Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Magnesium transporter wikipedia , lookup
List of types of proteins wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Hedgehog signaling pathway wikipedia , lookup
Protein moonlighting wikipedia , lookup
Protein phosphorylation wikipedia , lookup
Protein (nutrient) wikipedia , lookup
Nuclear magnetic resonance spectroscopy of proteins wikipedia , lookup
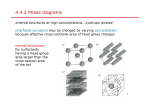
11. ORGANOGENESIS IN GASTROINTESTINAL AND RESPIRATORY SYSTEMS Major Period of Organogenesis Do I need to know this? Splanchnic mesoderm in GI tract development Neural crest cells and mesodermal roles in tissue and organ development in the GI tract Some neurons derive from neural crest cells Other pacemaker cells including Interstitial Cells of Cajal (ICC) come from mesoderm Early gut tube with emphasis on septum transversum Distinct vascularization of foregut midgut and hindgut Origins of the respiratory tract: a dorsal-ventral patterning problem Left-side view Ventral view Ventral view Branching mechanisms in the lung regulated by FGF and Sonic hedgehog signaling Figure 22-92a Molecular Biology of the Cell (© Garland Science 2008) “Normal neonatal chest radiograph” Lung maturation A crucial event in the maturation of lungs and pulmonary function is the onset of surfactant production. Surfactant is a mixture of phospholipids, neutral lipids and proteins synthesized by type II pneumocytes by the end of gestation. 60% of surfactant is dipalmitoylphosphatidylcholine (DPPC), also Called dipalmitoyllecithin. Surfactant protein A (SP-A), surfactant protein B (SP-B), surfactant protein C (SP-C) and surfactant protein D (SP-D) are evolutionarily conserved and expressed in mice and man. During the third trimester the fetal lung synthesizes primarily sphingomyelin, and lung cells convert the majority of their stored glycogen to fatty acids and then to dipalmitoyllecithin. Fetal lung maturity can be determined by measuring the ratio of lecithin to sphingomyelin (L/S ratio) in the amniotic fluid. An L/S ratio less than 2.0 indicates a potential risk of RDS. The risk is nearly 75-80% when the L/S ratio is 1.5. Surfactant functions and RDS The role of surfactant in gas exchange includes lowering of surface tension at the air water interface to prevent collapse of terminal alveoli and small airways, and to prevent movement of fluid into the alveolus. Other roles of surfactant are thought to include enhancement of mucous clearance and stimulation of host lung immunological defences. Small airway and alveolar collapse can result in infant respiratory distress syndrome (RDS), also called hyaline membrane disease. Chest X-ray in respiratory distress syndrome Surfactant production can be induced by administration of corticosteroids to the mother (over a period of about 24 hours) prior to delivery of infants between 26-34 weeks. Post-natally, aerosolized surfactant can be administered to infants with suspected RDS. From the 1960’s until recently, the protein components of surfactant therapy were derived from animal extracts (bovine or porcine). Recombinant surfactant protein is now the standard. Surfactant therapy carries some risk, however, which will be discussed in the upcoming lecture on perinatal development and birth. In rare instances, a fatal homozygous recessive familial condition results in deficiency of the protein components of surfactant, like surfactant protein B (hereditary surfactant protein B deficiency). This deficiency also affects processing of SP-B and phospholipids, both in experimental mouse models and in humans. Bile breaks down lipids (as you will learn) so aspiration of bile can lead to reduced surfactant function. You will learn more about surfactant in pulmonary physiology and in lectures on perinatal development and birth. Rotation and growth of the GI tract to achieve asymmetry: stomach and duodenum Transverse view of the GI tract at the level of the stomach Swallowing, amniotic fluid, polyhydramnios, oligohydramnios Polyhydramnios - too much Oligohydramnios - too little Regulation of blood and immune system by GI organs; the spleen Radiographic view of the normal upper GI tract with ingested contrast agent FGF signaling directs ‘bi-potent’ endoderm toward liver and away from pancreas development Normal pancreas development Normal pancreas development Pancreas functions Exocrine: digestive enzymes (acini) and bicarbonate (ducts) Endocrine: islet hormones, principally insulin and glucagon Note relation of pancreatic duct to liver bile duct Case history Radiographic view of the GI tract with ingested contrast agent in this case The intestines constitute the largest immune organ and one of the largest endocrine organs; so big they ‘herniate’ transiently while turning: ‘physiological herniation’ Views of the normal appendix and pathology including appendicitis Normal gut turning Enterohepatic bile cycle Pyloric sphincter stenosis