Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
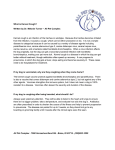
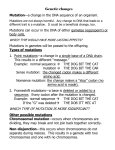
Molecular Genetics and Metabolism 112 (2014) 302–309 Contents lists available at ScienceDirect Molecular Genetics and Metabolism journal homepage: www.elsevier.com/locate/ymgme A CLN8 nonsense mutation in the whole genome sequence of a mixed breed dog with neuronal ceroid lipofuscinosis and Australian Shepherd ancestry Juyuan Guo a, Gary S. Johnson a, Holly A. Brown b, Michele L. Provencher c, Ronaldo C. da Costa c, Tendai Mhlanga-Mutangadura a, Jeremy F. Taylor d, Robert D. Schnabel d, Dennis P. O'Brien a, Martin L. Katz e,⁎ a Department of Veterinary Pathobiology, University of Missouri College of Veterinary Medicine, Columbia, MO, USA Metz Petz Veterinary Clinic at Shawnee, Lima, OH, USA c Department of Veterinary Clinical Sciences, The Ohio State University College of Veterinary Medicine, Columbus, OH, USA d Division of Animal Science, University of Missouri College of Agriculture, Food and Natural Resources, Columbia, MO, USA e Mason Eye Institute, University of Missouri School of Medicine, Columbia, MO, USA b a r t i c l e i n f o Article history: Received 1 May 2014 Received in revised form 28 May 2014 Accepted 28 May 2014 Available online 4 June 2014 Keywords: Batten disease Dog model CLN8 mutation Lysosomal storage disease Retina Brain a b s t r a c t The neuronal ceroid lipofuscinoses (NCLs) are hereditary neurodegenerative diseases characterized by seizures and progressive cognitive decline, motor impairment, and vision loss accompanied by accumulation of autofluorescent lysosomal storage bodies in the central nervous system and elsewhere in the body. Mutations in at least 14 genes underlie the various forms of NCL. One of these genes, CLN8, encodes an intrinsic membrane protein of unknown function that appears to be localized primarily to the endoplasmic reticulum. Most CLN8 mutations in people result in a form of NCL with a late infantile onset and relatively rapid progression. A mixed breed dog with Australian Shepherd and Blue Heeler ancestry developed neurological signs characteristic of NCL starting at about 8 months of age. The signs became progressively worse and the dog was euthanized at 21 months of age due to seizures of increasing frequency and severity. Postmortem examination of the brain and retinas identified massive accumulations of intracellular autofluorescent inclusions characteristic of the NCLs. Whole genome sequencing of DNA from this dog identified a CLN8:c.585GNA transition that predicts a CLN8:p.Trp195* nonsense mutation. This mutation appears to be rare in both ancestral breeds. All of our 133 archived DNA samples from Blue Heelers, and 1481 of our 1488 archived Australian Shepherd DNA samples tested homozygous for the reference CLN8:c.585G allele. Four of the Australian Shepherd samples tested heterozygous and 3 tested homozygous for the mutant CLN8:c.585A allele. All 3 dogs homozygous for the A allele exhibited clinical signs of NCL and in 2 of them NCL was confirmed by postmortem evaluation of brain tissue. The occurrence of confirmed NCL in 3 of 4 CLN8:c.585A homozygous dogs, plus the occurrence of clinical signs consistent with NCL in the fourth homozygote strongly suggests that this rare truncating mutation causes NCL. Identification of this NCL-causing mutation provides the opportunity for identifying dogs that can be used to establish a canine model for the CLN8 disease (also known as late infantile variant or late infantile CLN8 disease). © 2014 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/). 1. Introduction The neuronal ceroid lipofuscinoses (NCLs) are inherited progressive neurodegenerative disorders characterized by accumulations of autofluorescent lysosomal storage material in the central nervous system as well as in many other organs and tissues [1,2]. Among the symptoms of NCL are progressive cognitive decline and loss of motor functions, seizures, and vision loss. The NCLs vary in age at onset of neurological signs from infancy to adulthood, as well as in rates of disease progression and ⁎ Corresponding author at: Mason Eye Institute, School of Medicine, University of Missouri, One Hospital Dr., Columbia, MO 65212, USA. Fax: +1 573 884 4100. E-mail address: [email protected] (M.L. Katz). severity [1,2]. The majority of the NCLs have childhood onsets and are ultimately fatal. The genetic bases of most cases of NCL have been identified and include a variety of mutations in at least 14 different genes [3]. Some of these genes encode soluble lysosomal enzymes of known function, but the functions and even the subcellular localization of other NCL proteins are unknown or are poorly understood. In addition to occurring in people, naturally occurring NCLs have been identified in many other species including cattle, sheep, cats and dogs [1,2]. Canine genes harboring NCL-causing mutations have been identified in American Bulldogs (CTSD), Australian Shepherds (CLN6), Border Collies (CLN5), English Setters (CLN8), American Staffordshire Terriers (ARSG), Tibetan Terriers (ATP13A2), and Dachshunds (both TPP1 and PPT1) [4–10]. Mutations in the human orthologs of all these http://dx.doi.org/10.1016/j.ymgme.2014.05.014 1096-7192/© 2014 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/). J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 genes except ARSG are known to cause NCL in people. The canine disorders can serve as NCL models for studying disease pathogenesis and for evaluating therapeutic interventions. For example, evaluation of enzyme replacement therapy in Dachshunds with a TPP1 null mutation laid the groundwork for a human clinical trial to determine the efficacy of this approach in children with NCL resulting from mutations in the orthologous gene [5]. Because of the potential value of canine models for developing treatments for the NCLs, we undertake studies to determine whether dogs exhibiting clinical signs that may be indicative of NCL harbor mutations in any of the known NCL genes. One such dog of mixed Australian Shepherd and Blue Heeler ancestry was recently reported to us. Studies were undertaken to confirm that this dog suffered from NCL and to identify the causative mutation. 2. Materials and methods 303 therapeutic range, the dog's anxiety continued to worsen and by 51 days post-presentation the dog was exhibiting progressively more frequent and severe seizure activity that was not ameliorated by Diazepam administration. As a result of the intractable seizures, the dog was euthanized at this time. The affected dog was conceived from a breeding between two littermates (Fig. 1) one of whose parents was an Australian Shepherd and the other of which was a Blue Heeler (breed also referred to as Australian Cattle Dog). The owners of both the grandparents and parents of the affected dog were unwilling to provide DNA samples from their dogs and we were unable to locate littermates of the affected dog. 2.2. Magnetic resonance imaging The patient's brain was imaged with a 3 T Philips magnetic resonance imaging instrument (Achieva, Cleveland OH). Several sequences 2.1. Subject dog — clinical signs and ancestry A 20 month old 26.3 kg spayed female dog with mixed Australian Shepherd/Blue Heeler ancestry presented to Metz Petz Veterinary Clinic after a 3 week history of severe vision loss culminating in blindness. The owners noted that since puppyhood the dog had exhibited signs of visual impairment characterized by difficulty in catching and locating tossed treats and bumping into objects, even under bright light conditions. The owners reported that over a period of 10 to 12 months prior to presentation the affected dog exhibited a loss of housetraining, decreased responsiveness to voice commands, and increased sensitivity to noises. She also exhibited compulsive circling and pacing behavior and a loss of the ability to navigate stairs. The dog became progressively more ataxic and exhibited periods of trance-like staring behavior. At presentation, the patient was very anxious. She lacked a menace response in both eyes. Pupillary light responses, both direct and consensual, were normal in both eyes, and dazzle reflexes were positive in both eyes. The rest of her cranial nerve and physical examination were within normal limits. The pet was referred to the Ohio State University (OSU) Veterinary Medical Center. While being transported the patient began exhibiting signs of focal seizures with fly biting behavior, pawing at her face, shaking her head, falling, and biting the air near her flank region. Ophthalmic examination revealed no retinal abnormalities upon fundic examination and normal tear film production and intraocular pressures. Electroretinogram responses were within normal limits. Within 24 h of presentation, the patient became very aggressive with progressive seizure activity and high pitched barking. She presented to an emergency clinic overnight and was started on Phenobarbital IV. The patient continued to exhibit seizure activity laying in lateral recumbency and paddling the following day. She presented to the OSU Neurology Service 48 h after the initial clinical presentation for examination, magnetic resonance imaging (MRI) and spinal cerebrospinal fluid collection and analysis. A complete neurologic examination revealed inappropriately anxious behavior, with absent menace responses, and decreased proprioceptive positioning bilaterally in both pelvic limbs. The remainder of the neurologic examination was normal. The complete blood chemistry analysis was unremarkable with only mild alanine aminotransferase elevation. No abnormalities were observed in the analysis of the cerebrospinal fluid. MRI revealed diffuse brain atrophy but no localized lesions. To ameliorate seizure activity, treatment with Phenobarbital was continued. She did well at home initially with no seizures but was dragging her feet more, stumbling, and had difficulty keeping her balance to urinate and defecate. The patient was polyuric, polydipsic, with an increased appetite — known effects of phenobarbital administration. At 27 days after initial presentation, the dog was again brought in for evaluation due to increased anxiety, decreased responsiveness to sound stimuli, and severe behavioral changes including aggression, disorientation, and ataxia. Despite blood levels of phenobarbital being within the Fig. 1. (A) Littermates produced by breeding between an Australian Shepherd and a Blue Heeler. A breeding between the dogs shown in (A) produced the dog shown in (B) that was characterized in this study. 304 J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 were obtained including T2- and T1-weighted images (pre- and postcontrast administrations) in the sagittal, transverse and dorsal planes. Additionally FLAIR (fluid attenuated inversion recovery) and gradient echo sequences were obtained in the transverse plane. Slice thickness was 3 mm for all sequences with no interslice interval. 2.3. Histopathology and electron microscopy The affected dog was euthanized at approximately 20 months of age due to intractable seizures. The eyes were enucleated and the corneas were removed before placing one of the globes in EM fixative (2% glutarladehyde, 1.12% paraformaldehyde, 130 mM sodium cacodylate, 1 mM CaCl2, pH 7.4) and the other in immuno fixative (0.05% glutaraldehyde, 3.5% paraformaldehyde, 120 mM sodium cacodylate, 1 mM CaCl2, pH 7.4). The brain was then removed from the skull. Slices of the cerebral cortex parietal lobe and of cerebellum were each placed in vials of the same fixatives. The remainder of the brain was placed in 10% phosphate-buffered formalin (Fisher Scientific SF93-4, Fair Lawn, NJ). After approximately 24 h at room temperature, the immuno-fixed samples of cerebral cortex and cerebellum were transferred to 170 mM sodium cacodylate, pH 7.4, in which they were stored at 4 °C until further processing. At the same time, the irises, lenses and vitreous bodies were removed from the eyes, the remainders of which were then incubated for another 24 h in the fixatives. The immuno-fixed eyecup was then transferred to 170 mM sodium cacodylate, pH 7.4, and stored at 4 °C until further processing. The EM-fixed tissues were incubated at room temperature for at least 48 h and then stored in the fixative at 4 °C until further processing. After incubation at room temperature for approximately 48 h, the formalin-fixed portion of the brain was stored at 4 °C until further processing. Slices of the immuno-fixed cerebral cortex, cerebellum, and retina from the posterior pole of the immuno-fixed eye were processed, embedded and frozen for cryostat sectioning as previously described [11]. Cryostat sections of each of these tissues were cut at a thickness of 8 μm, mounted on Superfrost Plus slides (Fisher Scientific, Fair Lawn, NJ) in 170 mM sodium cacodylate. The sections were examined and photographed using fluorescence microscopy as previously described [11]. After at least 48 h of incubation at room temperature, pieces of the EM-fixed cerebral cortex, cerebellum, and retina from the posterior pole of the EM-fixed eye were post-fixed and embedded in epoxy resin. Sections of the embedded tissue were cut on an ultramicrotome at thicknesses of 0.5 to 0.8 μm, mounted on glass slides and stained with toluidine blue. Areas of interest were identified by microscopic examination of these sections, and the blocks were trimmed to remove tissue from outside the areas of interest. Sections were then obtained from the trimmed blocks at thicknesses of 70 to 90 nm. The latter sections were mounted on 200 mesh copper thin-barred grids, stained with uranyl acetate and lead citrate, and were then examined and photographed using a JEOL 1400 transmission electron microscope. Slices of the formalin-fixed cerebellum were embedded in paraffin. For comparison, similar slices of cerebellum from two one-year-old normal Beagles were collected, fixed in formalin, and embedded in paraffin. Four μm-thick sections of these tissues were mounted on positively charged glass slides, deparaffinized, and immunostained with an antibody directed against glial fibrillary acid protein (GFAP). For immunolabeling, the slide-mounted sections were steam treated in a decloaking chamber (Biocare Medical, Concord, CA) at 98 °C for 30 min in citrate target retrieval solution (Dako, Carpinteria, CA), cooled at room temperature for 10 min, rinsed with distilled water, then placed on an IntelliPATH FLX autostainer for staining. Slides were treated with 3% H2O2 for 15 min, washed in buffer, and treated with Sniper block (Biocare Medical) for 20 min. They were then incubated in primary antibody (rabbit anti-GFAP, DakoCytomation, product # Nr.Z 0334) for 60 min. Control sections were treated with nonimmune rabbit IgG (Sigma, St. Louis, MO) at a 1:1000 dilution for 60 min in place of the primary antibody. The detection system was a rabbit anti-goat horse radish peroxidase (HRP) kit (PK6105; Biocare Medical) with 30-min incubations in link and label steps followed by a Tris-buffered rinse. The sections were then incubated in romulin red (Biocare Medical) for 10 min. Slides were counterstained in hematoxylin (Biocare Medical) at a 1:10 dilution for 5 min followed by a Tris-buffered rinse, dehydrated, coverslipped, and then imaged with light microscopy. 2.4. Molecular genetic analyses A DNA sample from the affected dog was used with the Illumina TruSeq DNA PCR-Free Sample Preparation Kit to prepare 2 paired-end libraries: one with a fragment size of approximately 350 bp and the other with a fragment size of approximately 550 bp. The 2 libraries were sequenced with an Illumina HiSeq 2000 sequencer at the University of Missouri DNA Core Facility. Adapter sequences were trimmed from the sequence reads with custom Perl scripts and the adaptertrimmed reads were error corrected using MaSuRCA v1.9.5 software [12]. NextGENe software (Soft Genetics) was used to align the error corrected reads to the CanFam3.1 reference genome assembly and to categorize sequence variants. Variant calls were further processed using custom Perl scripts to remove likely false positives. The remaining sequence variants were uploaded to a custom PostgreSQL database which contained the variant calls for an additional 101 canid samples. These control whole genome sequences included: 43 genomes from our group; 15 wild canid genomes provided by the University of California, Los Angeles; 28 genomes from the Institute for Translational Genomic Research; 10 genomes provided by investigators at North Carolina State University; and, 5 genomes provided by investigators at the University of Pennsylvania. Custom SQL scripts were used to identify variants that fit an autosomal recessively inherited rare disease model such that the case is homozygous for an allele not observed in either heterozygous or homozygous state in any of the similarly generated 101 canid whole genome sequences in our data set. The candidate variant list was further filtered to include only variants predicted to alter the primary structure of gene products. A detailed description of the data processing pipeline is in preparation and will be published elsewhere. An apparent CLN8:c.585GNA sequence variant (GenBank accession NM_001012343) was verified by PCR amplification with primers 5′GGCAGTAAGTCTTCCTCAAAGTG-3′ and 5′-TGCTGACCAGACCGTCCCA-3′ and automated Sanger sequencing. A TaqMan allelic discrimination assay [13] was used to genotype DNA samples from individual dogs at CLN8:c.585G NA. For this assay, the PCR primer sequences were 5′GGTCCGAGTCTCTGTTTTGGAA-3′ and 5′-CGGCAGTGGAACATGTGGAT-3′ and the competing probes were 5′-VIC-TGAACCAGTGGCTGATG-MGB-3′ (reference allele) and 5′-FAM-TGAACCAGTGACTGATG-MGB-3′ (mutant allele). 3. Results 3.1. Magnetic resonance imaging T-2 weighted MR imaging of the brain revealed ventriculomegaly, as well as abnormally prominent cortical sulci (Fig. 2). The folia of the cerebellum were also abnormally prominent. No localized brain lesions were observed. 3.2. Histopathology and electron microscopy A defining feature of the NCLs is the accumulation of autofluorescent lysosomal storage material in the central nervous system as well as in many nonneuronal tissues and organs [1,2]. Unless the causative mutation is known and can be screened for, the only way to definitively diagnose NCL in a dog exhibiting signs of these disorders is to examine J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 305 neural tissues for the presence of this autfluorescent material. In the dog that was evaluated for this study, massive amounts of autofluorescent material with the fluorescence spectral characteristics of NCL-specific storage substance were observed in the cerebellum, cerebral cortex, and retina (Fig. 3). The storage bodies that accumulated in the brain and retina consisted of membrane-bounded intracellular inclusion bodies (Fig. 4). The most prominent feature of the contents of these inclusion bodies from all cell types examined were multilamellar structures composed of stacks of membrane-like rectilinear structures (Fig. 4). A minor component of the storage bodies in the retinal ganglion cells had a curvilinear appearance (Fig. 4C). The storage bodies along the retinal outer limiting membrane appeared to be present primarily in the Mueller cells. The NCLs are characterized by astrogliosis throughout the central nervous system as demonstrated by the presence of large numbers of astrocytes that exhibit immunohistochemical staining for GFAP [14–17]. GFAP immunohistochemical staining of the cerebellum from the affected dog revealed the presence of a dramatically larger number of GFAP-positive cells, primarily in the medulla, than were present in the same brain areas of two normal one-year-old Beagles that were examined (Fig. 5). In those cells that did exhibit GFAP immunostaining in the cerebellums of the normal dogs, the staining intensity was much lower than in cells from the same region of the cerebellum of the affected dog (Fig. 5). 3.3. CLN8 mutation identification Fig. 2. T2 weighted MRI in the sagittal (A), dorsal (B) and transverse (C) planes from the affected dog. Cerebrospinal fluid (CSF) is white and brain parenchyma gray. Diffuse brain atrophy is indicated by increased CSF surrounding the folia of the cerebellum (A arrow), enlargement of the lateral ventricles (B & C asterisks), and widening of the sulci of the cerebral cortex (B & C arrowheads). DNA from the NCL-affected dog was used to generate a 20-fold average coverage whole genome sequence which contained 6.1 million sequence variants (differences from the canine genome reference sequence). Of these, 83 sequence variants remained after filtering to retain only the variants that were homozygous in the target sequence, predicted to alter the amino acid sequence of the gene product, and absent from 101 other canid whole genome sequences (Table S1). Among Fig. 3. Fluorescence micrographs of cryostat sections of the cerebellum (A), parietal lobe of the cerebral cortex (B), and the retina (C). Accumulation of autofluorescent storage material was abundant in all 3 tissues. In the cerebellum the Purkinje cells (PC) showed the most pronounced accumulation of storage material. In the retina autofluorescent storage material content was most abundant in the ganglion cells (GC), along the outer limiting membrane (OLM), and in the retinal pigment epithelium (RPE). Bar in (B) indicates magnification for panels (A) and (B). 306 J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 Fig. 4. Electron micrographs of the storage material from a cerebellar Purkinje cell (A), a cerebral cortical neuron (B), a retinal ganglion cell (C), and a cell adjacent to the retinal outer limiting membrane (D). these 83 sequence variants, a CLN8:c.585GNA transition that predicts a CLN8:p.Trp195* nonsense mutation (Fig. 6A) was considered most likely to be causal because it was the only variant in a canine ortholog of a gene associated with human NCL and because it is predicted to encode a truncated protein missing the 93 C-terminal amino acids. The CLN8: c.585GNA transition was verified by automated Sanger sequencing (Fig. 6B). Since the affected dog was a member of the F2 generation from an Australian Shepherd crossed with a Blue Heeler, we genotyped archived DNA samples from each breed to identify the most likely source of the CLN8 nonsense mutation. All of our 133 DNA samples from Blue Heelers tested homozygous for the reference CLN8:c.585G allele. Of our 1488 Australian Shepherd samples, 1481 tested homozygous for the CLN8:c.585G allele, 4 were heterozygous, and 3 tested homozygous for the mutant CLN8:c.585A allele. One of the CLN8:c.585A homozygous DNA samples came from an Australian Shepherd with a history of seizures. No postmortem histopathological data are available from that dog. The other two DNA samples had been extracted from paraffin embedded formalin-fixed brain from NCL-affected littermates characterized in an earlier study [18]. 4. Discussion We investigated a mixed-breed dog with a progressive neurodegenerative disease and a medical history that included blindness, seizures, cognitive decline, behavioral changes, ataxia, and brain atrophy similar to the disease signs seen in human and in other canine NCLs [1,2]. In addition to these signs, the presence of autofluorescent cytoplasmic inclusions in unstained sections of the dog's brain and retina and astrogliosis in the cerebellum supported a diagnosis of NCL [4,5,7,9,10, 19,20]. Storage material with similar fluorescence properties (lipofuscin) accumulates in many postmitotic cells during normal aging, but the amount of this material in the brain and retina of the young affected dog was dramatically higher than would have accumulated as a result of aging alone. In the retina, lipofuscin normally accumulates only in the RPE; the presence of autofluorescent material in the ganglion and Mueller cells and elsewhere in the neural retina is diagnostic of NCL [5,9,19,21]. In addition, the mulitlamellar rectilinear ultrastructural features of the storage material in the affected dog brain are similar to those of the storage materials that accumulate in the cells of human subjects with some late infantile forms of NCL [22–25] and does not contain lipid-like components that are typical of lipofuscin [26]. The lamellar appearance of material within the storage bodies is suggestive of membrane fragments which may not be properly degraded in this disease. Because the canine NCLs are rare recessive diseases, we searched the whole genome sequence from the affected dog for homozygous sequence variants that were predicted to alter the amino acid sequences of the gene products but absent from the whole genome sequences of 101 control canids. Among the 83 sequence variants that met these criteria, the only one that involved an ortholog of a gene associated with human NCL was CLN8:c.585GNA, which predicts a nonsense mutation, p.Trp195*. The function of CLN8, the protein encoded by CLN8, has not been clearly identified, although there is some evidence that CLN8 may be involved in ceramide biosynthesis [27] and vesicular and membrane trafficking [28]. CLN8 appears to be an intrinsic membrane protein localized primarily to the endoplasmic reticulum (ER) and ERGolgi intermediate compartment [29]. It belongs to a family that includes 15 other mammalian proteins encoded by CLN8 paralogs, each containing a TRAM-LAG-CLN8 (TLC) domain comprised of 5 putative transmembrane helices [30,31]. The CLN8:c.585GNA transition predicts a CLN8:p.Trp195* nonsense mutation and a truncated protein product J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 Fig. 5. GFAP immunostained sections of the cerebellar white matter (medulla) from a oneyear-old normal Beagle (A) and from the dog with NCL (B). The density of GFAP-positive cells and the amount GFAP staining per cell was much higher in the affected dog than in the dog that did not suffer from NCL. missing the 93 C-terminal amino acids. Truncated CLN8 is unlikely to be functional because it lacks 2 of the 5 predicted transmembrane helicies of the TLC domain. A potentially functional C-terminal endoplasmic retriculum retrieval signal [29] is also predicted to be missing from the truncated CLN8. Even missense mutations both within and outside of the TLC domain of CLN8 result in late infantile onset NCL in people [32], so it is unlikely that the nonsense mutation observed in the 307 affected dog would be benign and very likely that it is the molecular genetic cause of the dog's NCL. Our assertion that the homozygous CLN8:c.585A allele is a cause of canine NCL was further supported when we genotyped more than 1600 archived Australian Shepherd and Blue Heeler DNA samples at CLN8:c.585. Only 3 of these samples were from c.585A homozygous dogs. Little is known about the clinical history of one of these dogs except that it had recurrent seizures (a prominent clinical sign of the mixed breed dog). The other two CLN8:c.585A homozygous samples were extracted from formalin-fixed brains that were collected from Australian Shepherd littermates with well-documented NCL of unknown etiology [18]. The clinical histories and neuropathologic lesions of the Australian Shepherd littermates were almost identical to those of the mixed-breed dog reported here. Thus, 3 of the 4 dogs known to be homozygous for the rare CLN8 nonsense mutation also shared a rare clinical condition (and the fourth dog had a scant clinical history suggestive of this condition). We conclude that the CLN8 nonsense mutation is almost certainly the cause of the neurological disorder in these dogs. Many different CLN8 mutations have been identified in human NCL patients (http://www.ucl.ac.uk/ncl/CLN8mutationtable.htm) [32, 33]. These patients have shown either of two distinct disease phenotypes. A large cohort of Finnish patients with a CLN8:c.70CNG missense mutation exhibited an atypical juvenile-onset NCL sometimes called Northern epilepsy [34]. In these patients, the first seizures occur at 5 to 10 years of age [34,35]. A progressive psychomotor deterioration becomes apparent a few years later; however, disease progression is markedly slower in Northern epilepsy patients compared to patients with the other forms of childhood-onset NCL. Northern epilepsy patients have a near normal life expectancy and retain their eyesight [34,35]. More than 10 different CLN8 mutations have been found in the other disease phenotype, often referred to as late infantile CLN8 disease, or variant late infantile NCL (vLINCL) (http://www.ucl.ac.uk/ncl/ CLN8mutationtable.htm) [32,33]. In these patients, seizures may begin as early as 3 years of age. There is rapid psychomotor deterioration and visual impairment or loss [32,36,37]. The NCL of the CLN8:c.585A homozygous dogs more closely resembles the vLINCL disease phenotype in that there is visual loss, rapid disease progression and a markedly decreased life expectancy. In our survey of CLN8:c.585GNA genotypes in archived DNA, all of the samples from Blue Heelers were homozygous for the reference CLN8: c.585G allele, whereas 4 of the Australian Shepherd samples were c.585A/G heterozygotes and 3 were homozygous for the mutant CLN8: c.585A allele. This distribution of genotypes could have occurred because 92% of the samples in the survey were from Australian Shepherds. While we cannot be certain about the source of the c.585A alleles in the Fig. 6. (A) Sequence reads from the mixed-breed dog whole-genome sequence aligned to a segment of canine chromosome 37 showing the homozygous GNA transition in CLN8. (B) Automated Sanger sequence confirms the GNA transition in CLN8 in DNA from the mixed-breed dog with NCL. 308 J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 mixed breed dog, we know that this allele has occurred in purebred Australian Shepherds. The samples from the 7 Australian Shepherds harboring 1 or 2 c.585A alleles were acquired over a span of 10 years and the 2 homozygous siblings had the only known family relationship among these 7 dogs. Thus, the c.585A allele appears to be rare, but widespread among Australian Shepherds. Previously, English Setters were found to develop NCL as a result of a CLN8:c.491CNT transition that predicts a CLN8:p.Leu164Pro amino acid substitution [7]. Dogs with this mutation were maintained for many years in research colonies [38–40]; however, it is doubtful that any descendants of the English Setters with the CLN8:c.491CNT mutation still survive. The existence of dogs with the CLN8:c.585GNA mutation may provide an opportunity to establish a new canine NCL model to investigate the functions of CLN8 and evaluate therapies that could prove helpful to human vLINCL patients with CLN8 mutations. In conclusion, we have identified a CLN8 nonsense mutation that is most likely the cause of NCL in a mixed breed dog and also the cause of previously described NCL in unrelated Australian Shepherds. This missense mutation was found by prioritizing the sequence variants in the whole genome sequence of a single affected dog. Similar whole genome sequencing strategies have been used to identify CUBN mutations in Border Collies and Beagles with Imerslund-Gräsbeck syndrome, a COL11A2 mutation in Labrador Retrievers with disproportionate dwarfism, a SUV39H2 mutation in Labrador Retrievers with hereditary nasal parakeratosis, and a KCNJ10 mutation in Jack Russell Terriers with spinocerebellar ataxia and myokymia [41–45]. As the costs for generating whole genome sequences decrease and software for data analysis improves, we expect whole genome sequencing to become more widely used for identifying the mutations responsible for many other heritable diseases in domestic animals. Supplementary data to this article can be found online at http://dx. doi.org/10.1016/j.ymgme.2014.05.014. Acknowledgments Our thanks to Joyce and John Van Dyke for donating tissues from their dog Annie for this study and to Liz Hansen for assisting with DNA sample collections and archiving. This work was supported in part by the Batten Disease Support and Research Association, the University of Missouri PRIME Fund, the University of Missouri Research Board, and Mizzou Advantage. References [1] S.E. Mole, R.E. Williams, H.H. Goebel, The Neuronal Ceroid Lipofuscinoses (Batten Disease), Oxford University Press, Oxford, UK, 2011. [2] K. Wisniewski, N. Zhong, Batten Disease: Diagnosis, Treatment, and Research, Academic Press, NY, 2001. [3] V. Warrier, M. Vieira, S.E. Mole, Genetic basis and phenotypic correlations of the neuronal ceroid lipofuscinoses, Biochim. Biophys. Acta 1832 (2013) 1827–1830. [4] T. Awano, M.L. Katz, D.P. O'Brien, J.F. Taylor, J. Evans, S. Khan, P. Lobel, I. Sohar, G.S. Johnson, A mutation in the cathepsin D gene (CTSD) in American bulldogs with neuronal ceroid-lipofuscinosis, Mol. Genet. Metab. 87 (2006) 341–348. [5] M.L. Katz, F.H. Farias, D.N. Sanders, R. Zeng, S. Khan, G.S. Johnson, D.P. O'Brien, A missense mutation in canine CLN6 in an Australian shepherd with neuronal ceroid lipofuscinosis, J. Biomed. Biotechnol. (2011), http://dx.doi.org/10.1155/2011/198042 (Article ID 198042). [6] S.A. Melville, C.L. Wilson, C.S. Chiang, V.P. Studdert, F. Lingaas, A.N. Wilton, A mutation in canine CLN5 causes neuronal ceroid lipofuscinosis in Border collie dogs, Genomics 86 (2005) 287–294. [7] M.L. Katz, S. Khan, T. Awano, A. Shahid, A.N. Siakotos, G.S. Johnson, A mutation in the CLN8 gene in English Setter dogs with neuronal ceroid-lipofuscinosis, Biochem. Biophys. Res. Commun. 327 (2005) 541–547. [8] M. Abitbol, J.L. Thibaud, N.J. Olby, C. Hitte, J.P. Puech, M. Maurer, F. Pilot-Storck, B. Hedan, S. Dreano, S. Brahimi, D. Delattre, C. Andre, F. Gray, F. Delisle, C. Caillaud, F. Bernex, J.J. Panthier, G. Aubin-Houzelstein, S. Blot, L. Tiret, A canine arylsulfatase G (ARSG) mutation leading to a sulfatase deficiency is associated with neuronal ceroid lipofuscinosis, Proc. Natl. Acad. Sci. U.S.A. 107 (2010) 14775–14780. [9] T. Awano, M.L. Katz, I. Sohar, P. Lobel, J.R. Coates, S. Khan, G.C. Johnson, U. Giger, G.S. Johnson, A frame shift mutation in the canine ortholog of human CLN2 in a juvenile dachshund with neuronal ceroid lipofuscinosis, Mol. Genet. Metab. 89 (2006) 254–260. [10] D.N. Sanders, F.H. Farias, G.S. Johnson, V. Chiang, J.R. Cook, D.P. O'Brien, S.L. Hofmann, J. Lu, M.L. Katz, A frame shift mutation in canine palmitoyl protein thiesterase 1 (PPT1) causes early onset neuronal ceroid lipofuscinosis in a Dachshund, Mol. Genet. Metab. 100 (2010) 349–356. [11] B. Vuillemenot, M.L. Katz, J.R. Coates, P. Lobel, P. Tiger, S. Bunting, S. Kanazono, D. Kennedy, L. Tsuruda, C. O'Neill, Intrathecal tripeptidyl peptidase-1 reduces lysosomal storage in a canine model of LINCL, Mol. Genet. Metab. 104 (2011) 325–337. [12] A.V. Zimin, G. Marçais, D. Puiu, M. Roberts, S.L. Salzberg, J.A. Yorke, The MaSuRCA genome assembler, Bioinformatics 29 (2013) 2669–2677. [13] K.J. Livak, Allelic discrimination using fluorogenic probes and the 5′ nuclease assay, Genetic Analysis 14 (1999) 143–149. [14] S.L. Macauley, M. Pekny, M.S. Sands, The role of attenuated astrocyte activation in infantile neuronal ceroid lipofuscinosis, J. Neurosci. 31 (2011) 15575–15585. [15] Y. Nakamoto, O. Yamato, K. Uchida, K. Nibe, S. Tamura, T. Ozawa, N. Ueoka, A. Nukaya, A. Yabuki, M. Nakaichi, Neuronal ceroid-lipofuscinosis in longhaired Chihuahuas: clinical, pathologic, and MRI findings, J. Am. Anim. Hosp. Assoc. 47 (2011) 64–70. [16] J. Tyynela, J.D. Cooper, M.N. Khan, S.J. Shemilts, M. Haltia, Hippocampal pathology in the human neuronal ceroid-lipofuscinoses: distinct patterns of storage deposition, neurodegeneration and glial activation, Brain Pathol. 14 (2004) 349–357. [17] R.C. Riis, J.F. Cummings, E.R. Loew, A. de Lahunta, Tibetan terrier model of canine ceroid lipofuscinosis, Am. J. Med. Genet. 42 (1992) 615–621. [18] D.P. O'Brien, M.L. Katz, Neuronal ceroid lipofuscinosis in three Australian shepherd littermates, J. Vet. Intern. Med. 22 (2008) 472–475. [19] M.L. Katz, J.R. Coates, J.J. Cooper, D.P. O'Brien, M. Jeong, K. Narfström, Retinal pathology in a canine model of late infantile neuronal ceroid lipofuscinosis, Invest. Ophthalmol. Vis. Sci. 49 (2008) 2686–2695. [20] J.D. Cooper, The neuronal ceroid lipofuscinoses: the same, but different? Biochem. Soc. Trans. 38 (2010) 1448–1452. [21] T. Bensaoula, H. Shibuya, M.L. Katz, J.E. Smith, G.S. Johnson, S.K. John, A.H. Milam, Histopathologic and immunocytochemical analysis of the retina and ocular tissues in Batten disease, Ophthalmology 107 (2000) 1746–1753. [22] H.H. Goebel, K.E. Wisniewski, Current state of clinical and morphological features in human NCL, Brain Pathol. 14 (2004) 61–69. [23] S. Ranta, M. Savukoski, P. Santavuori, M. Haltia, Studies of homogeneous populations: CLN5 and CLN8, Adv. Genet. 45 (2001) 123–140. [24] M. Haltia, The neuronal ceroid-lipofuscinoses, J. Neuropathol. Exp. Neurol. 62 (2003) 1–13. [25] G. Anderson, M. Elleder, H.H. Goebel, Morphological diagnostic and pathological considerations, in: S.E. Mole, R.E. Williams, H.H. Goebel (Eds.), The Neuronal Ceroid Lipofuscinoses (Batten Disease), Oxford University Press, Oxford, UK, 2011, pp. 35–49. [26] D. Harman, Lipofuscin and ceroid formation: the cellular recycling system, Adv. Exp. Med. Biol. 266 (1989) 3–15. [27] S.E. Haddad, M. Khoury, M. Daoud, R. Kantar, H. Harati, T. Mousallem, O. Alzate, B. Meyer, R. Boustany, CLN5 and CLN8 protein association with ceramide synthase: biochemical and proteomic approaches, Electrophoresis 33 (2012) (3978-3809). [28] R. Passantino, C. Cascio, I. Deidda, G. Galizzi, D. Russo, G. Spedale, P. Guarneri, Identifying protein partners of CLN8, and ER-resident protein involved in neuronal ceroid lipofuscinosis, Biochim. Biophys. Acta 1833 (2013) 529–540. [29] L. Lonka, A. Kyttala, S. Ranta, A. Jalanko, A.E. Lehesjoki, The neuronal ceroid lipofuscinosis CLN8 membrane protein is a resident of the endoplasmic reticulum, Hum. Mol. Genet. 9 (2000) 1691–1697. [30] E. Winter, C.E. Ponting, TRAM, LAG1 and CLN8: members of a novel family of lipidsensing domains? Trends Biochem. Sci. 27 (2002) 381–383. [31] Y. Pewzner-Jung, S. Ben-Dor, F. A.H., When do lasses (longevity assurance genes) become CerS (ceramide synthases)?: Insights into the regulation of ceramide synthesis, J. Biol. Chem. 281 (2006) 25001–25005. [32] K. Reinhardt, M. Grapp, K. Schlachter, W. Bruck, J. Gartner, R. Steinfeld, Novel CLN8 mutations confirm the clinical and ethnic diversity of late infantile neuronal ceroid lipofuscinosis, Clin. Genet. 77 (2010) 79–85. [33] M. Kousi, A.E. Lehesjoki, S.E. Mole, Update of the mutation spectrum and clinical correlations of over 360 mutations in eight genes that underlie the neuronal ceroid lipofuscinoses, Hum. Mutat. 33 (2012) 42–63. [34] A. Hirvasniemi, H. Lang, A.E. Lehesjoki, J. Leisti, Northern epilepsy syndrome: an inherited childhood onset epilepsy with associated mental deterioration, J. Med. Genet. 31 (1994) 177–182. [35] R. Herva, J. Tyynela, A. Hirvasniemi, M. Syrjakallio-Ylitalo, M. Haltia, Northern epilepsy: a novel form of neuronal ceroid-lipofuscinosis, Brain Pathol. 10 (2000) 215–222. [36] S. Ranta, M. Topcu, S. Tegelberg, H. Tan, A. Ustubutun, I. Saatci, A. Dufke, H. Enders, K. Pohl, Y. Alembik, W.A. Mitchell, S.E. Mole, A.E. Lehesjoki, Variant late infantile neuronal ceroid lipofuscinosis in a subset of Turkish patients is allelic to Northern epilepsy, Hum. Mutat. 23 (2004) 300–305. [37] N. Zelnik, M. Mahajna, T.C. Iancu, R. Sharony, M. Zeigler, A novel mutation of the CLN8 gene: is there a Mediterranean phenotype? Pediatr. Neurol. 36 (2007) 411–413. [38] N. Koppang, The English setter with ceroid-lipofuscinosis: a suitable model for the juvenile type of ceroid-lipofuscinosis, Am. J. Med. Genet. (Suppl. 5) (1988) 117–126. [39] N. Koppang, English setter model and juvenile ceroid-lipofuscinosis in man, J. Med. Genet. 42 (1992) 594–599. [40] A.N. Siakotos, G.D. Hutchins, M.R. Farlow, M.L. Katz, Assessment of dietary therapies in a canine model of Batten disease, Eur. J. Paediatr. Neurol. 5A (2001) 151–156. [41] M. Owczarek-Lipska, V. Jagannathan, C. Drogemuller, S. Lutz, B. Glanemann, T. Leeb, P.H. Kook, A frameshift mutation in the cubilin gene (CUBN) in Border Collies with Imerslund-Gräsbeck syndrome (selective cobalamin malabsorption), PLoS One 16 (2013) e61144. [42] M. Drogemuller, V. Jagannathan, J. Howard, R. Bruggmann, C. Drogemuller, M. Ruetten, T. Leeb, P.H. Kook, A frameshift mutation in the cubilin gene (CUBN) in J. Guo et al. / Molecular Genetics and Metabolism 112 (2014) 302–309 Beagles with Imerslund-Gräsbeck syndrome (selective cobalamin malabsorption), Anim. Genet. 48 (2014) 148–150. [43] M. Frischknecht, H. Niehof-Oellers, V. Jagannathan, M. Owczarek-Lipska, C. Drögemüller, E. Dietschi, G. Dolf, B. Tellhelm, J. Lang, K. Tiira, H. Lohi, L. T., A COL11A2 mutation in Labrador retrievers with mild disproportionate dwarfism, PLoS One 8 (2013) e60149. [44] V. Jagannathan, J. Bannoehr, P. Plattet, R. Hauswirth, C. Drogemuller, M. Drogemuller, D.J. Wiener, M. Doherr, M. Owczarek-Lipska, A. Galichet, M.M. Welle, K. Tengvall, K. Bergvall, H. Lohi, S. Rüfenacht, M. Linek, M. Paradis, E.J. Müller, P. Roosje, T. Leeb, A 309 mutation in the SUV39H2 gene in Labrador Retrievers with hereditary nasal parakeratosis (HNPK) provides insights into the epigenetics of keratinocyte differentiation, PLoS Genet. 9 (2013) e1003848. [45] D. Gilliam, D.P. O'Brien, J.R. Coates, G.S. Johnson, G.C. Johnson, T. MhlangaMutangadura, L. Hansen, J.R. Taylor, R.D. Schnabel, A homozygous KCNJ10 mutation in Jack Russell Terriers and related breeds with spinocerebellar ataxia with myokymia, seizures, or both, J. Vet. Intern. Med. (2014) (in press).