Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Neuropharmacology wikipedia , lookup
Clinical trial wikipedia , lookup
Plateau principle wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Pharmacognosy wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Dydrogesterone wikipedia , lookup
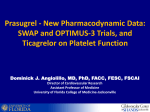
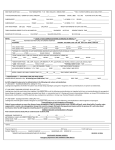
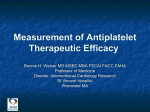
Platelets, June 2006; 17(4): 209–217 ORIGINAL ARTICLE Platelet inhibitory activity and pharmacokinetics of prasugrel (CS-747) a novel thienopyridine P2Y12 inhibitor: A single ascending dose study in healthy humansy FUMITOSHI ASAI1, JOSEPH A. JAKUBOWSKI2, HIDEO NAGANUMA1, JOHN T. BRANDT2, NOBUKO MATSUSHIMA1, TAKASHI HIROTA1, STEPHEN FREESTONE3, & KENNETH J. WINTERS2 1 Sankyo Co., Ltd., Tokyo, Japan, 2Lilly Research Laboratories, Eli Lilly and Company, Indianapolis, IN, USA, and 3Inveresk Clinical Research Ltd., Edinburgh, Scotland, UK (Received 13 October 2005; accepted 6 January 2006) Abstract We assessed the tolerability, pharmacodynamics as measured by inhibition of platelet aggregation (IPA), and pharmacokinetics of prasugrel (CS-747, LY640315), a novel thienopyridine antiplatelet agent in healthy volunteers. Twenty-four subjects were randomized into four groups of six in a double-blind, placebo-controlled trial. One subject in each group received placebo and five subjects received prasugrel orally at single doses of 2.5, 10, 30, or 75 mg. The IPA, assessed using 5 and 20 mM ADP, was periodically measured over a 7-day period by light transmission aggregometry. Plasma concentrations for three major metabolites, R-95913, R-106583, and R-100932, were measured. There were no serious adverse events and no clinically significant changes noted in any laboratory or clinical evaluations in any subject. At 1 h after prasugrel 30 and 75 mg, platelet aggregation induced by 20 mM ADP was inhibited by 43.5 7.8 and 43.2 15.7%, respectively, and this inhibition was significantly greater than that following placebo (5.9 3.5%) (P < 0.05 for both doses). The degree of inhibition observed at 2 h was slightly higher with both prasugrel 30 and 75 mg (59.8 9.9 and 57.0 7.2%) and was maintained through the subsequent 22 h. At 24 h, maximal platelet aggregation induced by 20 mM ADP was reduced to 39% in all subjects receiving prasugrel 30 mg and to 38% in subjects receiving prasugrel 75 mg. Full recovery of platelet aggregation occurred between 48 h and 7 days suggesting irreversible inhibition by prasugrel and/or its metabolites. With prasugrel 2.5 and 10 mg, there was no measurable effect on platelet aggregation throughout the study (P > 0.05 for 2.5 and 10 mg prasugrel vs. placebo). With prasugrel 75 mg at 4 h postdose, there was a significant increase in the mean bleeding time compared to placebo (682 vs. 161 s; P < 0.05). Prasugrel metabolites obeyed linear pharmacokinetics and the three metabolites appeared in the plasma soon after administration, reaching maximum levels at approximately 1 h. In conclusion, prasugrel 30 and 75 mg were well tolerated and achieved a consistently high level of platelet inhibition with a fast onset of action. Keywords: Prasugrel, CS-747, platelets, phase 1, thienopyridine Introduction It is widely recognized that platelet activation and aggregation at sites of atherosclerotic plaque rupture and subsequent thrombus formation underlie the tissue ischemia and necrosis in what is collectively known as acute coronary syndrome (ACS) [1, 2]. Further support of the central role that platelet activation and aggregation play in occlusive arterial disease is provided by the efficacy of platelet inhibitory agents in ACS. Three distinct classes of antiplatelet agents are in wide clinical use, namely aspirin, glycoprotein IIb–IIIa (GPIIb–IIIa) antagonists, and the adenosine 50 -diphosphate (ADP) receptor antagonists of which the most commonly used is clopidogrel. Aspirin reduces the risk of a serious vascular event in a wide range of atherosclerotic vascular disease [3]. Moreover, antiplatelet drugs acting through other pathways such as the final common pathway of GPIIb–IIIa or the platelet Correspondence: Joseph A. Jakubowski, PhD, Lilly Research Laboratories, Lilly Corporate Center, Indianapolis, IN 46285, USA. Tel: 1 317 276 9036. Fax: 1 317 433 1996. E-mail: [email protected] yThis study was conducted at Inveresk Clinical Research, Ltd., Edinburgh, Scotland, UK. ISSN 0953–7104 print/ISSN 1369–1635 online ß 2006 Taylor & Francis DOI: 10.1080/09537100600565551 210 F. Asai et al. ADP receptor have also provided improved clinical outcomes in patients with non ST-elevation ACS and those undergoing percutaneous coronary intervention (PCI) [4–7]. Ticlopidine and clopidogrel are thienopyridine prodrugs which following oral administration are metabolized to an active sulfhydryl form that binds to and irreversibly antagonizes the P2Y12 class of platelet ADP receptor [8]. Where approved, clopidogrel is the thienopyridine of choice due to its more favorable safety profile compared to ticlopidine. The effectiveness of clopidogrel reflects its ability to block platelet activation and aggregation induced by platelet-derived ADP released at sites of plaque rupture. However, several limitations of clopidogrel have recently been discussed including inter-patient variability in antiplatelet effects and a relatively slow onset of action [9–12]. More recently a novel thienopyridine P2Y12 antagonist, prasugrel (CS-747, LY640315), has been identified and profiled [13–16]. Preclinical studies indicate that like clopidogrel, prasugrel is a prodrug that requires metabolic activation to an active metabolite [13]. In vivo and ex vivo studies demonstrate that following oral dosing of prasugrel there is a rapid and potent inhibition of ADP-induced platelet activation and aggregation [13–15]. These early studies demonstrated that the dose required to achieve a given degree of platelet inhibition or inhibition of thrombus formation was approximately one-tenth and one-hundredth that of the dose of clopidogrel and ticlopidine, respectively. The current report describes the first experience of prasugrel in man in a study that examined the safety, tolerability, pharmacokinetics, and pharmacodynamics, as measured by inhibition of platelet aggregation (IPA), of prasugrel in a single ascending dose study. consisted of: medical history, complete physical examination and vital signs, 12-lead electrocardiography (ECG) recording, hematology, coagulation, clinical chemistry and urinalysis, urine screening for drugs including drugs of abuse, fecal occult blood examination, bleeding time, examination for petechiae, and Von Willebrand factor and arachidonic acid-induced platelet aggregation. All subjects were screened within 14 days prior to randomization. Exclusion criteria included a history of important bleeding disorders, a personal or family history of coagulation or bleeding disorders, reasonable suspicion of vascular malformations, or abnormal coagulation values at screening. No medications other than study drugs were permitted during the study except those deemed necessary by the clinical investigator/ study director/supervising physician to treat adverse events. Aspirin and nonsteroidal anti-inflammatory drugs were excluded. Treatment administered Prasugrel was manufactured by Ube Industries Ltd. (Tokyo, Japan) and plain tablets containing 2.5, 5, or 10 mg as free base were formulated by Sankyo Co. Ltd. (Tokyo, Japan). Twenty-four male volunteers were randomized into four groups. Each group consisted of six subjects, of whom one subject received placebo and five subjects received prasugrel at doses of 2.5, 10, 30, or 75 mg. Prasugrel was administered to each fasting subject by the oral route, with 200 mL of water. Each volunteer remained in the clinic for two nights, and was discharged 24 h postdose. If any safety parameters did not meet predefined criteria, subjects were obliged to return at 48 h postdose; otherwise, all the subjects returned for an outpatient visit at day 7 and again at day 14 if required. Methods A randomized, double-blind, placebo-controlled, single oral ascending dose study was undertaken in healthy subjects. A primary objective was to determine the safety and tolerability of prasugrel, whereas a secondary objective was to assess the pharmacodynamics and pharmacokinetics of prasugrel. The study was conducted at Inveresk Clinical Research, Ltd., Edinburgh, Scotland. The Inveresk Research Ethics committee approved the protocol. Signed informed consent was obtained from each subject and the study was conducted in accordance with the provisions of the Declaration of Helsinki. Subjects Subjects were male volunteers, aged 18–50 years with no clinically important physical findings or abnormalities in laboratory results, including platelet function tests, at screening. The screening examination Safety Safety assessments performed at various timepoints throughout the study included measurement of vital signs, ECG, hematology, clinical chemistry, coagulation, urinalysis, fecal occult blood, fundoscopy, and examination for petechiae. Adverse events were recorded and monitored throughout the study. Pharmacodynamic measurements Prasugrel was assessed for its effects on human platelet function by monitoring light transmission platelet aggregation using a BioData PAP-4 aggregometer. Venous blood samples were collected into one-tenth volume 3.8% citrate. Platelet-rich and platelet-poor plasma were prepared using differential centrifugation. No adjustments to the platelet count were performed. Subjects were initially screened to confirm normal platelet function (see following) Single oral doses of prasugrel in healthy subjects using ristocetin (1.2 mg/mL) and sodium arachidonate (0.75 mM). These screening procedures were qualitative assessments to exclude Von Willebrand’s disease and aspirin ingestion, respectively. All platelet aggregation studies were completed within 3 h of sample collection. Platelet aggregation was determined at predose, 1, 2, 4, 8, and 24 h and day 7 postdose. Samples for platelet aggregation were also drawn at 48 h in the prasugrel 30 and 75 mg dose groups. The maximum percent aggregation response (MPA) to ADP (5 and 20 mM), and collagen (2 mg/mL) was recorded over a 4 min monitoring period. Inhibition of aggregation (IPA) was defined as follows: [1–(MPAt MPA0)] 100%, where MPA0 ¼ MPA at baseline and MPAt ¼ MPA at given timepoint (t). Bleeding time using the Ivy–Nelson method [17] was determined at screening, predose, 4 and 24 h postdose and at the 7-day follow-up. Pharmacokinetic measurements The plasma concentration of three major inactive prasugrel metabolites, R-95913, R-106583 and R-100932 (Figure 1), were measured for evaluation of absorption and elimination of the parent drug and its metabolites. At the time the study was conducted, 211 a validated analytical method for the active metabolite of prasugrel (R-138727) [18] was not available. Blood samples were collected during the course of the study at the following times: predose (0), 0.5, 1, 1.5, 2, 4, 6, 8, 12, and 24 h postdose. Blood (10 mL) was collected from each subject via a cannula or by repeated venipuncture into lithium heparin tubes. After centrifugation, plasma was divided into two different tubes and stored at 20 C. A validated LC–MS/MS method was developed for simultaneous quantification of the three major inactive metabolites in human plasma [19]. The metabolites were analyzed following solid-phase extraction. No endogenous component interfered with the quantification. The lower limit of quantification for the three metabolites was 1.56 ng/mL in human plasma. Statistical analyses Descriptive statistics generated using SAS (v 6.07) were used to summarize demographics, laboratory parameters, platelet aggregation, bleeding times, and adverse events by dose group. Dunnett multiple comparisons tests were used to evaluate changes in bleeding times. A non-compartmental model was used to generate pharmacokinetic parameter O O N O N O S F CH3S F *R-100932 Prasugrel O O N O S N HOOC F F HS R-138727 (active metabolite) *R-95913 O HOOC CH3S N F *R-106583 Figure 1. Pathways of prasugrel metabolism. R-138727 was not measured in this study but has been shown to be the pharmacologically active metabolite [18]. Metabolites measured in study. Figure does not illustrate all metabolites of prasugrel that have been identified. 212 F. Asai et al. Table I. Inhibition of platelet aggregation at each prasugrel dose with 5 or 20 mM ADP as agonist. % Inhibition of platelet aggregation (mean SE) Prasugrel dose (mg) Timepoint Placebo (n ¼ 4) 2.5 (n ¼ 5) P-value 10 (n ¼ 5) P-value 30 (n ¼ 5) P-value 75 (n ¼ 5) P-value 5 mM ADP 1h 2h 4h 8h 24 h 48 h 168 h (7 days) 3.8 2.4 28.3 15.4 8.1 5.4 2.2 2.2 14.5 5.5 0.0 2.4 2.4 14.2 5.9 11.5 7.5 5.4 3.8 21.6 9.0 25.0 10.9 N.S.? N.S. N.S. N.S. N.S. 16.2 8.7 18.0 8.2 18.0 7.6 17.5 7.3 29.0 6.2 N.S. N.S. N.S. N.S. N.S. <0.01 <0.05 <0.001 <0.001 <0.001 N.S. 5.3 3.1 N.S. 58.5 11.5 69.4 4.0 71.6 3.8 58.8 2.8 76.0 1.3 61.2 5.0 11.1 5.9 <0.01 <0.05 <0.001 <0.001 <0.001 14.8 6.9 54.7 11.0 69.6 7.5 69.4 6.8 68.2 8.8 72.4 5.3 60.3 7.6 14.5 9.4 20 mM ADP 1h 2h 4h 8h 24 h 48 h 168 h (7 days) 5.9 3.5 6.9 6.9 1.2 1.2 0.0 0.0 6.4 3.9 0.0 1.0 1.0 11.8 5.0 4.0 3.4 2.1 2.1 10.3 5.1 15.4 6.5 N.S. N.S. N.S. N.S. N.S. 11.3 4.9 17.3 9.8 15.5 7.8 12.2 6.6 15.4 7.3 N.S. N.S. N.S. N.S. N.S. 43.5 7.8 59.8 9.9 58.5 6.6 54.8 6.9 60.7 5.7 43.9 8.4 13.0 6.2 <0.05 <0.001 <0.001 <0.001 <0.001 43.2 15.7 57.0 7.2 62.3 4.3 51.3 3.9 63.4 4.9 53.4 6.4 6.3 4.1 <0.05 <0.01 <0.001 <0.001 <0.001 ?? ?? ?? 12.8 6.6 ?? N.S. 10.8 6.5 N.S. ??? N.S. ??? N.S. ??? N.S. ??? N.S. SE, standard error. P-values are for prasugrel dose group comparison to placebo using Dunnett test. ? N.S., no significant difference was observed between prasugrel and placebo with P > 0.05. ?? No sample collection was required at this timepoint. ??? Statistical comparison cannot be performed due to insufficient number of placebo samples at this timepoint. estimates for the three metabolites using WinNonLin pharmacokinetic software (version 1.1, Scientific Consulting Inc., Cary, NC). Summary statistics for the parameter estimates of AUC(0–24h), the area under the plasma drug concentration versus time curve from time 0 to 24 h; Cmax, maximum concentration of metabolite in plasma measured in subject after dosing; Tmax, the time at which Cmax was apparent; and t1/2, plasma elimination half-life for each dose group in the study are presented. Results Subjects Twenty-four healthy male subjects were enrolled in the study of prasugrel administered as single doses of 2.5, 10, 30, or 75 mg (five subjects at each dose and one placebo subject per group). The mean age was 30.4 7.4 years, (range 19.0–48.0 years) and the mean weight was 73.1 9.3 kg (range 59.9–93.2 kg). Safety Adverse events. There were 13 postdose adverse events experienced by seven subjects in this study. None of these events were considered serious. All of the adverse events occurring during administration of prasugrel were considered mild in nature. The adverse events included gastrointestinal disturbances (flatulence, nausea, and vomiting), autonomic disturbances (pallor, sweating increased, and vomiting) and general disorders (rhinitis and superficial cut). Central and peripheral nervous system disorders included dizziness and headache. Dizziness was the most common adverse event (n ¼ 1 at prasugrel doses of 10, 30, and 75 mg), but occurred at the same frequency in the subjects receiving placebo (n ¼ 1). No adverse events were associated with the 2.5 mg dose of prasugrel. Only one event, a mild headache in a subject in the 10-mg dose group, was considered possibly related to administration of study drug. There were no clinically significant changes noted in clinical laboratory evaluations or vital signs in any subject. All ECGs, fundoscopic examinations, and examinations for petechiae were normal. Pharmacodynamics Platelet aggregation. Mean IPA observed in each dose group using 5 or 20 mM ADP as the agonist is listed in Table I. Within 1 h of dosing (shortest study interval) prasugrel, at the two higher doses of 30 and 75 mg, substantial inhibition of platelet aggregation induced by 20 mM ADP was observed (Figure 2 and Table I). At 1 h, the IPA with prasugrel 30 mg was 43.5 7.8% and with prasugrel 75 mg was 43.2 15.7% compared to IPA with placebo of 5.9 3.5% (P < 0.05 for both doses). The degree of inhibition observed at 2 h was slightly higher with both prasugrel 30 and 75 mg (59.8 9.9 and 57.0 7.2%) and was maintained through the subsequent 22 h. While the IPA recovered slightly to 43.9 8.4 and Single oral doses of prasugrel in healthy subjects 213 Maximal platelet aggregation (%) 100 80 60 40 20 0 BL 24 h BL 24 h 75 mg 30 mg Figure 2. Inhibition of ADP-induced platelet aggregation after single doses of prasugrel compared to placebo. Mean inhibition of platelet aggregation (% IPA) at selected timepoints induced by 20 mM ADP is illustrated. Solid circles represent placebo; open circles, 2.5 mg prasugrel; closed squares, 10 mg prasugrel; open squares, 30 mg prasugrel; and solid triangles, 75 mg prasugrel. A 48 h sample was collected only in the prasugrel 30 and 75 mg groups. Values are mean standard error, n ¼ 4 for placebo group, n ¼ 5 for all prasugrel dose groups. 53.4 6.4% for prasugrel 30 and 75 mg by 48 h, full recovery occurred between 48 h and 7 days. At day 7, platelet aggregation had returned to normal levels in both the higher dose groups. At 1 h after dosing, the lower doses of prasugrel, namely 2.5 and 10 mg, had no measurable effect on platelet aggregation as indicated by levels of inhibition indistinguishable from placebo values (P > 0.05 for 2.5 and 10 mg prasugrel versus placebo). The level of IPA observed with 5 mM ADP was slightly greater for any given prasugrel dose (Table I); however, the overall time course of inhibition and subsequent recovery following cessation of drug were very similar to that found with 20 mM ADP. The IPA observed with collagen (2 mg/mL) as the agonist was not as pronounced as with 20 mM ADP (maximum mean IPA observed with prasugrel 75 mg was 30.6% with collagen 2 mg/mL at 24 h vs. 63.4% with 20 mM ADP at 24 h), which suggests that prasugrel or a metabolite is an ADP receptor antagonist resulting in effective inhibition of ADP-induced platelet aggregation, but weaker inhibition of collagen-induced aggregation (data not shown). Figure 3 illustrates the consistency of the response, as measured by maximal platelet aggregation, obtained with prasugrel 30 and 75 mg using either 5 or 20 mM ADP. In all subjects, at 24 h postdose with prasugrel 30 mg, the MPA was reduced to 39% (IPA 42%). With prasugrel 75 mg, the MPA was reduced in all subjects to 38% (IPA 50%). Bleeding time The mean bleeding times at 4 h postdose of prasugrel 30 and 75 mg increased approximately 3- and 4-fold 5 µM ADP BL 24 h 30 mg BL 24 h 75 mg 20 µM ADP Figure 3. Individual ADP-induced platelet aggregation responses before and after single doses of prasugrel. Maximum platelet aggregation (% MPA) at baseline (BL) and 24 h post prasugrel dose (30 or 75 mg) in each subject. Platelet aggregation was induced by 5 or 20 mM ADP and the maximum platelet aggregation level achieved during the 4-min observation period is reported. The horizontal line is the mean MPA for each group. compared to placebo, from 161 s (placebo) to 444 s (P > 0.05) and 682 s (P < 0.05), in the prasugrel 30 and 75 mg groups, respectively (Table II). This change was directionally consistent with the increase in IPA. The mean bleeding times remained elevated at 24 h postdose for prasugrel 75 mg. Pharmacokinetics Pharmacokinetics were studied following single doses of 2.5, 10, 30, and 75 mg. Plasma concentrations of three metabolites determined after administration of prasugrel in the fasting state at a dose of 75 mg are shown in Figure 4, and the pharmacokinetic parameters are listed in Table III. The maximum plasma concentration (Cmax) and the area under the plasma concentration vs. time curve (AUC(0–24h)) of the metabolites increased proportionally to the dose administered, from 2.5 to 75 mg (Figure 5A, B). The correlation coefficients obtained by linear regression analysis for the dose– AUC(0–24h) relationship for R-95913, R-106583, and R-100932 were 0.90, 0.89, and 0.83, respectively. For the dose–Cmax relationship, the correlation coefficients for R-95913, R-106583, and R-100932 were 0.57, 0.69, and 0.60, respectively. The three metabolites appeared in the plasma soon after administration and reached Cmax in approximately 1 h, consistent with the appearance of inhibition of platelet aggregation. The most abundant metabolite was R-106583, which is an S-methylated derivative of the active metabolite (Figure 1). 214 F. Asai et al. Table II. Bleeding times. Time after prasugrel administration 4h Prasugrel dose (mg) Placebo (n ¼ 4) 2.5 (n ¼ 5) 10 (n ¼ 5) 30 (n ¼ 5) 75 (n ¼ 5) 24 h Post-study Mean bleeding time (sec) P-value Mean bleeding time (sec) P-value Mean bleeding time (sec) P-value 161 48 165 61 142 17 444 131 682 166 – N.S.? N.S. N.S. <0.05 120 5 151 17 221 37 272 71 584 203 – N.S. N.S. N.S. <0.05 172 40 121 8 155 8 168 27 157 8 – N.S. N.S. N.S. N.S. Bleeding times are expressed as seconds, mean standard error. *N.S., no significant difference was observed between prasugrel and placebo with P > 0.05. Plasma concentration (ng/ml) 500 R-95913 R-106583 R-100932 400 300 200 100 0 0 4 8 12 Time (h) 16 20 24 Figure 4. Plasma concentration profile of metabolites after administration of 75 mg prasugrel. Concentration of metabolites over time is displayed. Solid triangles represent R-95913, solid circles represent R-106532, and open circles represent R-100932. Values are mean standard error, n ¼ 5 at each timepoint. Discussion This was the first clinical study of the novel thienopyridine antiplatelet agent, prasugrel (CS-747, LY640315) in healthy volunteers. For the safety endpoints studied, the results indicated that prasugrel at the doses and intervals studied appeared to be safe, well tolerated, and obeyed linear pharmacokinetics. The pharmacokinetic and pharmacodynamic results of this study indicate rapid gastrointestinal absorption of prasugrel, which led to sustained and apparently irreversible inhibition of ADP-induced platelet aggregation within 1 h of administration at the doses of 30 and 75 mg of prasugrel. The antiplatelet effects of prasugrel 2.5 and 10 mg could not be distinguished from placebo. Increasing levels of IPA were also associated with a progressive prolongation of the bleeding time. Rapid onset of platelet inhibition was observed at the higher doses of prasugrel 30 and 75 mg. At these higher doses, inhibition of platelet aggregation occurred within 1 h of dosing and continued through 48 h, supporting the irreversible nature of the antagonism of the P2Y12 receptor. These observations and conclusions are consistent with ex vivo results in preclinical animal studies and in vitro human platelet studies [13]. The rapid onset of platelet inhibition could be a potential advantage for prasugrel in the setting of PCI. In addition, there was a marked consistency of response achieved with prasugrel 30 and 75 mg. Although the sample size in this study was small, it is noteworthy that at 24 h postdose with 20 mM ADP as agonist, maximal platelet aggregation achieved with prasugrel 30 mg was reduced to 39% (IPA 42%) in all subjects. With prasugrel 75 mg at 24 h postdose, maximal platelet aggregation was reduced in all subjects to 38% (IPA 50%). Reduced platelet inhibition by prasugrel with collagen relative to ADP as the agonist is consistent with the mode of action of prasugrel or its active metabolite as a purine receptor antagonist that primarily inhibits ADP-induced platelet aggregation. The smaller effect on collagen-induced aggregation reflects the partial role played by the ADP released following platelet stimulation with collagen. Three inactive metabolites of prasugrel were measured in this study, one the precursor to the active metabolite (R-95913) and two downstream metabolites (R-106583 and R100932). The pharmacokinetics of all three metabolites were well described by an integrated population pharmacokinetic model. The maximum plasma concentration of the precursor to the active metabolite and the downstream metabolites appeared approximately 1 h after administration of prasugrel, indicating rapid absorption of the drug and consistent with the appearance of inhibition of platelet aggregation. The most abundant metabolite was the S-methylated derivative of the active metabolite, 106583. Although we did not measure active metabolite in this study, a proportional relationship of the AUC of R-106583 to that of the active metabolite has been observed in other studies (data not shown). The pharmacokinetics of the metabolites and relationship to platelet inhibition Single oral doses of prasugrel in healthy subjects 215 Table III. Pharmacokinetic parameters estimated from single ascending dose study. Prasugrel dose (mg) 2.5 (n ¼ 5) 10 n ¼ 5 30 (n ¼ 5) 75 (n ¼ 5) R-95913 AUC (0–24 h) (ng h ML1) Cmax (ng mL1) Tmax (h) t1/2 (h) 9.2 2.4 7.4 1.2 0.7 0.1 N.A. 53.2 10.6 30.0 6.9 0.8 0.1 5.6 0.9 157.9 22.5 90.8 12.9 0.6 0.1 6.4 1.3 350.8 36.0 117.0 27.5 1.0 0.2 8.8 1.2 R-106583 AUC (0–24 h)(ng h mL1) Cmax (ng mL1) Tmax (h) t1/2 (h) 58.4 8.7 14.6 1.6 0.8 0.1 8.6.1.4 324.5 25.6 71.5 7.7 1.1 0.1 10.2 0.6 969.0 131.3 189.4 23.5 0.9 0.1 8.9 0.5 2686.1 368.4 391.5 91.6 1.5 0.2 11.0 1.7 R-100932 AUC (0–24 h)(ng h mL1) Cmax (ng mL1) Tmax (h) t1/2 (h) 7.4 1.6 5.2 1.1 1.0 0.2 N.A. 62.4 9.7 28.9 3.9 0.9 0.1 3.5 0.7 204.1 17.7 77.8 7.6 0.7 0.1 5.8 1.0 585.1 94.5 163.0 45.3 1.1 0.2 9.1 1.4 N.A., t1/2 was not calculated due to lack of sufficient data points. All data are expressed as mean standard error. AUC(0–24h), the area under the plasma drug concentration vs. time curve from time 0 to 24 h; Cmax, maximum concentration of drug in plasma measured in subject after dosing; Tmax, the time at which Cmax was apparent; t1/2, plasma elimination half-life. Figure 5. Dose response of Cmax and AUC(0–24h). The mean area under the plasma drug concentration versus time curve from time 0 to 24 h (AUC(0–24h), ng h mL) achieved with each dose of prasugrel administered is represented in panel A. Maximum mean concentration (Cmax, ng mL1) of each metabolite in plasma achieved with each dose of prasugrel administered is represented in panel B. The linear regression line for the dose–AUC(0–24h) and the dose–Cmax relationship for each metabolite is illustrated. The correlation coefficients obtained by linear regression analysis for the dose–AUC(0–24h) relationship for R-95913, R-106583, and R-100932 were 0.90, 0.89, and 0.83, respectively. For the dose–Cmax relationship, the correlation coefficients for R-95913, R-106583, and R-100932 were 0.57, 0.69, and 0.60, respectively. Solid triangles represent R-95913, solid circles represent R-106583, and open circles represent R-100932. Values are mean standard error, n ¼ 5 at each prasugrel dose. observed in these studies are consistent with previously published preclinical data indicating that prasugrel is a prodrug that is metabolized to an active moiety that irreversibly inhibits the platelet P2Y12 ADP receptor [13]. Although clopidogrel was not included in this study, previously published studies of clopidogrel using 5 or 20 mM ADP as the platelet agonist demonstrated that the onset of IPA requires approximately 2–4 h for clopidogrel at a loading dose of 216 F. Asai et al. 300 mg [20, 21]. In addition, other clinical studies with clopidogrel 300 mg report a pharmacodynamic nonresponder rate (i.e. change in maximal percent aggregation to 20 mM ADP <10%) of 25–30% [9, 11, 12, 22, 23]. Based on comparison to these clopidogrel studies, a higher level of IPA was achieved with 30 mg prasugrel, a dose 10-fold lower than the wellaccepted clopidogrel loading dose (300 mg). In this study, with prasugrel 30 mg and 20 mM ADP as agonist, a mean inhibition of aggregation of 60.7% at 24 h postdose was observed compared to a mean inhibition of 20–40% in published studies for clopidogrel 300 mg loading dose [20, 21, 24] or a widely variable IPA at 24 h of 30–60% for clopidogrel 600 mg loading dose [20, 24, 25]. The results from this study are consistent with preclinical animal studies indicating prasugrel was an irreversible inhibitor of ADP-induced platelet aggregation with a fast onset of action and a potency approximately 10–15 times that of clopidogrel [13]. Conclusions In this single dose study, prasugrel was well tolerated, achieved a consistent high level of platelet inhibition with a fast onset of action at doses of 30 and 75 mg, and obeyed linear pharmacokinetics at doses of up to 75 mg. There were no serious adverse events and no significant bleeding complications. No abnormal drug effects were observed on safety evaluations in any of the prasugrel dose groups. This initial study supported selection of doses of prasugrel for subsequent multiple dose safety studies of prasugrel in healthy subjects. Acknowledgments The authors would like to acknowledge the assistance provided by Satoshi Fukuda of Sankyo Co. Ltd., in conducting the statistical analyses and the writing and administrative assistance of Barbara Utterback of Eli Lilly and Company in the preparation of this manuscript. Financial support and potential Conflict of Interest The study was supported by Sankyo Co. Ltd., Tokyo, Japan. Drs Asai, Naganuma, and Hirota and Ms Matsushima are employees of Sankyo Co. Ltd., Tokyo, Japan. Drs Jakubowski, Winters, and Brandt are employees and stockholders of Eli Lilly and Company. Sankyo Co. Ltd., and Eli Lilly and Company are currently co-developing prasugrel for potential clinical use. Dr Freestone is an employee of Inveresk Clinical Research Ltd. (now known as Charles River Laboratories). References 1. Bertrand ME, Simoons ML, Fox KA, Wallentin LC, Hamm CW, McFadden E, De Feyter PJ, Specchia G, Ruzyllo W. Task Force on the Management of Acute Coronary Syndromes of the European Society of Cardiology. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2002;23:1809–1840. 2. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Shaeffer JW, Smith EE III, Steward DE, Theroux P. ACC/AHA 2002 guideline update for the management of patients with unstable angina and nonST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). http:// www.acc.org/clinicalguidelines/unstable/unstable.pdf2002. Accessed 5-11-2005. 3. Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. Br Med J 2002;324:71–86. 4. Boersma E, Harrington RA, Moliterno DJ, White H, Theroux P, Van de WF, de Torbal A, Armstrong PW, Wallentin LC, Wilcox RG, Simes J, Califf RM, Topol EJ. Simoons ML. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: A meta-analysis of all major randomised clinical trials. Lancet 2002;359:189–198. 5. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. New Engl J Med 2001;345:494–502. 6. Schomig A, Neumann FJ, Kastrati A, Schuhlen H, Blasini R, Hadamitzky M, Walter H, Zitzmann-Roth EM, Richardt G, Alt E, Schmitt C, Ulm K. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. New Engl J Med 1996;334:1084–1089. 7. Leon MB, Baim DS, Popma JJ, Gordon PC, Cutlip DE, Ho KK, Giambartolomei A, Diver DJ, Lasorda DM, Williams DO, Pocock SJ, Kuntz RE. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. New Engl J Med 1998;339:1665–1671. 8. Sharis PJ, Cannon CP, Loscalzo J. The antiplatelet effects of ticlopidine and clopidogrel. Ann Intern Med 1998;129:394–405. 9. Jaremo P, Lindahl TL, Fransson SG, Richter A. Individual variations of platelet inhibition after loading doses of clopidogrel. J Intern Med 2002;252:233–238. 10. Gurbel PA, Bliden KP. Durability of platelet inhibition by clopidogrel. Am J Cardiol 2003;91:1123–1125. 11. Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrel for coronary stenting: Response variability, drug resistance, and the effect of pretreatment platelet reactivity. Circulation 2003;107:2908–2913. 12. Muller I, Besta F, Schulz C, Massberg S, Schonig A, Gawaz M. Prevalence of clopidogrel non-responders among patients with stable angina pectoris scheduled for elective coronary stent placement. Thromb Haemost 2003;89:783–787. 13. Sugidachi A, Asai F, Yoneda K, Iwamura R, Ogawa T, Otsuguro K, Koike H. Antiplatelet action of R-99224, an active metabolite of a novel thienopyridine-type G(i)-linked P2T antagonist, CS-747. Br J Pharmacol 2001;132:47–54. Single oral doses of prasugrel in healthy subjects 14. Sugidachi A, Asai F, Ogawa T, Inoue T, Koike H. The in vivo pharmacological profile of CS-747, a novel antiplatelet agent with platelet ADP receptor antagonist properties. Br J Pharmacol 2000;129:1439–1446. 15. Niitsu Y, Jakubowski JA, Sugidachi A, Asai F. Pharmacology of CS-747 (prasugrel, LY640315), a novel, potent antiplatelet agent with in vivo P2Y12 receptor antagonist activity. Semin Thromb Hemost 2005;31:184–194. 16. Hirota TP, Sugii H, Asai FP, Kawabata K, Inoue T, Iwamura R, Freestone SM, Dickson JM. Efficacy of cs-747, a new potent and antiplatelet agent. Clin Pharmacol Ther 1999;65:148. 17. Ivy AC, Nelson D, Bercher G. The standardization of certain factors in the cutaneous venostasis bleeding time technique. J Lab Clin Med 1941;26:1812–1822. 18. Jakubowski J, Ogawa T, Sugidachi A. Steroselective inhibition of human platelet aggregation by R-138727, the active metabolite of CS-747, a novel P2Y12 receptor antagonist. J Thromb Haemost 2003;(Suppl):2056 (abstr). 19. Wong E, McIntosh M, Garofolo F et al. Bioanalytical assay for LY640315 (CS-747) three inactive metabolites in human plasma by LC MS/MS. ASMS Annual Meeting. 2004. 20. Muller I, Seyfarth M, Rudiger S, Wolf B, Pogatsa-Murray G, Schomig A, Gawaz M. Effect of a high loading dose of clopidogrel on platelet function in patients undergoing coronary stent placement. Heart 2001;85:92–93. 217 21. Ernst NM, Suryapranata H, Miedema K, Slingerland RJ, Ottervanger JP, Hoorntje JC, Gosselink AT, Dambrink JH, de Boer MJ, Zijlstra F. van’t Hof AW. Achieved platelet aggregation inhibition after different antiplatelet regimens during percutaneous coronary intervention for ST-segment elevation myocardial infarction. J Am Coll Cardiol 2004;44:1187–1193. 22. Gurbel PA, Bliden KP. Interpretation of platelet inhibition by clopidogrel and the effect of non-responders. J Thromb Haemost 2003;1:1318–1319. 23. Gurbel PA, Bliden KP, Hayes KM, Yoho JA, Herzog WR, Tantry US. The relation of dosing to clopidogrel responsiveness and the incidence of high post-treatment platelet aggregation in patients undergoing coronary stenting. J Am Coll Cardiol 2005;45:1392–1396. 24. Gurbel PA, Bliden KP, Zaman KA, Yoho JA, Hayes KM, Tantry US. Clopidogrel loading with eptifibatide to arrest the reactivity of platelets: Results of the Clopidogrel Loading With Eptifibatide to Arrest the Reactivity of Platelets (CLEAR PLATELETS) study. Circulation 2005;111:1153–1159. 25. Kastrati A, vonBeckerath N, Joost A, Pogatsa-Murry G, Gorchakova O, Schomig A. Loading with 600 mg clopidogrel in patients with coronary artery disease with and without chronic clopidogrel therapy. Circulation 2004;110:1–4.