Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Breast development wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Growth hormone therapy wikipedia , lookup
Hypothalamus wikipedia , lookup
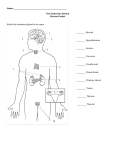
Endocrine System Chapter 16 The Endocrine System • Specialized glands throughout the body • Regulates metabolic activity – Secrete hormones into ECF • Slow acting • Long living • Act on target cells – Signaling molecules • Other tissues produce hormones too Categories of Hormones • Amino acid based – Chains of AA’s – Not membrane soluble (hydrophilic) – Regulatory G proteins and 2nd messengers – e.g. oxytocin, insulin, and prolactin – e.g. epinephrine, norepinephrine, and thyroxine – Derived from AA tryptophan and tyrosine • Steroids – Lipids made from cholesterol – Membrane soluble (hydrophobic) – Direct gene activation – e.g. testosterone, estrogen, and cortisol Amino Acid Action (cAMP) • Binds to PM receptors (1st messenger) – Conformation change binds inactive G protein – Activated by GTP replacing GDP • Active G protein binds to adenylate cyclase (effector) – Stimulatory (Gs) or inhibitory (Gi) – cAMP (2nd messenger) from ATP • cAMP activates protein kinase A – Phosphorylates proteins causing signaling cascade • Target cell specificity produces/inhibits hormone production – Phosphodiesterase rapidly degrades Amino Acid Action (PIP2) • Binds to PM receptors (1st messenger) – Conformation change binds inactive G protein – Activated by GTP replacing GDP • Active G protein binds to phospholipase C (effector) – Stimulatory (Gs) or inhibitory (Gi) – DAG and IP3 (2nd messengers) from PIP2 • DAG activates protein kinase C • IP3 triggers Ca2+ (2nd messenger) release Steroid Action • Binds to intracellular receptors • Hormone-receptor complex binds to DNA – Activates or inhibits – Gene transcription (mRNA production) • mRNA translated into proteins Hormonal Functioning • Stimulating release – Humoral: concentration of ions & nutrients in blood • Drop in Ca2+ signals PTH or increased glucose signals insulin – Neural: nerve fibers • Stress (SNS) signals NE and Epi – Hormonal: other endocrine gland secretions • Hypothalamus signals anterior pituitary • Interactions at target cells – Permissiveness: requirement of 1+ hormone for full effect • Reproductive hormones need thyroid hormone – Synergism: 1+ hormone produces same effect both amplifies • Glucagon and epinephrine signal liver to release glucose – Antagonism: hormones oppose one another • Glucagon increases and insulin decreases blood glucose levels • Generally regulated by negative feedback – Oxytocin is positive feedback Pituitary Gland • Posterior lobe is neural tissue – Store hypothalamic hormones – Exocytic release on demand • Anterior lobe is glandular tissue – Produce hormones – Release of hormones to blood portal system • Hypothalamic control • Releasing or inhibiting hormones Posterior Lobe • Oxytocin – Uterine contractions (smooth muscle) – Milk letdown (glandular muscle) – Sexual arousal, satisfaction, and ‘bonding’ behavior in males & nonlactating females • Antidiuretic hormone – Water balance and loss – Vasoconstriction of visceral blood vessels • Raises blood pressure vasopressin Anterior Lobe • Tropic hormones – – – – TSH ACTH FSH LH • Non-tropic – GH – PRL – Melanocyte-stimulating hormone (MSH): controls appetite Growth Hormone • Growth hormone releasing (GHRH) and inhibiting (GHIH) hormones regulate • Increase size of multiple target cells – Promotes protein synthesis/growth • Primarily skeletal muscle mass and bone length – Metabolic effects (glucose conservation) • Mobilize fat from adipose • Hypersecretion – Gigantism: in children; tall stature w/ normal body proportions – Acromegaly: in adults; disproportionately large hands, feet, face • Hyposecretion – Pituitary dwarfism: in children; short stature w/normal body proportions • TSH, LH, and FSH reduced can misproportioned and/or delay sexual maturity • Artificial production w/ pros and cons Prolactin • Prolactin inhibiting hormone (PIH) regulates • Stimulates milk production – Rise and fall w/ estrogen levels in females • Breast tenderness prior to menstrual period • Elevates at end of pregnancy; suckling maintains – Role in males is not understood • Hypersecretion – Inappropriate lactation, lack of menses, impotence in males • Hyposecretion only problem for nursing females Thyroid Gland • Thyrotropin-releasing hormone (TRH) regulates TSH release to regulate • Anatomy – Bilobed structure w/connecting isthmus – Composed of follicles surrounded by follicular cells w/ thyroglobin • Colloid in lumen is thyroglobin bound to iodine thyroid hormone – Parafollicular cells w/i follicular epithelium secretes calcitonin • Inhibits osteoclast activity and Ca 2+ release; stimulates Ca 2+ uptake Thyroid Hormone (TH) • Most processes in body (table 16.2) – Steroid hormone action – Oxidizes glucose to up metabolic rate & heat production – Maintains blood pressure – Regulates tissue growth and development – Skeletal and nervous system development – Reproductive maturation • Thyroxine (T4) primarily produced, but converted to triiodothytonine (T3) by targets Thyroid Imbalances • Hypothyroidism – Myxedema in adults • Low metabolic rate, chills, dry skin, puffy eyes, lethargy, edema – Goiter from lack of iodine • Gland enlargement – Cretinism when severe in infants • Mental retardation and short, disproportionate body • Hyperthyroidism – Graves’ disease from autoimmune attack of follicle cells • Elevated metabolic rate, sweating, rapid heart rate, weight loss, protruding eyeballs Adrenal Gland • Adrenal cortex is glandular tissue – Long-term stress responses • Corticosteroids derived from cholesterol – Corticotropic releasing hormone (CRH) regulates ACTH to regulate • Adrenal medulla is neural tissue – Short-term stress responses • Epinephrine (Epi) • Norepinephrine (NE) – Hypothalamic neural signal (SNS) Adrenal Cortex • Zona glomerulosa produce mineralcorticoids – Aldosterone (chpts. 25 & 26) • Zona faciculata produce glucocorticoids – Cortisol stimulates gluconeogenesis – Excessive levels cause antiinflammatory and –immune functions • Zona reticularis produce sex steroids (androgens) – Onset of puberty, hair production, and sex drive in women – Testosterone (and estrogen) precursors Adrenal Cortex Imbalances • Hyposecretion – Addison’s disease (mineral- and glucocorticoids) • Loss of weight, drop in glucose and Na+, increase in K+ • Dehydration and hypotension are common • Hypersecretion – Cushing’s disease (glucocorticoids) • Chronic elevated blood glucose, loss of muscle and bone, H2O and NaCl retention • Hypertension, edema, swollen face, neck hump, bruise tendency – Masculinization prepubescently (sex steroids) • Strong sex drive in males • Masculine body hair patterns and clitoris resembling a penis in females Adrenal Medulla • SNS regulates • Secrete epinephrine (Epi) and norepinephrine (NE) – Similar effects – Tyrosine dopamine NE Epi • Hypersecretion increases SNS effects Gonads • Gonadotropin-releasing hormones (GnRH) regulates FSH and LH to regulate • Ovaries and testes contain all types, but ratios vary – Estrogens (estradiol) • • • • Maintain female system Development of 2° sex characteristics Derived from androgens Masculinize male brain in early development – Progesterone • Prepare and maintain uterus • Breast development • Can be converted to testosterone – Testosterone • Maintain and stimulate development of male system • Development of 2° sex characteristics and sex drive • 7th week level determines sex Parathyroid Gland • Tiny glands on the posterior thyroid • Chief cells secrete parathyroid hormone (PTH) – Regulates blood Ca2+ levels (fig 16.12) • Skeleton: stimulates osteoclast activity • Intestine: increases Ca2+ reabsorption (vitamin D) • Kidneys: activates vitamin D and enhances Ca2+ reabsorption in nephrons • Hyperparathyroidism is rare – Ca2+ leaches from bones causing softening and deformation – Elevated Ca2+ depresses nervous system and kidney stones form • Hypoparathyroidism – Low Ca2+ levels increases excitability of neurons Pancreas • Acinar cells produce enzyme rich digestive juices • Islets of Langerhans produce hormones – Alpha (α) cells produce glucagon w/ fasting – Beta (β) cells produce insulin w/feeding Diabetes Mellitus • Blood glucose levels high after feeding • Type I (insulin dependent) – Autoimmune disease – WBC’s attack beta cells (hyposecretion) • Type II (non-insulin dependent) – Older onset – Cells can’t use insulin (hypoactivity) Other Hormone Producing Structures • Heart: ANP reduces blood pressure, volume, and [Na+] • GI tract: enteroendocrine cells release local digestive hormones (gastrin, secretin, CCK) • Placenta: human chorionic gonadotrophic (hCG) to sustain fetus and pregnancy • Kidneys: secrete erythropoietin (EPO) to signal erythropoiesis Other Hormone Producing Structures • Skin: choleocalciferol produce precursor of vitamin D • Adipose tissue: leptin signals stored energy levels and satiety; increase activity levels • Thymus: large in children, diminishes in size w/age; thymosin and thymopoietins stimulate T-cells • Pineal gland: releases melatonin to regulate rhythmic variation of physiological processes