear cells purified from the affected intestines of patients with Crohn disease (26, 67). However, it is important to note that the depletion of NK and NKT cells had no effect on the course of TNBS-induced colitis (20), and, in the absence of activation by potent synthetic agonists, it remains to be demonstrated in these models whether the normal functioning of NKT cells influences colitis. Oxazolone-induced colitis is an IBD model in which TH2 cytokines induce pathology. The mucosal immune response following oxazolone exposure is initially dominated by IL-4, which is soon superseded by an IL-13 response (20). The IL-13 derived from iNKT cells has been shown to be crucial for disease development (20), and interfering with iNKT cell activation prevented disease development (8, 20). However, in patients with ulcerative colitis, it was found that vNKT cells, rather than iNKT cells, were the major producers of the deleterious IL-13 (14). Specifically, CD4/CD161⫹ T cells accumulated in patients’ lamina propria and these cells were capable of secreting IL-13 in vitro in a CD1d-dependent fashion (14). However, these cells did not express V␣24 and did not respond to ␣GalCer (14). Notwithstanding the absence of functional data implicating iNKT cells in disease causation in humans with IBD, iNKT cells were decreased in the PBMCs of patients with ulcerative colitis (17, 65). The differing requirements in mice and humans for iNKT cells and vNKT cells, in colitis characterized by IL-13 production by T cells in the intestine, could be due in part to the lower frequency of iNKT cells in most humans. G5 Themes G6 CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION AJP-Gastrointest Liver Physiol • VOL mNKT cells are ⬃5–10 times more frequent in humans than in mice, accounting for ⬃15% of all double-negative T cells in PBMCs (i.e., 0.1– 0.2% of all T cells) and for 10% of doublenegative T cells in the intestine (59 – 61). Because of their paucity in mice, the generation of V␣19i transgenic animals has greatly facilitated the investigation of this subpopulation (27, 40), complemented by the generation of MR1-deficient mice (59). Although the high evolutionary conservation of mNKT cells and their prominence in the intestine suggest an important role in the mucosal immune system, no nonredundant function of mNKT cells in the intestinal mucosa has yet been described. For example, the frequency of V␣7.2i NKT cells is not altered in patients with Crohn disease or ulcerative colitis (61). Similar to iNKT cells, mNKT cells rapidly produce effector cytokines like IL-4, IL-5, IL-10, IL-17, and IFN-␥ after activation via MR1 or ␣CD3ε antibody in vitro and in vivo (12, 27, 52, 53, 59). mNKT cells also have the capacity to migrate to sites of inflammation, where their cytokines could influence the inflammatory process. It has been reported that they accumulate in some central nervous system lesions and in the cerebral fluid of patients with multiple sclerosis, as well as in peripheral nerve samples of patients with chronic inflammatory demyelinating polyneuropathy (24). The same group demonstrated a protective role of V␣19i NKT cells during experimental autoimmune encephalomyelitis, a mouse model of multiple sclerosis (12). Overexpression of V␣19i NKT cells ameliorated the disease, whereas depletion of V␣19i NKT cells exacerbated it (12). Furthermore, donor V␣19i NKT cells could transfer protection (12). The data indicate that the interaction of NK1.1⫹ V␣19i T cells and B cells via ICOS/ICOS-L, and to a lesser extent via CD40/CD154, induced the production of protective IL-10 by both cell populations (12). In this setting, the interaction of iTCR and MR1 seemed not to be required (12). SUMMARY For iNKT and mNKT cells, there are a number of striking similarities. Both are selected in the thymus by nonpolymorphic MHC class I-like molecules expressed by hematopoietic cells. Interestingly, CD1d and MR1 are encoded in close proximity on chromosome 1 (19), perhaps suggesting a similar evolutionary selection and function. Both cNKT cell populations display a phenotype characteristic of activated or memory cells, they rapidly secrete effector cytokines, and they exhibit a degree of autoreactivity. Both cNKT cell populations have been reported to be specific for glycolipids, although the antigens recognized by mNKT cells are not yet well characterized. Additionally, both populations are prominent in sites other than the lymph node, such as the intestine for mNKT cells or the liver, which collects circulation from the intestine, for iNKT cells. iNKT cells require CD1d in the periphery for their final differentiation, and mNKT cells depend on MR1 expression on B cells and the gut flora for their homeostasis and localization to the intestine. Selection by hematopoietic cells in the thymus might imprint the properties that cNKT cells share. In this context, it is of interest to note that the forced selection of MHC class II-reactive CD4 T cells in transgenic mice that express MHC class II only on thymocytes also led to the development of T cells bearing an effector/ 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 intestinal epithelium (27, 59, 60). In this context, the observation that V␣19i mNKT cells are absent in germ-free mice (59, 60) is quite interesting because it suggests that microbially derived stimuli, either directly or indirectly, are required for their selection and/or expansion. V␣19i mNKT cells are absent in athymic nu/nu (nude) mice (58), and hematopoietic cells mediate their thymic-positive selection, rather than the cortical epithelial cells that positively select conventional T cells (59). Furthermore, V␣19i mNKT cells are absent in B cell-deficient mice and in patients with a mutation in Bruton’s tyrosine kinase, which leads to a profound B cell deficiency (59). Innate-like B1-B cells and plasma cells are not involved, however, in forming the mNKT cell population (59, 60). Whether this dependency reflects a requirement for the few thymic B cells to select V␣19i mNKT cells in the thymus, or perhaps more likely their expansion, homeostasis, or homing in the periphery, is so far unresolved (59 – 61). In line with the latter hypothesis, the few intestinal IgA⫹ B cells that develop in -heavy chain-deficient (MT⫺/⫺) mice were sufficient for the development of V␣19i mNKT cells (59). V␣19i mNKT cells are restricted by MR1 (59), a 2mdependent nonpolymorphic MHC class I-like molecule encoded by a gene linked to the Cd1d gene (Fig. 1). Considering the entire family of antigen-presenting molecules, MR1 shows the highest degree of conservation between mouse and human (19, 35). Although MR1 mRNA is ubiquitous (19), cellular expression of the protein is still incompletely characterized. In MR1-transfected cell lines, most of the protein is retained in the endoplasmic reticulum; therefore, it has been suggested that attainment of a native conformation leading to MR1 surface expression might be limited by the availability of a specific MR1-binding ligand(s) (35). Consistent with this hypothesis, addition of a surplus of serum components could increase the surface expression of MR1 (22, 35). This and other indirect evidence (22, 35) make it very likely that MR1 acts as an antigen-presenting molecule. Furthermore, because some V␣19i mNKT cell hybridomas were activated spontaneously by MR1-transfected cell lines (22, 59), there may be a substantial degree of autoreactivity by V␣19i mNKT cells, similar to their CD1d-dependent iNKT cell counterparts. Endogenous MR1-binding ligands for potentially self-reactive mNKT cells are not known so far, but it has recently been reported that ␣-mannosylceramide and particularly some related compounds with modifications of the ceramide lipid can activate V␣19i NKT cells after binding to MR1 (40, 52–54). Consistent with their potential autoreactivity, mNKT cells display an effector/memory phenotype in the periphery characterized by the expression of CD27⫹, CD44high, CD45RA⫺, and CD57⫺ in humans (59) and CD25low, CD44high, CD45RBlow, CD62L⫺, and CD69⫹ in mice (27). Most mNKT cells are CD4⫺CD8⫺ (double negative) (27, 58), ⬃60 – 80% in mice (27). Although in mice V␣19i mNKT cells are never CD8␣⫹ (27, 58), some human V␣7.2i NKT cells express CD8␣ (58). Furthermore, mNKT cells express several costimulatory molecules such as CD28, CD154, and inducible costimulator (ICOS) (12, 27, 51, 59), as well as NK cell receptors such as NK1.1 in mice and CD161 in humans (12, 24, 27, 51, 53, 59). Finally, V␣7.2i mNKT cells have been shown to express the integrin ␣47, which is required for gut homing (59). Themes CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION ACKNOWLEDGMENTS The authors thank Barbara A. Sullivan and Dirk M. Zajonc for critical review of the manuscript (B. A. Sullivan) and for helpful discussions (B. A. Sullivan, D. M. Zajonc). Because of space constraints, we had to limit citations of the primary literature. GRANTS This work was supported by National Institute of Allergy and Infectious Diseases Grants AI-71922 and AI-45053 (M. Kronenberg) and a Marie Curie Foundation fellowship (G. Wingender). This is manuscript number 944 from the La Jolla Institute for Allergy and Immunology. REFERENCES 1. Arrunategui-Correa V, Kim HS. The role of CD1d in the immune response against Listeria infection. Cell Immunol 227: 109 –120, 2004. 2. Balk SP, Burke S, Polischuk JE, Frantz ME, Yang L, Porcelli S, Colgan SP, Blumberg RS. Beta 2-microglobulin-independent MHC class Ib molecule expressed by human intestinal epithelium. Science 265: 259 –262, 1994. 3. Balk SP, Ebert EC, Blumenthal RL, McDermott FV, Wucherpfennig KW, Landau SB, Blumberg RS. Oligoclonal expansion and CD1 recognition by human intestinal intraepithelial lymphocytes. Science 253: 1411–1415, 1991. 4. Bannai M, Kawamura T, Naito T, Kameyama H, Abe T, Kawamura H, Tsukada C, Watanabe H, Hatakeyama K, Hamada H, Nishiyama Y, Ishikawa H, Takeda K, Okumura K, Taniguchi M, Abo T. Abundance of unconventional CD8(⫹) natural killer T cells in the large intestine. Eur J Immunol 31: 3361–3369, 2001. 5. Berntman E, Rolf J, Johansson C, Anderson P, Cardell SL. The role of CD1d-restricted NK T lymphocytes in the immune response to oral infection with Salmonella typhimurium. Eur J Immunol 35: 2100 –2109, 2005. 6. Borg NA, Wun KS, Kjer-Nielsen L, Wilce MC, Pellicci DG, Koh R, Besra GS, Bharadwaj M, Godfrey DI, McCluskey J, Rossjohn J. CD1d-lipid-antigen recognition by the semi-invariant NKT T-cell receptor. Nature 448: 44 – 49, 2007. 7. Brigl M, Bry L, Kent SC, Gumperz JE, Brenner MB. Mechanism of CD1d-restricted natural killer T cell activation during microbial infection. Nat Immun 4: 1230 –1237, 2003. AJP-Gastrointest Liver Physiol • VOL 8. Brozovic S, Nagaishi T, Yoshida M, Betz S, Salas A, Chen D, Kaser A, Glickman J, Kuo T, Little A, Morrison J, Corazza N, Kim JY, Colgan SP, Young SG, Exley M, Blumberg RS. CD1d function is regulated by microsomal triglyceride transfer protein. Nat Med 10: 535–539, 2004. 9. Burdin N, Brossay L, Kronenberg M. Immunization with alpha-galactosylceramide polarizes CD1-reactive NK T cells towards Th2 cytokine synthesis. Eur J Immunol 29: 2014 –2025, 1999. 10. Cardell S, Tangri S, Chan S, Kronenberg M, Benoist C, Mathis D. CD1-restricted CD4⫹ T cells in major histocompatibility complex class II-deficient mice. J Exp Med 182: 993–1004, 1995. 11. Colgan SP, Hershberg RM, Furuta GT, Blumberg RS. Ligation of intestinal epithelial CD1d induces bioactive IL-10: critical role of the cytoplasmic tail in autocrine signaling. Proc Natl Acad Sci USA 96: 13938 –13943, 1999. 12. Croxford JL, Miyake S, Huang YY, Shimamura M, Yamamura T. Invariant V(␣)19i T cells regulate autoimmune inflammation. Nat Immun 7: 987–994, 2006. 13. Emoto M, Yoshizawa I, Emoto Y, Miamoto M, Hurwitz R, Kaufmann SH. Rapid development of a gamma interferon-secreting glycolipid/ CD1d-specific V␣14⫹ NK1.1-T-cell subset after bacterial infection. Infect Immun 74: 5903–5913, 2006. 14. Fuss IJ, Heller F, Boirivant M, Leon F, Yoshida M, Fichtner-Feigl S, Yang Z, Exley M, Kitani A, Blumberg RS, Mannon P, Strober W. Nonclassical CD1d-restricted NK T cells that produce IL-13 characterize an atypical Th2 response in ulcerative colitis. J Clin Invest 113: 1490 – 1497, 2004. 15. Ge Y, Rampy BA, Wang HL, Xiao SY. Reduced CD1d expression in colonic epithelium in microscopic colitis. Appl Immunohistochem Mol Morphol 14: 309 –313, 2006. 16. Grose RH, Cummins AG, Thompson FM. Deficiency of invariant natural killer T cells in coeliac disease. Gut 56: 790 –795, 2007. 17. Grose RH, Thompson FM, Baxter AG, Pellicci DG, Cummins AG. Deficiency of invariant NK T cells in Crohn’s disease and ulcerative colitis. Dig Dis Sci 52: 1415–1422, 2007. 18. Guy-Grand D, Cuenod-Jabri B, Malassis-Seris M, Selz F, Vassalli P. Complexity of the mouse gut T cell immune system: identification of two distinct natural killer T cell intraepithelial lineages. Eur J Immunol 26: 2248 –2256, 1996. 19. Hashimoto K, Hirai M, Kurosawa Y. A gene outside the human MHC related to classical HLA class I genes. Science 269: 693– 695, 1995. 20. Heller F, Fuss IJ, Nieuwenhuis EE, Blumberg RS, Strober W. Oxazolone colitis, a Th2 colitis model resembling ulcerative colitis, is mediated by IL-13-producing NK-T cells. Immunity 17: 629 – 638, 2002. 21. Hornung M, Farkas SA, Sattler C, Schlitt HJ, Geissler EK. DX5(⫹)NKT cells induce the death of colitis-associated cells: involvement of programmed death ligand-1. Eur J Immunol 2006. 22. Huang S, Gilfillan S, Cella M, Miley MJ, Lantz O, Lybarger L, Fremont DH, Hansen TH. Evidence for MR1 antigen presentation to mucosal-associated invariant T cells. J Biol Chem 280: 21183–21193, 2005. 23. Iiai T, Watanabe H, Suda T, Okamoto H, Abo T, Hatakeyama K. CD161⫹ T (NT) cells exist predominantly in human intestinal epithelium as well as in liver. Clin Exp Immunol 129: 92–98, 2002. 24. Illes Z, Shimamura M, Newcombe J, Oka N, Yamamura T. Accumulation of V␣7.2-J␣33 invariant T cells in human autoimmune inflammatory lesions in the nervous system. Int Immunol 16: 223–230, 2004. 25. Ishimoto Y, Tomiyama-Miyaji C, Watanabe H, Yokoyama H, Ebe K, Tsubata S, Aoyagi Y, Abo T. Age-dependent variation in the proportion and number of intestinal lymphocyte subsets, especially natural killer T cells, double-positive CD4⫹ CD8⫹ cells and B220⫹ T cells, in mice. Immunology 113: 371–377, 2004. 26. Karttunnen R, Breese EJ, Walker-Smith JA, MacDonald TT. Decreased mucosal interleukin-4 (IL-4) production in gut inflammation. J Clin Pathol 47: 1015–1018, 1994. 27. Kawachi I, Maldonado J, Strader C, Gilfillan S. MR1-restricted V␣19i mucosal-associated invariant T cells are innate T cells in the gut lamina propria that provide a rapid and diverse cytokine response. J Immunol 176: 1618 –1627, 2006. 28. Kim HS, Colgan SP, Pitman R, Hershberg RM, Blumberg RS. Human CD1d associates with prolyl-4-hydroxylase during its biosynthesis. Mol Immunol 37: 861– 868, 2000. 29. Kim HS, Garcia J, Exley M, Johnson KW, Balk SP, Blumberg RS. Biochemical characterization of CD1d expression in the absence of 2microglobulin. J Biol Chem 274: 9289 –9295, 1999. 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 memory phenotype and the ability to rapidly secret cytokines after activation (32). From their shared properties, it has been suggested that iNKT and mNKT cells might play similar roles, although in different environments (60). It could be hypothesized that the continuous presence of different endogenous or exogenous ligands presented by CD1d or MR1 guide differential iNKT and mNKT cell homing and retention. However, although iNKT and mNKT cells are enriched in different organs, it should be kept in mind that there is by no means a complete segregation of these two populations. There is evidence for a role for iNKT cells and CD1d expression in mucosal immunity and inflammation. CD1ddependent vNKT cells maybe even more prevalent and more important in humans, however, as suggested by a study of cells from patients with ulcerative colitis. By contrast, the function of mNKT cells in the intestine has yet to be established. So far, it has not been possible to produce MR1 tetramers, and the paucity of reagents for detecting and purifying mNKT cells surely has hampered progress in their study. However, given their prevalence in the lamina propria, their ability to produce effector cytokines, and their demonstrated ability to regulate inflammation in other sites including the nervous system using mouse models, it is likely that an important role for mNKT cells in mucosal immunity will be uncovered soon. G7 Themes G8 CANONICAL NKT CELLS IN MUCOSAL IMMUNITY AND INFLAMMATION AJP-Gastrointest Liver Physiol • VOL 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. vation of natural killer T cells by ␣-galactosylceramide in the presence of CD1d provides protection against colitis in mice. Gastroenterology 119: 119 –128, 2000. Shimamura M, Huang YY. Presence of a novel subset of NKT cells bearing an invariant V␣19.1-J␣26 TCR ␣ chain. FEBS Lett 516: 97–100, 2002. Shimamura M, Huang YY, Okamoto N, Suzuki N, Yasuoka J, Morita K, Nishiyama A, Amano Y, Mishina T. Modulation of V␣19 NKT cell immune responses by ␣-mannosyl ceramide derivatives consisting of a series of modified sphingosines. Eur J Immunol 37: 1836 –1844, 2007. Shimamura M, Huang YY, Okamoto N, Watanabe Y, Murakami Y, Kinoshita T, Hirabayashi Y, Murakata C, Ito Y, Ogawa T. Glycolipids with nonreducing end ␣-mannosyl residues that have the potential to activate invariant V␣19 NKT cells. FEBS J 274: 2921–2932, 2007. Shimamura M, Okamoto N, Huang YY, Yasuoka J, Morita K, Nishiyama A, Amano Y, Mishina T. Induction of promotive rather than suppressive immune responses from a novel NKT cell repertoire V␣19 NKT cell with ␣-mannosyl ceramide analogs consisting of the immunosuppressant ISP-I as the sphingosine unit. Eur J Med Chem 41: 569 –576, 2006. Smiley ST, Lanthier PA, Couper KN, Szaba FM, Boyson JE, Chen W, Johnson LL. Exacerbated susceptibility to infection-stimulated immunopathology in CD1d-deficient mice. J Immunol 174: 7904 –7911, 2005. Somnay-Wadgaonkar K, Nusrat A, Kim HS, Canchis WP, Balk SP, Colgan SP, Blumberg RS. Immunolocalization of CD1d in human intestinal epithelial cells and identification of a 2-microglobulin-associated form. Int Immunol 11: 383–392, 1999. Tilloy F, Di Santo JP, Bendelac A, Lantz O. Thymic dependence of invariant V␣14⫹ natural killer-T cell development. Eur J Immunol 29: 3313–3318, 1999. Tilloy F, Treiner E, Park SH, Garcia C, Lemonnier F, de la Salle H, Bendelac A, Bonneville M, Lantz O. An invariant T cell receptor ␣ chain defines a novel TAP-independent major histocompatibility complex class Ib-restricted ␣/ T cell subpopulation in mammals. J Exp Med 189: 1907–1921, 1999. Treiner E, Duban L, Bahram S, Radosavljevic M, Wanner V, Tilloy F, Affaticati P, Gilfillan S, Lantz O. Selection of evolutionarily conserved mucosal-associated invariant T cells by MR1. Nature 422: 164 –169, 2003. Treiner E, Duban L, Moura IC, Hansen T, Gilfillan S, Lantz O. Mucosal-associated invariant T (MAIT) cells: an evolutionarily conserved T cell subset. Microbes Infect 7: 552–559, 2005. Treiner E, Lantz O. CD1d- and MR1-restricted invariant T cells: of mice and men. Curr Opin Immunol 18: 519 –526, 2006. Tupin E, Kinjo Y, Kronenberg M. The unique role of natural killer T cells in the response to microorganisms. Nat Rev Microbiol 5: 405– 417, 2007. Ueno Y, Tanaka S, Sumii M, Miyake S, Tazuma S, Taniguchi M, Yamamura T, Chayama K. Single dose of OCH improves mucosal T helper type 1/T helper type 2 cytokine balance and prevents experimental colitis in the presence of V␣14 natural killer T cells in mice. Inflamm Bowel Dis 11: 35– 41, 2005. Van de Wal Y, Corazza N, Allez M, Mayer LF, Iijima H, Ryan M, Cornwall S, Kaiserlian D, Hershberg R, Koezuka Y, Colgan SP, Blumberg RS. Delineation of a CD1d-restricted antigen presentation pathway associated with human and mouse intestinal epithelial cells. Gastroenterology 124: 1420 –1431, 2003. Van der Vliet HJ, von Blomberg BM, Nishi N, Reijm M, Voskuyl AE, van Bodegraven AA, Polman CH, Rustemeyer T, Lips P, van den Eertwegh AJ, Giaccone G, Scheper RJ, Pinedo HM. Circulating V(␣24⫹) V11⫹ NKT cell numbers are decreased in a wide variety of diseases that are characterized by autoreactive tissue damage. Clin Immunol 100: 144 –148, 2001. Wei B, Velazquez P, Turovskaya O, Spricher K, Aranda R, Kronenberg M, Birnbaumer L, Braun J. Mesenteric B cells centrally inhibit CD4⫹ T cell colitis through interaction with regulatory T cell subsets. Proc Natl Acad Sci USA 102: 2010 –2015, 2005. West GA, Matsuura T, Levine AD, Klein JS, Fiocchi C. Interleukin 4 in inflammatory bowel disease and mucosal immune reactivity. Gastroenterology 110: 1683–1695, 1996. Wingender G, Kronenberg M. Invariant natural killer T cells in the response to bacteria: the advent of specific antigens. Future Microbiol 1: 325–340, 2006. Zhou D, Mattner J, Cantu C, Schrantz N 3rd, Yin N, Gao Y, Sagiv Y, Hudspeth K, Wu YP, Yamashita T, Teneberg S, Wang D, Proia RL, Levery SB, Savage PB, Teyton L, Bendelac A. Lysosomal glycosphingolipid recognition by NKT cells. Science 306: 1786 –1789, 2004. 294 • JANUARY 2008 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on October 28, 2016 30. Kronenberg M. Toward an understanding of NKT cell biology: progress and paradoxes. Annu Rev Immunol 23: 877–900, 2005. 31. Kronenberg M, Gapin L. Natural killer T cells: know thyself. Proc Natl Acad Sci USA 104: 5713–5714, 2007. 32. Li W, Kim MG, Gourley TS, McCarthy BP, Sant’Angelo DB, Chang CH. An alternate pathway for CD4 T cell development: thymocyteexpressed MHC class II selects a distinct T cell population. Immunity 23: 375–386, 2005. 33. Matsuda JL, Naidenko OV, Gapin L, Nakayama T, Taniguchi M, Wang CR, Koezuka Y, Kronenberg M. Tracking the response of natural killer T cells to a glycolipid antigen using CD1d tetramers. J Exp Med 192: 741–754, 2000. 34. Michel ML, Keller AC, Paget C, Fujio M, Trottein F, Savage PB, Wong CH, Schneider E, Dy M, Leite-de-Moraes MC. Identification of an IL-17-producing NK11(neg) iNKT cell population involved in airway neutrophilia. J Exp Med 204: 995–1001, 2007. 35. Miley MJ, Truscott SM, Yu YY, Gilfillan S, Fremont DH, Hansen TH, Lybarger L. Biochemical features of the MHC-related protein 1 consistent with an immunological function. J Immunol 170: 6090 – 6098, 2003. 36. Miyamoto K, Miyake S, Yamamura T. A synthetic glycolipid prevents autoimmune encephalomyelitis by inducing TH2 bias of natural killer T cells. Nature 413: 531–534, 2001. 37. Mizoguchi A, Mizoguchi E, Takedatsu H, Blumberg RS, Bhan AK. Chronic intestinal inflammatory condition generates IL-10-producing regulatory B cell subset characterized by CD1d upregulation. Immunity 16: 219 –230, 2002. 38. Numata Y, Tazuma S, Ueno Y, Nishioka T, Hyogo H, Chayama K. Therapeutic effect of repeated natural killer T cell stimulation in mouse cholangitis complicated by colitis. Dig Dis Sci 50: 1844 –1851, 2005. 39. Ohteki T, MacDonald HR. Major histocompatibility complex class I related molecules control the development of CD4⫹8- and CD4 – 8subsets of natural killer 1.1⫹ T cell receptor-␣/⫹ cells in the liver of mice. J Exp Med 180: 699 –704, 1994. 40. Okamoto N, Kanie O, Huang YY, Fujii R, Watanabe H, Shimamura M. Synthetic ␣-mannosyl ceramide as a potent stimulant for an NKT cell repertoire bearing the invariant V␣19-J␣26 TCR ␣ chain. Chem Biol 12: 677– 683, 2005. 41. O’Keeffe J, Doherty DG, Kenna T, Sheahan K, O’Donoghue DP, Hyland JM, O’Farrelly C. Diverse populations of T cells with NK cell receptors accumulate in the human intestine in health and in colorectal cancer. Eur J Immunol 34: 2110 –2119, 2004. 42. Page MJ, Poritz LS, Tilberg AF, Zhang WJ, Chorney MJ, Koltun WA. Cd1d-restricted cellular lysis by peripheral blood lymphocytes: relevance to the inflammatory bowel diseases. J Surg Res 92: 214 –221, 2000. 43. Panja A, Blumberg RS, Balk SP, Mayer L. CD1d is involved in T cell-intestinal epithelial cell interactions. J Exp Med 178: 1115–1119, 1993. 44. Park SH, Benlagha K, Lee D, Balish E, Bendelac A. Unaltered phenotype, tissue distribution and function of V␣14(⫹) NKT cells in germ-free mice. Eur J Immunol 30: 620 – 625, 2000. 45. Pellicci DG, Hammond KJ, Coquet J, Kyparissoudis K, Brooks AG, Kedzierska K, Keating R, Turner S, Berzins S, Smyth MJ, Godfrey DI. DX5/CD49b-positive T cells are not synonymous with CD1d-dependent NKT cells. J Immunol 175: 4416 – 4425, 2005. 46. Perera L, Shao L, Patel A, Evans K, Meresse B, Blumberg R, Geraghty D, Groh V, Spies T, Jabri B, Mayer L. Expression of nonclassical class I molecules by intestinal epithelial cells. Inflamm Bowel Dis 13: 298 –307, 2007. 47. Porubsky S, Speak AO, Luckow B, Cerundolo V, Platt FM, Grone HJ. Normal development and function of invariant natural killer T cells in mice with isoglobotrihexosylceramide (iGb3) deficiency. Proc Natl Acad Sci USA 104: 5977–5982, 2007. 48. Ranson T, Bregenholt S, Lehuen A, Gaillot O, Leite-de-Moraes MC, Herbelin A, Berche P, Di Santo JP. Invariant V␣ 14⫹ NKT cells participate in the early response to enteric Listeria monocytogenes infection. J Immunol 175: 1137–1144, 2005. 49. Ronet C, Darche S, Leite de Moraes M, Miyake S, Yamamura T, Louis JA, Kasper LH, Buzoni-Gatel D. NKT cells are critical for the initiation of an inflammatory bowel response against Toxoplasma gondii. J Immunol 175: 899 –908, 2005. 50. Saubermann LJ, Beck P, De Jong YP, Pitman RS, Ryan MS, Kim HS, Exley M, Snapper S, Balk SP, Hagen SJ, Kanauchi O, Motoki K, Sakai T, Terhorst C, Koezuka Y, Podolsky DK, Blumberg RS. Acti-