Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Serotonin syndrome wikipedia , lookup
Asperger syndrome wikipedia , lookup
Microneurography wikipedia , lookup
Rett syndrome wikipedia , lookup
Neuropharmacology wikipedia , lookup
Marfan syndrome wikipedia , lookup
Down syndrome wikipedia , lookup
Werner syndrome wikipedia , lookup
Guillain–Barré syndrome wikipedia , lookup
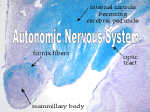
Vet Times The website for the veterinary profession http://www.vettimes.co.uk SYMPATHETIC ROUTE TO HORNER’S SYNDROME: SIGNS AND DIAGNOSIS Categories : Vets Date : April 11, 2011 Elena Scarpante and Victoria Doyle discuss a common condition in cats and dogs, using MRI scans to highlight lesions and softtissue infl ammation consistent with its cause Summary Horner’s syndrome (HS) is a common neurological syndrome that occurs due to the loss of sympathetic innervation to the eye. The clinical signs include miosis, ptosis of the upper eyelid, decreased tone in the lower eyelid, protrusion of the third eyelid and enophthalmos. Horner’s syndrome can be classified as first order, second order (preganglionic) or third order (postganglionic) according to the anatomical location of the lesion. Localisation of the lesion requires information from the clinical, neurological and ophthalmic examinations to be used in conjunction with pharmacologic testing. Based on this information, further diagnostic tests can be performed to identify the underlying cause. Key words cat, dog, Horner’s syndrome, idiopathic, sympathetic, innervation to the eye HORNER’S syndrome (HS) is a common neurological condition seen in both cats and dogs. It occurs due to lesions affecting the sympathetic supply to the eye. The aims of this article are to describe: • the anatomy of the sympathetic supply to the eye; 1/5 • the clinical signs associated with Horner’s syndrome; • the common differential diagnoses for this condition; and • the further diagnostic tests that are indicated. Anatomy The pathway that provides the sympathetic innervation to the eye consists of three neurons. The cell bodies of the first order neurons are located in the hypothalamus and rostral midbrain. The axons pass caudally through the brainstem and in the lateral part of the cervical spinal cord (tectotegmental spinal tract) to reach the first three thoracic spinal cord segments (T1-3). Here, the first order neurons synapse on the cell bodies of the second order neurons (preganglionic neurons) located in the intermediolateral grey column of the spinal cord. The second order neurons exit the spinal canal through the intervertebral foramina together with the ventral nerve root arising from the first three thoracic spinal cord segments (T1-3). The axons of the second order neurons leave the spinal nerve as the ramus communicans and join the thoracic sympathetic trunk. The thoracic sympathetic trunk courses inside the thorax ventrolateral to the vertebral bodies and runs cranially along the neck, associated with the vagus nerve forming the vagosympathetic trunk within the carotid sheath. The axons of the second order neurons travel rostrally to the cranial cervical ganglion, which is located ventromedially to the tympanic bulla. At the level of the cranial cervical ganglion the axons of the second order neurons synapse on the cell bodies of the third order neurons (postganglionic neurons). From the cranial cervical ganglion, the postganglionic neurons project through the ventral part of the tympanic bulla and enter the cranial cavity through the tympano-occipital fissure together with the carotid artery and glossopharyngeal nerve (CN IX). Within the cranial cavity the axons travel rostrally adjacent to the middle cranial fossa. The postganglionic fibres then exit the cranial cavity through the orbital fissure with the ophthalmic branch of the trigeminal nerve to innervate the smooth muscle of the eyelids (including third eyelid), orbit and iris dilator muscles. The sympathetic innervation also supplies the smooth muscles of the ). blood vessels to the head (Figure 1 Clinical signs The loss of sympathetic innervation of the eye causes a combination of clinical signs, which are collectively referred to as HS. They include ipsilateral miosis, ptosis of the upper eyelid, decreased 2/5 tone in the lower eyelid, protrusion of the third eyelid and enophthalmos (Figures 2 and 3). No visual deficits are directly associated to damage along the sympathetic pathway to the eye, but vision might be obscured in a case of bilateral HS, due to the prominent third eyelid protrusion. Partial HS can also be seen. This usually consists of only the presence of miosis (Figure 4) and is most commonly observed with lateralised cervical lesions in dogs. On clinical examination the anisocoria is more pronounced when examined in a darkened room. Enophthalmos can be best appreciated by viewing the patient from above. In dogs the protrusion of the third eyelid occurs passively as a consequence of enophthalmos, whereas in the cat the third eyelid has a small amount of smooth muscle, which is innervated by the sympathetic supply to the eye. Therefore, in cats with HS the third eyelid protrusion is partly due to the loss of innervation to the smooth muscle of the third eyelid preventing it from being retracted, as well as the presence of enophthalmos. In addition to the signs related to the eye and the orbital smooth muscle, the paralysis of the sympathetic supply to the head causes a peripheral vasodilation that may be shown by increased warmth and hyperaemia of the pinna, as well as congestion of the scleral vessels and nasal mucosa ipsilaterally. A fundic exam may show congested retinal blood vessels. Reduced sweating (anhidrosis), usually on the ipsilateral nostril, is also possible. However, these signs are not commonly detected in small animals. The sympathetic supply to the eye is a very long pathway and damage anywhere along its route can cause HS. HS is classified as first, second and third order. Damage to the sympathetic supply to the eye due to a lesion anywhere between the hypothalamus and the T1-3 spinal cord segments can cause damage to the first order neuron (Figures 5 and 6). Damage to the sympathetic supply from the cell bodies in the intermediate grey matter of T1-3 spinal cord segments to the tympanic bulla will cause a second order (preganglionic) HS (Figures 7 and 8). Damage to the sympathetic supply anywhere between the tympanic bulla and the eye will cause a third order (postganglionic) HS (Figures 9 and 10). Differential diagnoses for the first, second and third order HS and the associated clinical signs are listed in Table 1. Diagnosis A full history, clinical, ophthalmological and neurological examinations are required in any patient presenting with HS. Pharmacological testing using topical one per cent phenylephrine may be used to aid the classification of the HS (first, second or third). 3/5 After topical administration of one per cent phenylephrine (sympathomimetic) to both eyes simultaneously, the time for the mydriasis to occur is recorded (Table 2). The phenylephrine test is based on the principle of denervation hypersensitivity, which takes approximately two weeks to develop. According to this phenomenon, the smooth muscles increase their sensitivity to neurotransmitters (norepinephrine) following denervation. The shorter the time for the pupil to dilate, the closer the lesion is to the iris. The test is not 100 per cent reliable and should be interpreted in light of the other clinical signs. Based on the history, clinical, ophthalmological and neurological findings and result of the pharmacological test further investigations can be planned (Table 3). Treatment and prognosis of the most common causes of HS The prognosis is closely related to the underlying disease process (Table 1). Conclusion The sympathetic supply to the eye is extremely long and, therefore, lesions at many different anatomical locations from a variety of pathologies can cause HS. Consequently, it is important to interpret the results of clinical, neurological and pharmacological tests to localise the lesion before embarking on the diagnostic investigation. In this way an accurate diagnosis can be made and any required treatment can be instituted expediently. • The authors would like to thank Alberta de Stefani for her support and supervision. References Barlow C M and Root W S (1949). The ocular sympathetic path between the superior cervical ganglion and the orbit in the cat, J Comp Neurol 91: 195. Bosmans T, Schauvliege S, Gasthuys F, Marcilla M G and Polis I (2009). Transient unilateral Horner’s syndrome after epidural ropivacaine in a dog, Vet Anaesth Analg 36(4): 401-406. Boydell P (1995). Idiopathic Horner’s syndrome in the golden retriever, J Small Anim Prac 36: 382-384. Boydell P (2000). Idiopathic Horner’s syndrome in golden retrievers, J Neuro Ophthalmol 20(4): 288-290. De Lahunta A and Glass E (2009). Lower motor neuron – general visceral efferent system. In De Lahunta A and Glass E (eds) Veterinary Neuroanatomy and Clinical Neurology (3rd edn), Saunders: 173-180. De Risio L and Fraser McConnell J (2009). Second order Horner’s syndrome in a cat, J Feline Med Surg 11(8): 714-716. 4/5 Kern T J, Aromando M C and Erb H N (1989). Horner’s syndrome in dogs and cats: 100 cases (1975-1985), J Am Vet Med Assoc 195: 369-373. Krotscheck U, Kunze C P and Bergman R L (2004). What is your diagnosis? Horner syndrome, J Am Vet Med Assoc 225(9): 1,337-1,338. Morgan R V and Zanotti W (1989). Horner’s syndrome in dogs and cats: 49 cases (1980-1986), J Am Vet Med Ass 194: 196-199. Penderis J (2004). Disorders of the eyes and vision. In Platt S R and Olby N J (eds). BSAVA Manual of Canine and Feline Neurology (3rd edn) BSAVA, Gloucester: 138-139, 144-145. Ron Ofri (2009). Neuro-ophthalmology. In Slatter’s Fundamentals of Veterinary Ophthalmology (4th edn) Saunders: 336-339. Van den Broek A H M (1987). Horner’s syndrome in cats and dogs: a review, J Small Anim Pract 28: 929-940. 5/5 Powered by TCPDF (www.tcpdf.org)