Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adoptive cell transfer wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Molecular mimicry wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Autoimmunity wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
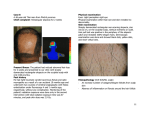
Dermatologic Therapy, Vol. 24, 2011, 364–368 Printed in the United States · All rights reserved © 2011 Wiley Periodicals, Inc. DERMATOLOGIC THERAPY ISSN 1396-0296 Treatment of alopecia areata: “What is new on the horizon?” dth_1421 364..368 Maria K. Hordinsky Department of Dermatology, University of Minnesota, Minneapolis, Minnesota ABSTRACT: New drug treatment opportunities based on the results of a genome-wide association study, which implicate T cell and natural killer (NK)-cell activation pathways, are leading to new approaches in future clinical trials of alopecia areata. Special attention is being given to the UL 16-binding protein (ULBP3) gene cluster on chromosome 6q25, as these genes make the NKG2Dactivating ligand or signal that can trigger the NKG2D receptor, initiating an autoimmune response. A greater expression of ULBP3 has also been found in hair follicles in scalp biopsy specimens from patients with active disease. It is now postulated that the characteristic T cell “swarm of bees” infiltrate seen in alopecia areata is the result of T cells being attracted to the hair follicle by NKG2D-activating ligands. Future treatment approaches for alopecia areata include use of drugs that: (i) block the NKGDactivating ligand and NKG2D receptor interaction, (ii) halt activated T cells, or (iii) modification of the inflammatory cytokine network. Many drugs currently being used or being evaluated for other autoimmune diseases that work through these mechanisms might prove to be very effective in alopecia areata. KEYWORDS: alopecia areata, clinical trials, genome-wide association study (GWAS) Introduction Alopecia areata is a complex genetic, immunemediated disease that targets anagen hair follicles (1). Characterized by round or oval patches of hair loss, loss of all scalp hair (alopecia totalis), loss of all body hair (alopecia universalis), or ophiasis pattern hair loss, alopecia areata is a relatively common autoimmune disease that affects both males and females of all ages and races in all parts of the world. The lifetime risk for alopecia areata in the United States is estimated to be approximately 2% (2). Unfortunately, there is currently no cure for this chronic disease and, although many therapies are available, there is no universally proven therapy that induces and sustains remission (3). In the United States, there is no FDA-approved therapy for the treatment of alopecia areata, so treatments Address correspondence and reprint requests to: Maria K. Hordinsky, MD, Professor and Chair, Department of Dermatology, University of Minnesota, Minneapolis, MN 55455, or email: [email protected]. 364 are considered “off label.” Current treatment choices are frequently based on disease extent and duration, as well as the age of the patient. Treatments include a variety of topical, intralesional, and systemic agents (1,4). Pathophysiology A histopathologic hallmark of alopecia areata is the presence of perifollicular inflammation and in particular, a peribulbar infiltrate of predominantly lymphocytes around anagen follicles (5). This infiltrate is commonly referred to as a “swarm of bees” and is typically seen in patients with active disease (FIG. 1). When alopecia areata is more chronic this infiltrate may not be a striking feature, rather a shift to the telogen stage of the hair cycle or follicles in early anagen predominates (FIG. 2). Transplantation studies using severe-combined immunodeficient mice have established that alopecia areata is transferrable with T cells (6). There is also evidence to suggest that immune privilege is lost in alopecia areata (7,8). Treatment of alopecia areata FIG. 1. “Swarm of bees” around an anagen hair follicle in a scalp biopsy taken from a patient with alopecia areata. treatment of choice for many dermatologists and in uncontrolled studies variable rates of response have been found (1,4,9). Second-line therapies for alopecia areata include topical minoxidil, anthralin, and phototherapy with psoralen plus near ultraviolet light (UVA) therapy. Additional second-line therapies include systemic treatment with oral glucocorticoids, sulfasalazine, cyclosporine, methotrexate, or combination therapy (1,4,9). Other therapies that have shown some efficacy include the excimer laser, topical bexarotene, photodynamic therapy, prostaglandin analogs, and even fractional photothermylysis (1,4,9). Aromatherapy, a natural treatment option, has also been reported to be effective in some patients (10). Although there are isolated case reports of different biologics being effective in the treatment of alopecia areata, attempts to treat this disease with biologic agents that directly or indirectly alter T cell function have not proven to be successful in clinical trials. In studies examining: (i) alefacept, a fusion protein that binds to CD2 and inhibits T cell activation, (ii) etanercept, a tumor necrosis factoralpha inhibitor, or (iii) efalizumab, a recombinant humanized monoclonal antibody against CD11a, none has been shown to be effective in clinical trials. Of note, the manufacture of efalizumab has since been discontinued. Moreover, alopecia areata has been described to develop in patients while on therapy with adalimumab, infliximab, or etanercept for other autoimmune disorders (1,4,9). What is new on the horizon? FIG. 2. Shift to telogen and miniaturized follicles in a scalp biopsy taken from a patient with a several-year history of extensive alopecia areata. The inflammatory infiltrate is still present, but is not as prominent as seen in patients with acute, active disease. Current treatments (1,4,9) First-line therapies of alopecia areata commonly include intralesional or topical corticosteroids, and in some institutions, topical immunotherapy. There are no randomized trials of intralesional corticosteroids for alopecia areata; however, there are several published studies investigating the efficacy of topical corticosteroids in the treatment of this disease. Topical immunotherapy, the preferred In August 2009, scientists and clinicians with an interest in alopecia areata and major autoimmunity experts met in Denver, Colorado at a meeting sponsored by the National Alopecia Areata Foundation. The major goal of this one-day meeting was to develop future research directions and opportunities for alopecia areata. There were four major outcomes from this meeting, one being the identification of new potential therapies. The other three outcomes focused on the determination of key areas for future research, formation of research teams to immediately address key gaps in the knowledge of immune mechanisms in alopecia areata, and the development of funding strategies to engage the hair research and autoimmunity world in alopecia areata research. At the end of the meeting, a group of investigators interested in clinical trials/clinical research was created. The charge given to this group was to 365 Hordinsky review and develop clinical trials using devices as well as off-the-shelf treatments found to be effective in other autoimmune diseases. Those devices and treatments were chosen based on the knowledge of the immunology and genetics of alopecia areata. A comprehensive review of all FDA-approved drugs as well as those in clinical trials for autoimmune diseases was undertaken. Over 230 drugs were identified, and information was obtained on generic drug name, trade names, indications, mechanism, manufacturer (drug company), study phase, and information as to whether or not the drug was FDA-approved. Concurrently, a date was set for a Clinical Research/Translational Summit on Alopecia Areata. This took place October 23, 2010 at Columbia University in New York City and brought together leaders in alopecia areata clinical research, as well as those in drug delivery, immunology drug development, and experts from the National Institutes of Health. The discussions at the Summit focused on several subjects including those summarized in Table 1. Incorporated into the discussion of the Summit were the results of the recently published genome-wide association study (GWAS) and discussion of new drug treatment opportunities based on the results of these studies, in which T cells and natural killer (NK)-cell activation pathways were implicated (11). The stage was set for not only new approaches in clinical trials, but also plans for developing a translational platform with biomarkers. Key findings from the GWAS (12) Key genes that were found in the GWAS studies are summarized in Table 2 and include T cell related genes such as IL2/IL21 (T-, B-, and NK cell proliferation), IL2RA (T cell proliferation), CTLA4 (T cell proliferation), IKZF4 (T cell proliferation) and HLA (antigen proliferation), and genes in the hair follicle including NK-activating ligands ULBP3 and ULBP6, as well as two other hair follicle genes, STX17 and peroxiredoxin V (PRDX5). A major new finding was the identification of cytomegalovirus UL16-binding protein (ULBP3) gene cluster on chromosome 6q25.1. STX17 encodes a member of the syntaxin family; syntaxins are involved in vesicle transport. PRDX5 is an intracellular antioxidant enzyme (11). The importance of the ULBP genes is that they make the NKG2D-activating ligand or signal that can trigger the NKG2D receptor, which, in turn, can initiate a response and more NKG2D-activating ligands or signals providing an opportunity to trigger autoimmunity. This is now postulated to be 366 Table 1. Alopecia areata clinical research summit – summary of subjects covered 1. Need for safe and effective treatments for alopecia areata 2. Definition of quality of life issues 3. Review of what worked and what did not work in past clinical studies of alopecia areata 4. Insights into immune targets for alopecia areata 5. New treatment opportunities based on drugs being developed for other autoimmune diseases 6. New treatment opportunities for devices for alopecia areata patients 7. Review of different drug delivery methods 8. Standardization of all future alopecia areata clinical trials in organization, selection of patients, and regrowth measurement Table 2. Summary of genes implicated in alopecia areata from the GWAS studies 1. Immune system • T cell related genes IL2/IL21, IL2RA, CTLA4, IKZF4, HLA 2. In the hair follicle • NK-activating ligands ULBP3, ULBP6 • Other hair follicle genes STX17, PRDX5 a possible mechanism for alopecia areata as well as other autoimmune diseases. Subsequent immunohistochemical studies on affected alopecia areata scalp, as well as normal scalp, have found higher levels of ULBP3 expressed in the hair follicles of patients with an active disease. This new information has been integrated to suggest that alopecia areata is related to the “swarm of bees” that has characterized this disease for decades. However, the bees have now been identified as killer CD8 cells, which are attracted to the hair follicle by the NKG2D-activating ligand. These findings have opened new avenues of exploration for therapies based on the underlying mechanisms of alopecia areata, permitting treatments to be developed on what we have known, including mechanisms common to other types of autoimmunity and T cell related mechanisms that involve signaling pathways downstream of the NKG2D receptor (5,11). New trends Proposed treatment approaches to alopecia areata now fall into three broad categories and can Treatment of alopecia areata Table 3. Potential therapies to test in clinical trials 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Anti-CD25 Anti-CTLA-4 Jak 1/2 inhibitor Anti-NKG2D Syk inhibitor Anti-IL-15 Anti-IL-6 Anti-IFNg Anti-TAP2 Anti-IL-1 Anti-IL-17 Anti-PDE4 include drugs already being used effectively in many autoimmune diseases. The three approaches could do any of the following: 1. Block NK cell innate immunity 2. Halt activated T cells 3. Modify the inflammatory cytokine network Approaches discussed at the Summit included blocking the innate/NKG2D response (UBLP3, UBLP6, and MICA) and/or antigen presenting cells/sentinel (HLA, TAP, and IFN-g) targeting adaptive immunity such as IL-15, which drives the NKG2D axis and itself could be a good target or the use of Jak inhibitors, which might block TH1 cytokines that are postulated to drive alopecia areata (12–14). There are multiple drugs currently being evaluated for other autoimmune diseases that could potentially be very effective in alopecia areata providing new treatment opportunities. For drugs that are not yet FDA-approved, the consensus from the Summit was that the selection and study of drugs in Phase III of development would be most practical. From the discussions at the Summit and after careful review of approximately 238 drugs in different phases of development or already approved by the FDA in the United States for the treatment of autoimmune diseases, a short list of potential systemic or topical choices to study in alopecia areata was generated. Most of these are antibodies or peptides that block specific immune functions and are summarized in Table 3. Summary: the alopecia areata treatment development program In September 2000, the National Institute of Arthritis, Metabolism and Skin Diseases funded a 10-year Alopecia Areata Registry project with a continuation phase through September 2011. The primary goals of the Registry have been to collect epidemiology data and DNA samples from alopecia areata patients for the purpose of immunogenetic research (15). As of the first quarter of 2011, there were almost 8000 patients and controls who had completed an online registration for first tier information and who agreed to be contacted for possible future clinical trials. There are also greater than 3000 serum and DNA samples from patients who have been carefully characterized by phenotype, disease duration, and treatments. These samples come from patients who participated in the second tier of the Registry and who were either seen by their dermatologists or in most cases, at one of five study sites – MD Anderson, Columbia University or the Universities of California, San Francisco, Colorado, or Minnesota. Upon completion of the project in September 2011, the Registry could potentially expand to a Clinical Trials Network. It is this population of patients as well as patients in clinical practices who will be recruited for the clinical trials and testing of selected new treatments based on the immunology and genetics of alopecia areata. The results of such clinical research studies should define more effective therapies and longer lasting remissions in pediatric and adult patients affected with alopecia areata. References 1. Alkhalifah A, Alsantali A, Wang E, et al. Alopecia areata update. J Am Acad Dermatol 2010: 62: 191–202. 2. Safavi KH, Muller SA, Suman VJ, et al. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc 1995: 70: 628–633. 3. Delamere FM, Sladden MJ, Dobbins HM, et al. Interventions for alopecia areata. Cochrane Database Syst Rev 2008: (2): Art. No.: CD004413. DOI: 10.1002/14651858.CD004413. pub2. 4. Messenger AG. Management of alopecia areata. In: Basow DS, ed. Up to date. Waltham, MA: UpToDate, 2011: Available at http://www.uptodate.com/contents/ management-of-alopecia-areata [Accessed June 3, 2011]. 5. Whiting DA. Histopathologic features of alopecia areata: a new look. Arch Dermatol 2003: 139 (12): 1555–1559. 6. Gilhar A, Ullmann Y, Berkutzki T, Assy B, Kalish RS. Autoimmune hair loss (alopecia areata) transferred by T lymphocytes to human scalp explants on SCID mice. J Clin Invest 1999: 101: 62–67. 7. Kang H, Wu W, Lo B, et al. Hair follicles from alopecia areata patients exhibit alterations in immune privilegeassociated gene expression in advance of hair loss. J Invest Dermatol 2010: 130 (11): 2535–2537. 8. Paus R, Ito N, Takigawa M, et al. The hair follicle and immune privilege. J Invest Dermatol Symp Proc 2003: 8: 188–194. 367 Hordinsky 9. Hordinsky MK, Caramori APA. Alopecia areata. In: Hordinsky M, McMichael A, eds. Hair and scalp diseases: medical, surgical and cosmetic treatments. London UK: Informa Healthcare, 2008: 92–105. 10. Hay IC, Jamieson M, Ormerod AD. Randomized trial of aromatherapy. Successful treatment for alopecia areata. Arch Dermatol 1999: 135: 602–603. 11. Petukhova L, Duvic M, Hordinsky M, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature 2010: 466: 113–117. 12. Freyschmidt-Paul P, McElwee KJ, Hoffmann R, Sundberg JP, Vitacolonna M, Kissling S. Interferon g deficient mice 368 are resistant to the development of alopecia areata. Br J Dermatol 2006; 155: 515–521. 13. Verstovsek S, Kantarjian H, Mesa RA, et al. Safety and efficacy of INCB018424, a JAK1 and JAK2 inhibitor in myelfibrosis. N Engl J Med 2010: 363: 1117–1127. 14. Von Bubnoff D, Hentges AE, Bieber T, Zimmer MT. Natural killer cells in atopic and autoimmune diseases of the skin. J Allergy Clin Immunol 2010: 125: 60–68. 15. Duvic M, Norris D, Christiano A, Hordinsky M, Price V. Alopecia areata registry: an overview. J Investig Dermatol Symp Proc 2003: 8 (2): 219–212.