Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Toxicodynamics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug interaction wikipedia , lookup
Norepinephrine wikipedia , lookup
Effects of long-term benzodiazepine use wikipedia , lookup
Neuropharmacology wikipedia , lookup
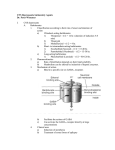
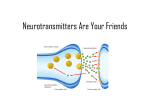
General Pharmacology Drugs That Affect the Central Nervous System S. Habibian Dehkordi D.V.M, Ph.D Central Nervous System CNS CNS Brain and Spinal Cord Acts as control for regulating physical and mental processes Neurons are the brains functional units Neurons The brain is a collection of about 10 billion interconnected neurons. Each neuron is a cell that uses biochemical reactions to receive, process and transmit information. Neurotransmitters Chemical substances that carry messages from one neuron to another or from a neuron to other body tissues, such as cardiac or skeletal muscles. Synapses The synapse is a small gap separating neurons. Receptors Proteins embedded in the cell membranes of neurons. A neurotransmitter must bind to receptors to exert an effect on the next neuron in the chain. Drugs That Effect CNS Depressants Stimulants CNS Depressants Mild CNS depressant: decreased interest in surroundings, inability to focus. Moderate CNS depressant: drowsiness or sleep, decreased perception of heat or cold. Severe CNS depressant: unconsciousness or coma, loss of reflexes, respiratory failure and death. CNS Stimulation Mild stimulation: wakefulness, mental alertness, and decreased fatigue. Moderate stimulation: hyperactivity, excessive talking, nervousness, and insomnia. Excessive stimulation: confusion, seizures, and cardiac dysrhythmias. CNS Drugs Anticonvulsants: help prevent seizures by suppressing the spread of abnormal electric impulses from the seizure focus to other areas of the cerebral cortex All anticonvulsants are CNS depressants and may cause ataxia, drowsiness, and hepatotoxicity Examples: Phenobarbital (short-acting barbiturate) Primidone (structurally similar to phenobarbital) Diazepam (used IV to treat status epilepticus) Clorazepate (adjunct anticonvulsant) Potassium bromide (adjunct anticonvulsant) © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Tranquilizers: used to calm animals; reduce anxiety and aggression Sedatives: used to quiet excited animals; decrease irritability and excitement Anti-anxiety drugs: lessen anxiousness, but do not make animals drowsy Examples in these groups: Phenothiazine derivatives (acepromazine, chlorpromazine) Benzodiazepines (diazepam) Alpha-2 agonists (xylazine, detomidine, medetomidine) © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Analgesics: drugs that relieve pain Analgesics are categorized as non-narcotic (Chapter 16) or narcotic Narcotic analgesics are used for moderate to severe pain Narcotic refers to opioid (natural) or opioidlike (synthetic) products © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Opioids: Do not produce anesthesia; patients still respond to sound and sensation Produce analgesia and sedation, and relieve anxiety Side effects: respiratory depression, excitement if given too rapidly Produce their effects by the action of opioid receptors Mu = found in the brain Kappa = found in the cerebral cortex and spinal cord Sigma = found in the brain © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Examples of opioids: Opium Morphine sulfate Meperidine Hydromorphone Butorphanol Hydrocodone Fentanyl Etorphine Buprenorphine Pentazocine © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Opioid antagonists: Block the binding of opioids to their receptors Used to treat respiratory and CNS depression of opioid use Examples include naloxone and naltrexone © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. CNS Drugs Neuroleptanalgesics: Combination of an opioid and a tranquilizer or sedative Can cause a state of CNS depression and analgesia and may or may not produce unconsciousness Combination products may be prepared by veterinarian Examples include acepromazine and morphine; xylazine and butorphanol © 2004 by Thomson Delmar Learning, a part of the Thomson Corporation. Sedative-Hypnotic Drugs BASIC PHARMACOLOGY OF SEDATIVE-HYPNOTICS An effective sedative (anxiolytic) agent should reduce anxiety and exert a calming effect with little or no effect on motor or mental functions. A hypnotic drug should produce drowsiness and encourage the onset and maintenance of a state of sleep that as far as possible resembles the natural sleep state. BASIC PHARMACOLOGY OF SEDATIVE-HYPNOTICS Hypnotic effects involve more pronounced depression of the central nervous system than sedation, and this can be achieved with most sedative drugs simply by increasing the dose. Graded dose-dependent depression of central nervous system function is a characteristic of sedative-hypnotics. CHEMICAL CLASSIFICATION 1. 2. 3. Benzodiazepines: not to lead general anesthesia, raraly death. Barbiturates: the older sedative-hypnotics, general depression of central nervous system. With such drugs, an increase in dose above that needed for hypnosis may lead to a state of general anesthesia. At still higher doses, it may depress respiratory and vasomotor centers in the medulla, leading to coma and death. Other classes of drugs: chloral hydrate, buspirone, et al. Ⅰ.Benzodiazepines The first benzodiazepine, chlordiazepoxide, was synthesised by accident in 1961. Ⅰ.Benzodiazepines Derivative of 1,4- benzodiazepines. About 20 are available for clinical use. They are basically similar in their pharmacological actions, though some degree of selectivity has been reported. It is possible that selectivity with respect to two types of benzodiazepine receptor may account for these differences. From a clinical point of view, difference in pharmacokinetic behaviour are more important than difference in profile of activity. PHARMACOLOGICAL EFFECTS 1. Reduction of anxiety and aggression : affects the hippocampus and nucleus amygdalae 2. Sedation and induction of sleep: (1) the latency of sleep onset is decreased; (2) the duration of stage 2 NREM sleep is increased; (3) the duration of slow-wave sleep is decreased. PHARMACOLOGICAL EFFECTS Reasons for their extensive clinical use: (1) great margin of safety; (2) little effect on REM sleep; (3) little hepatic microsomal drugmetabolizing enzymes; (4) slight physiologic and psychologic dependence and withdrawal syndrome; (5) less adverse effects such as residual drowsiness and incoordination movement. 3. Anticonvulsant and antiseizure They are highly effective against chemically induced convulsions caused by leptazol, bicuculline and similar drugs but less so against electrically induced convulsions. The can enhance GABA-mediated synaptic systems and inhibit excitatory transmission. 4. Muscle relaxation relax contracted muscle in joint diease or muscle pasm. 5. Other effects lead to temporary amnesia decrease the dosage of anesthetic; depress respiratory and cardiovascular fuction. MECHANISM OF ACTION Benzodiazepines act very selectively on GABAA-receptors, which mediate the fast inhibitory synaptic response produced by activity in GABA-ergic neurons. The effect of benzodiazepines is to enhance the response to GABA, by facilitating the opening of GABA-activated chloride channels (an increase in the frequency of channel opening, but no change in the conductance or mean open time). MECHANISM OF ACTION Benzodiazepines bind specifically to a regulatory site on the receptor, distinct from the GABA binding site, and enhanced receptor affinity for GABA. The GABAA-receptors is a ligand-gated ion channel consisting of a pentameric assembly of subunits. PHARMACOKINETIC ASPECTS Well absorbed when given orally; They bind strongly to plasma protein, and their high lipid solubility cause many of them to accumulate gradually in body fat. Distribution volumes is big. Metabolic transformation in the microsomal drug-metabolizing enzyme systems of the liver, eventually excreted as glucuronide conjugates in the urine. They vary greatly in duration of action, and can be roughly divided into Short-acting compounds: triazolam, oxazepam(15-30min, t1/2 2-3 h) Medium-acting compounds: estazolam, nitrazepam (40min, t1/2 5-8 h) Long-acting compounds: diazepam, flurazepam(50h) ADVERSE DRUG REACTION Acute toxicity: Benzodiazepines in acute overdose are considerably less dangerous than other sedative-hypnotic drugs. Cause prolonged sleep,without serious depression of respiration or cardiovascular. The availability of an effective antagonist, flumazenil. ADVERSE DRUG REACTION Side-effects during therapeutic use: drowsiness, confusion, amnesia, impaired coordination. Main disadvantages are interaction with alcohol, long-lasting hangover and the development of dependence. Tolerance and dependence: induction of hepatic drug-metabolising enzymes; a change at the receptor level; Ⅱ.BARBITURATES Classification (1)Ultra-short-acting barbiturates: act within seconds, and their duration of action is 30min. Therapeutic use of Thiopental: anesthesia (2)Short-acting barbiturates: have a duration of action of about 2h. The principal use of Secobarbital : sleep- Ⅱ.BARBITURATES Classification (3)Intermediate-acting barbiturates: have and effect lasting 3-5h. The principal use of Amobarbital is as hypnotics. (4)Long-acting barbiturates: have a duration of action greater than 6h. Such as Barbital and Phenobarbital. Therapeutic uses: hypnotics and sedative, and antiepileptic agents at low doses. BARBITURATES Barbiturates depress the CNS at all level in a dose-dependent fashion. Now it mainly used in anaesthesia and treatment of epilepsy; use as sedative-hypnotic agents is no longer recommended. BARBITURATES Reasons: (1) have a narrow therapeutic-to-toxic dosage range. (2) suppress REM sleep. (3) Tolerance develops relatively quickly. (4) have a high potential for physical dependence and abuse. (5) potent inducers of hepatic drugmetabolising enzymea. MECHANISM OF ACTION (1) Barbiturates share with benzodiazepines the ability to enhance the action of GABA, but they bind a different site on the GABAreceptor/chloride channel, and their action seems to prolong the duration of the opening of GABA-activated chloride channels. MECHANISM OF ACTION (2) At high doses, barbiturates can inhibit the release of the Ca2+-dependent neurotransmitter. Pharmacokinetics High lipid solubility allows rapid transport across the blood-brain barrier and results in a short onset. Removal from the brain occurs via redistribution to the other tissues results in short duration of action. Barbiturates and their metabolites the excretion via the renal route. Alkalinization of the urine expedites the excretion of barbiturates. Treatment of acute overdosage: Sodium bicarbonate. Therapeutic uses Sedative-hypnotic agents Be used in the emergency treatment of convulsions as in status epilepticus. Anesthetic (or be given before anesthetic) Combination with antipyretic-analgesic Treatment of hyperbilirubinemia and kernicterus in the neonate. Adverse effects After effect: hangover---dizzy, drowsiness, amnesia, impaired judgment, disorientation. Tolerance: decreased responsiveness to a drug following repeated exposure because of down-regulation of receptors and induction of hepatic drug-metabolising enzymes. Adverse effects Dependence: including psychologic and physiologic dependence. Withdrawal symptoms: excitation, insomnia, tremor, anxiety, hallucinations and sometimes convulsions. Depressant effect on respiration: can cross the placental barrier during pregnancy and secrete to breast milk. Others: Skin eruptions and porphyria Phenothiazines (Tranquilizers) Indications Good sedation for healthy animals undergoing elective procedures Anti-emetic Phenothiazines Contraindications Convulsing/epileptic patients, seizure history or head trauma Acepromazine may reduce the seizure threshold of the animal Shock (hypovolemia) and hypothermia because of peripheral vasodilation that can lead to hypotension Depressed patients Caution with geriatrics and pediatrics; use a lower dose or consider alternative agents such as benzodiazepines Liver or kidney disease Allergy testing because of antihistamine effect Phenothiazines Other effects Antiarrhythmic effect May cause excitement rather than sedation Personality changes that usually subside within 48 hours Benzodiazepines (Benzodiazepines) Indications Convulsing/epileptic patients Patients with a history of seizure CSF taps or myelogram procedures Minimal cardiovascular or respiratory depression Useful in geriatric or pediatric animals Ideal for older, depressed or anxious patients Works effectively as an induction agent when used with ketamine Benzodiazepines (Benzodiazepines) Contraindications May cause excitement in some dogs, cats and horses Does not sedate animal but has antianxiety and calming effects May make animal more difficult when inhibitions and anxieties are removed Neonatal animals and animals with poor hepatic function Benzodiazepines (Benzodiazepines) Valium is in a propylene glycol solution, is insoluble in water May precipitate with other drugs Propylene glycol is irritating and may sting at the injection site Does not work well when given via routes other than IV Benzodiazepines (Benzodiazepines) Other points Midazolam is water soluble and readily combines with opioids (oxymorphone, butorphanol) Effects are reversed with flumazenil if adverse effects are seen α2-Agonists Are derivatives of thiazine Examples: Xylazine (Rompun, Anased) Romifidine Detomidine (Dormosedan) Medetomidine (Domitor) α2-Agonists Stimulates the α2-adrenoreceptors causing a decrease in norepinephrine Indication Potential side effects limit use to sedation only, not for preanesthetic medication Can use to sedate a vicious animal before euthanasia α2-Agonists Have some short-lived (16 to 20 minutes) analgesic effects Will cause vomiting in up to 50% of dogs and 90% of cats Xylazine and Detomidine are used most frequently in horses Xylazine also used in ruminants but at much lower dosages α2-Agonists Contraindications Considerable potential for side effects especially if administered IV Profound cardiovascular effects include bradycardia, profound hypotension, decreased contractility and stroke volume and second degree heart block Contraindicated when concerned about respiratory function, hepatic and renal function and if the animal is prone to gastric dilation α2-Agonists Contraindications Associated with temporary behavior and personality changes Reduces pancreatic secretions causing transient hyperglycemia (exacerbates dehydration) Opioids will exacerbate these side effects Opioids Commonly used: Morphine Oxymorphone (Numorphan) Butorphanol (Torbugesic, Torbutrol) Hydromorphone Meperidine (Demerol, Pethidine) Fentanyl Opioids Act by reversible combination with one or more specific receptors in the brain and spinal column Also classified according to their analgesic activity and their addiction potential Pure agonists are more effective for severe pain In order of decreasing potency they are: Fentanyl Oxymorphone Buprenorphine Butorphanol Meperidine pentazocine Opioids Commonly used as an analgesic in premedication, as an induction agent or can be used for balanced anesthesia and post-operative pain control Provides some sedation and may potentiate the action of the sedative that it is given with has a synergistic effect Opioids Commonly used as an analgesic in premedication, as an induction agent or can be used for balanced anesthesia and post-operative pain control Fentanyl, sufentanil and oxymorphone are often part of a balanced anesthetic regimen Fentanyl is available as a transdermal patch in various sizes for long-term analgesia Used as neuroleptanalgesia in combination wit tranquilizer Morphine can be injected epidurally or sub-arachnoidally for regional analgesia Opioids Fentanyl patches Takes 8 to 12 hours to reach effectiveness but will last for several days Very few cardiovascular side effects Does not significantly contribute to vasodilation or hypotension Heating pads can increase transdermal uptake Opioids Reversible by use of pure antagonists such as naloxone or nalmefene Compete with opioids for the specific receptor sites Possible to titrate the naloxone dose so as to remove the side effects yet maintain analgesia Opioids Other effects in addition to analgesia Either stimulate or depress the central nervous system Depends on the dose, species and opioid agent Excitement occurs if given rapidly IV Horse and cat are particularly susceptible to excitatory effects Dogs generally show sedation although hypnosis can be seen in higher doses in sick animals Dogs that are not in pain may show excitement especially if given without any other agents Opioids Other effects in addition to analgesia Cardiopulmonary effects Bradycardia Possible hypotension with release of histamine Especially if given IV Morphine and meperidine Increased muscle contraction in low doses Inotropic effect morphine Opioids Other effects in addition to analgesia Respiratory depression is dose dependent Gastrointestinal effects depend on the agent May initially include diarrhea, vomiting and flatulence Constipation may occur as a result of prolonged GI stasis Addiction Opioids Other effects in addition to analgesia Body temperature decreases and panting in dogs due to a resetting of the thermoregulatory center in the brain Miosis in dogs and pigs and mydriasis the cat and horse Increased responsiveness to noise Cough suppression Excessive salivation Sweating, particularly in the horse Opioids Contraindications Previous history of opioid excitement Morphine has a higher incidence of producing vomiting so should be avoided in cases of GI obstruction and diaphragmatic hernia Classified as a narcotic in Canada and is a Schedule II controlled drug in the US CNS Stimulants Defination “Stimulants are a substance which tends to increase behavioral activity when administered” CNS Stimulants Two disorders treated with CNS stimulants are narcolepsy and Attention Deficit Hyperactivity Disorder CNS stimulants act by facilitation initiation and transmission of nerve impulses that excite other cells. New drugs act selectively to inhibit reuptake or norepinephrine in the nervous system. Signs and symptoms: 1- Elevate Mood 2- Increase Motor Activity 3- Increase Alertness 4- Decrease need for Sleep In case of overdose lead to convulsion and death. CNS Stimulants - They can be divided based on their site of action: 1.Cerebral stimulants (amphetamines) 2.Medullary stimulants (picrotoxin) 3.Spinal stimulants (strychnine) Indications Analeptics (CNS stimulants) Reversal of anaesthesia- induced respiratory depression Anorexiants Thought to suppress the appetite control centre in the brain ADHDStimulate the areas in the brain responsible for mental alertness and attentiveness NarcolepsyIncrease mental alertness Migraine headaches Caffeine, co-administered with other drugs, used to treat headaches Side Effects Wide range, dose related Tend to “speed up” body systems Common adverse effects include: Palpitations, tachycardia, hypertension, angina, dysrhythmias, nervousness, restlessness, anxiety, insomnia, nausea, vomiting, diarrhea, increased urinary frequency 1- Amphetamine MOAs : Block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space. - Clinical use: 1. Narcolepsy. 2. Attention-deficit hyperactivity disorder Amphetamine Adverse effects: - Cardiovascular: Hypertension (7% to 22%, pediatric ) - Endocrine metabolic: Weight loss (4% to 9%, pediatric; 11%, adults ) - Gastrointestinal: Abdominal pain (11% to 14%, pediatrics ), Loss of appetite (22% to 36%), Xerostomia (35% ) - Neurologic: Headache (26% ), Insomnia ( ارق12% to 17%, pediatric; 27%, adults ) - Psychiatric: Feeling nervous (6% ) Amphetamine After injecting, the mice with amphetamine you well notice: - Hair erection - Licking, gnawing. - Stereotype - Sniffing Picrotoxin MOA: Non-competitive antagonist of GABA receptors. After injecting the mice with picrotoxin you well notice: - Clonic convulsion characterized by : 1. Asymmetric 2. Intermittent 3. Spontaneous 4. Coordinated Strychinine MOA: Competitive antagonist of the glycin receptors. After injecting the mice with Strychinine you well notice: - Tonic convulsion characterized by : 1. Symmetric 2. Reflex in origin 3. Continuous 4. Uncoordinated. Attention Deficit Hyperactive Disorder Methylphenidate Brand Name: Ritalin Classification Therapeutic: CNS stimulant Action: Produces CNS and respiratory stimulation with weak sympathomimetic activity. Therapeutic Effects: Increased attention span in ADHD. Increased motor activity, mental alertness, and diminished fatigue in narcoleptic patients.