Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
5-HT3 antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
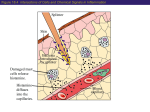
FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 1 of 6 Note: in a couple of the drawings he referred to things in the audio but did not say the name of what he was referring to so I could not identify what he was pointing out in the drawings I. II. III. IV. V. Introduction on Antihistamines [S1]: All of you are familiar with the use of anti-histamines just from over the counter treatment of runny nose, rhinitis, and so on and so we will talk about how those drugs and we will recognize different classes of those drugs and then after that we will talk about the Leukotriene inhibitors which are cousins of anti-histamines and are used in a lot of the same situations Mast Cell Mediators [S2] – a. Mast cells are little bags of mediators and their job is sit around in the body and wait to be activated, upon which they will release things that have short, long, and intermediate actions; most of those actions are protective for us and they serve a good purpose; when they are triggered in a way that’s excessive or they are triggered by a stimulus that creates problems for us we can sometimes use drugs to block the actions of the mediators that are released from mast cells; the number one component released from mast cells is histamine b. Histamine goes out into your blood stream and finds histamine receptors (H1 and H2 are the most common) i. we have drugs that are specific for one type of histamine receptor and some that bind to several different histamine receptors c. Enzymes like tryptase, chymase, proteases are also released from mast cells d. Lipid-derived mediators: (also released from mast cells) i. Prostaglandins (ex// PGD2) ii. Leukotrienes (LTC4) – we will focus on these today iii. Platelet activating factor iv. Cytokines – proteins that are released from mast cells and they interact with other cells particularly in the blood stream to activate them to get further involved in the inflammatory process; so, you get a cascade of events e. One of the cardinal signs of mast cell action is that the initial trigger causes these cells to release their mediators which then go out into the rest of the system and multiply; when we think of an antihistamine effect we tend to think of anaphylaxis i. The reason that one has an anaphylactic response as opposed to a runny nose is due to the amount of histamine that’s released and the rate at which it’s released ii. Our body has ways of getting rid of histamine iii. A small amount of histamine released from mast cells in our nose will cause a runny nose; if we have a large amount of histamine released (like if you are allergic to a bee sting) we get mass amounts of histamine released and our body can’t remove all of it all at once so then we have effects all over the rest of our body and we end up with anaphylactic shock and a tremendous loss of blood pressure f. We usually deal with the effect of histamine locally with antihistamines drugs; it’s all about how much and how fast histamine is released Picture of [S3] – a mast cell is shown here with the little bags or storage vesicles that are full of mediators; they are at rest; your lungs have a lot of these cells along with your blood stream; they are waiting to be primed and release these chemicals Mast Cell Activation[S4] – what triggers a response: a number of different things a. IgE-mediated (“allergic”) response – these are primary mediators of it i. Pollen; if you have ragweed or hay fever you get inhaled pollen that will trigger a response; some people are allergic to food, drugs, or insects etc.; all these different stimuli can stimulate the release of histamine and other mediators b. Anaphylatoxins (C5a) c. Direct release by certain drugs (like opiates in old people) d. Physical stimuli (heat, cold, trauma) i. If you are hit in the nose it will swell up and turn red because you have mast cells lining your nose; this is meant to be a beneficial thing to bring other cells to the site of injury to help repair the area; so again, mast cells and histamines are mediators that we sometimes think of as bad guys but in reality they are a part of a normal natural defense mechanisms; when they are overstimulated or inappropriately stimulated (like with ragweed or hay fever) this is when they are bad e. Some people can have an autoimmune response (chronic urticaria) – people will get a rash caused by, among other things, histamine Histamine [S5] – it’s a chemical that’s a 1st cousin of histidine (one of our normal amino acids); if you decarboxylate histidine you will get histamine; inside your cells you do this all the time and in most cells the histamine doesn’t stick around it gets broken down but in mast cells and in basophils there is storage of histamine inside these vesicles where it’s not broken down so that it can accumulate in these cells a. High concentrations are found in skin tissue, mucosa of the bronchial tree and the intestinal tract FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 2 of 6 b. Has no clinical use for histamine; we don’t give histamine in anybody to treat anything; if we did give it intravenously, it would have a very short 1/2 life c. Released after interaction of Ag with IgE Abs; and again, these same things, pollen, foods, drugs insect bites, etc. … he didn’t finish his thought but I think he was referring to these things acting like Ags and our Abs binding to them d. 2 different histamine receptors: H1 and H2 (we are going to ignore anything outside of these 2) e. Most storage occurs in basophils and mast cells f. The immediate pharmacological effects are itching, increased permeability, vasodilatation that is causing redness, smooth muscle contraction, and gastric acid secretion i. Notice that in the above list all but gastric acid secretion, are all receptors; H2 receptors are associated with gastric acid secretion; these 2 are distinct so our use of anti-histamines are distinct; we use one class of drugs to treat the effects of H1 receptors and we use another class of drugs to treat the effects of the H2 receptors VI. Histamine [S6] – Test Question: will always be distinguishing between the H1 effect and a H2 effect; a. H1 is always everywhere else b. H2 is always the one in the stomach VII. Systemic Effects [S7] and [S8] – what do they do systemically? Their effect is to vasodilate small blood vessels. So, again for example, the blood vessels in your nose dilate, you get edema, you get congestion as a result of that; it can lead to a lowering of systemic blood pressure; this can occur most with H1 and H2 receptors but H1 is primarily the one we think of increasing capillary permeability and then the nasal congestion being the cardinal sign a. The one that we intervene with a lot with our anti-histamine drugs are the H1’s b. Conventionally when people are using a broad term anti-histamine they usually are talking about an H1 blocker; usually when we talk about H2 blockers you specifically say it’s an H2 blocker; because H1 and H2 both are found in your body you shouldn’t just use that term, but if someone just says anti-histamines, they often times are inappropriately talking just about anti H1’s c. In your lungs, bronchiolar smooth muscle are constricted by H1 so if you have a person who is having an allergic reaction or who is having an overly aggressive response to a pollen, what’s the effect on their lungs? i. They would constrict their lungs so breathing will become difficult; so when you have an allergic reaction to a bee sting, one of the ways you would die would be the inability to breathe you would get really severe bronchial constriction ii. How would you intervene to try to overcome this? You could give a person like that a bronchodilator or you could give an anti-histamine, but usually for an emergency you give epinephrine which binds to beta-2 adrenergic receptors in the lungs to make them dilate iii. Histamine has an opposing effect through a different receptor; so you can use epi to try and counter-effect the effect of histamine there d. Histamine causes contraction of smooth muscle in the gut and causes a gastric acid secretion in the stomach; you can think of this as a normal part of our digestive system; if we have overstimulation of this and too much histamine secretion you could have cramping and diarrhea, vomiting, GI distress and the overproduction of gastric acid would lead to acid reflux (many people are troubled at night by overproduction of gastric acids as a result of histamine stimulation and they wake up with burning in their esophagus); this is where we can intervene with an anti-H2 drug e. We stimulate nerve endings with itching and pain; if you have hay fever, or pollen problems the itchy nose, redness, and watery eyes are irritating and so an anti-histamine can help these symptoms VIII. Allergic Diseases [S9] – All of these processes below have histamine playing a role in them, and histamine is not the only character in this response but it’s one of the big ones a. Allergic rhinitis (hay fever) b. Atopic dermatitis (eczema) c. Urticaria d. Asthma e. Anaphylaxis IX. Picture of a little guy sneezing his brain out [S10] X. Allergic Rhinitis: Epidemiology [S11] – a. A lot of Americans have it; often it improves with age; you can have dust, pets, family history, all of these things can contribute to it; it’s not a life threatening condition but it’s one that we do seek a lot relief for XI. Picture of a girl wiping her nose with her hand [S12] – she developed a little crinkle in her nose because she is constantly wiping her nose; so the doctor is likely to think the patient has allergies if they have a crinkle in their nose XII. Antihistamines in Allergic Rhinitis [S13] – a. The symptoms are sneezing, puritis, rhinorrhea, congestion, late-phase reactions; we can use anti-histamines to block these first 3; they may have some effect on congestion FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 3 of 6 i. Late phase reactions are probably caused by interleukins and similar things released from mast cells and basophils and going to other cells recruiting them to the site ii. So, antihistamines don’t prevent the late phase reactions, they prevent the effects of histamine which are the earlier effects b. This is kind of a temporal sequence of events; histamine gets released and it causes sneezing, red eyes, runny nose, etc and then the interleukins are released to other cells like white blood cells that will come to the site of injury or irritation; so these later effects will not be treated effectively by anti-histamines XIII. Reduction of histamine effects [S14] – a. Epi can be used if you have an anaphylaxtic response; it has the opposite effect of histamine b. Mast cell stabilizers – these are the cromalins (word was inaudible) and we will talk about these with the treatment of asthma; they stabilize mast cells so they don’t release histamines; these are a different class of drugs i. runners will often use this because when they go running in the cold; they will have an allergic of asthmatic type response, but if they use the mast cell stabilizers before they go run it will stabilize the mast cells so they never release histamine (note the different mechanism of action) c. There are 1st and 2nd generation histamine receptor antagonists i. the 1st generation anti-histamines were things like Benadryl (diphenhydramine and diphenhydrinate), and these drugs were taken orally for the relief of runny noses 1. the biggest thing about these is that they did penetrate the CNS and so they would get into the brain and bind to other receptors in addition to the histamine receptor like the serotonin receptor or the adrenergic or cholinergic receptor; and so they had side effects like drowsiness ii. 1st thing that you think of when kids take diphenhydramine and diphenhydrinate is drowsiness; if you take a motion sickness drug it will get into the brain and interact with other receptors and dry out your nose but it will also make you drowsy; a few people had the opposite effect and they got wired from taking these drugs iii. These are all reversible competitive antagonist of H1 receptors; because they are reversible they have a relatively predictable ½ life anywhere from 1 hour to 8 hours and the ones that last longer you take less frequently during the day; most of the more commonly used ones you have to take more than once a day iv. In summary, we call this 1st generation because of the side effects that were produced; with the 2nd generation, these didn’t cross the CNS so they didn’t have the side effects XIV. Histamine H1 Receptor [S15] – **he said we did not have to know numbers of weights and stuff** a. Be able to know and recognize the fact that the H1 receptor mechanism is to increase phospholipase C which means you are going to affect Ca++ movement into a cell; it’s got one mechanism of action b. These are found in the smooth muscle, intestine, blood vessels, bladder, trachea, heart, adrenal gland, vascular endothelium, CNS (all over the place) i. it is thought that histamine plays a normal role and a lot of different functions in a lot of places all over our body including digestion, and blood pressure control, and so on c. This H1 receptor (he used the example of the one in your nose) involves Ca++ entering causing smooth muscle cells to constrict or relax depending on what part of the body they are in and so it’s effect is mostly at the level of smooth muscle cells d. It should make sense to you that we have 2 different receptor classes so it should not be surprising that we can get a drug that binds to the H2 receptor that doesn’t bind to the H1; or vice versa; we are talking about apples and oranges XV. Histamine H2 Receptor [S16] – a. This is a whole different protein compared to H1; b. This activates adenyl cyclase which raises the levels of cAMP; cAMP phosphorylates the proton pump and pushes acid out c. This one is more localized and the big player is the stomach but it can also be found some in the heart, uterus, and the CNS d. You might wonder why these 2 have completely different receptor classes (H1 and H2) … XVI. H1 Receptor Antagonists [S17] – a. This is not in your power point; there is a list of 19 drugs for this category in your text; a few of them are used a lot and most of the others, you just need to know that they exist; for test purposes he would only pick the prototypical H1 antagonists for us to recognize and to know that they are H1 as opposed to H2; there are only 3 2nd generation H1’s and those you should recognize as being 2 nd generation; don’t memorize the long list in your book, but be able to recognize the 2nd generation ones because you could see this on your test; he repeated that we should for sure memorize the 2nd generation ones b. They commonly cause sedation, blurry vision, nervousness, dryness of the mouth, urinary retention, and some of these effects are because they bind to other receptors like cholinergic receptors FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 4 of 6 c. There are paradoxal effects in some children where they become awake and they become very awake instead of sleepy; they can be used to prevent motion sickness and nausea and vomiting; again, it’s because these enter the CNS, it’s because they bind to other receptors it’s why they have these effects; they are built as H1 receptor antagonists but actually they’re some of them are more effective for treating motion sickness or nausea because they bind to other receptors in the brain d. 2nd generation H1 receptor antagonists won’t affect motion sickness anymore because they don’t get into the CNS e. This is the good news and bad news about drugs entering the brain; sometimes it does what we desire and sometimes it goes off and does things we don’t desire XVII. 2nd Generation Antihistamines [S18] – a. They are rapidly absorbed b. Long duration of action; either once a day or twice a day c. Poor distribution to the CNS d. Little to no sedation e. They are not metabolized by Cytochrome P450 so you avoid all that drug/drug interaction that some of the other drugs cause f. Can be combined with pseudoephedrine in some products; you have a double whammy in terms of affect on a runny nose XVIII. 2nd Generation Antihistamine Type 1 blocking drug [S19] – you should be able to recognize these 3 drugs for the exam; these don’t cause sedation, drowsiness, they are not effective for motion sickness or nausea a. Cetirizine (Zyrtec) – can get by with 1 a day and be effective; came along later so it was approved for ages 6 and up; age 6 and up are FDA approved b. Loratadine (Claritin) – can get by with 1 a day and be effective; came along later so it was approved for ages 6 and up; age 6 and up are FDA approved c. Fexofenadine (Allegra) – not seen as often; is less potent, but can be just as efficacious and that’s a big point; you have to take it twice a day, 60mg 2 times a day so 120mg a day; this was only originally approved for age 12 and up i. Remember from earlier that we are not so much interested in potency, it’s efficacy that’s important. d. There was a question that was inaudible but it was regarding the potency vs. the efficacy of these drugs. XIX. Ocular Topical Antihistamines [S20] – a. You can give these drugs topically; when you do this you avoid the systemic effects, you minimize the concentration of the drug then that would enter the CNS; if you are trying to promote a local effect of an antihistamine you can use one of these chemicals XX. Allergic Conjunctivitis [S21] – a. There is redness here; one of the contributors to this can be histamine and so treatment with a mast cell stabilizer or an anti-histamine could be used to treat this situation b. Mast cell stabilizers are the cromalins ?(word inaudible); he won’t define those for us today but they will be in the asthma lecture XXI. Nasal Topical Antihistamines [S22] – a. You can prescribe these for a runny nose b. These are just derivatives of antihistamines that can be used in a nice water soluble form taken in a nasal spray to get the local effects on the nose as opposed to the systemic effects XXII. Review a. [S23] Which of the following drugs is least likely to cause sedation? i. [S24] Answer: Cetirizine; this is the 2nd generation antihistamine b. [S25] Which of the following mediators are immediately released after IgE is cross-linked by allergens? i. [S26] Answer: Histamine; they are all released immediately so this question should probably be reworded, but the one that is released IMMEDIATELY within milliseconds and has an immediate effect is histamine; the other mediators are released with histamine but their effects take a little longer to present; histamine is the component of the mast cells that is present in the largest quantities c. [S27] Which of the following is not a systemic effect of histamine? i. [S28] Constriction of small blood vessels FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 5 of 6 XXIII. Leukotrienes (Intro) [S29] – XXIV. Mediators of inflammation [S30] – a. You’ve seen this slide before: phospholipids are found in the cell membrane; we release phospholipids using phospholipase to form Arachadonic acid; once this gets into the cytoplasm of your cells you have enzymes that can break it into Leukotrienes and you have enzymes that can break it into prostacyclins, prostaglandins, and thromboxane i. If you give a glucocorticoid you block the process where the arrow shows on the diagram ii. If you are given Prednisone which is an effective glucocorticoid anti-inflammatory drug you would prevent the formation of everything iii. If you are given aspirin you prevent the formation of another group of things on the diagram iv. If you are given a lipoxygenase inhibitor it would inhibit Leukotriene formation but not all of the other stuff v. If you are given an inhibitor of Leukotriene binding to its receptor you would block the effect of Leukotrienes by having an inhibitor for the receptor binding for this chemical XXV. Leukotrienes in Asthma [31] – a. Leukotriene C4 (LTC4) is made in pretty large amounts by a mast cells i. causes Bronchospasm and adema ii. if you are a person who has asthma these are 2 things that you don’t want; if you are having trouble breathing a Bronchospasm and fluid leaking into your lungs are very bad things to have happen to you; so you don’t want the effects of LTC4 in your body if you have asthma b. For people without asthma, this is a normal component for breathing; we respond every minute of every day they way our lungs are working, and Leukotrienes are a part of that c. So a drug that can block Leukotrienes can be used in asthma where you get excessive production of LTC4 d. Bottom line is that Leukotriene antagonists can be used for the relief of asthma symptoms XXVI. Picture [S32] – a. In this cartoon they are looking at nuclear membranes which is full of phospholipids which are the site of phospholipase action and the release of Arachadonic acid into the cell, which is the precursor to forming Leukotrienes and prostaglandins in our cells; all our cells can make this stuff, but they have to have a storage depot of phospholipids to get the Arachadonic acid from; our cell membranes is where that storage is; the phospholipase is the enzyme that pulls out the Arachadonic acid out and puts it in the cytoplasm b. In the cytoplasm we have an enzyme called lipoxygenase which is there all the time; apparently there is some type of activating protein that has to be turned on c. The control of this system is probably how effective our phospholipase A is and how much of the lipoxygenase activating protein we have d. Most of the time we are making a modest amount of Arachadonic acid, making Leukotriene A4 and it gets converted to the other Leukotrienes and we keep it under controlled e. People who have allergic problems or asthma, this isn’t regulated right; the underlying molecular problem that is associated with asthma may have something to do with this enzyme or this protein f. The 2 red boxes on this picture are where we use drugs to intervene in the pathway; the normal pathway would be Leukotriene A4 getting converted to C4 and then B4; they then go out of the cell and get released when the cell is activated g. Why would we go to all the trouble of making a B4, C4, D4, and an E4; if we have the nice molecule A4 why would we want to change it to these others … answer: specificity; you want to have these go to different cells and have different functions and the way to do that is to make each chemical a little different i. In this cartoon B4 goes to a cell that causes chemotaxis (cells come to site of injury) whereas C4 goes to an airway smooth muscle cell and cause constriction, or it might go to an eosinophil or it might cause edema at a particular location h. To make all these different things happen we convert the Leukotriene A4 to C4, E4, D4, and B4 and all these molecules find receptors, this molecule up here binds to a B Leukotriene receptor and this molecule down here bind to a different receptor; and in this particular cartoon FUN2: 11:00-12:00 Scribe: Brittney Wise Monday, December 8, 2008 Proof: Joan-Marie Manolakis Dr. Pillion Antihistamines Page 6 of 6 all 3 of these Leukotrienes binding to this one particular receptor i. Montelukast, Pranlukast, and Zafirlukast are competitive binding inhibitors for Leukotrienes binding to their receptors at their target cell; so the ones that end in “lukast” are all competitive binding inhibitors j. Zileuton is an inhibitor of 5-Lipoxygense which is the enzyme makes the Leukotrienes in the 1st place k. What’s the difference between these 2 red boxes of drugs? i. Zileuton blocks more Leukotrienes because you block B4 and all the other Leukotrienes before they are made so you block more of the inflammatory response; these 3 Montelukast, Pranlukast, and Zafirlukast will only block specific Leukotrienes to their receptors, so it is not as effective as Zileuton l. So, note, we have 2 different mechanisms of action; this might be a little chemical that is a orally effective little guy that looks like an Arachadonic acid (not very big) so it might bind to the enzyme that is converting the Arachadonic acid to the Leukotriene; these molecules will block the Leukotrienes to their receptors, so they probably have a shape that mimics the part of the Leukotriene that binds to its receptor; the point is, that the chemistry of these things is designed to block binding to the protein and the other is to interfere with the active site of that enzyme asthmatic effect these drugs will not be effect XXVII. Actions of LTC4 (LTD4, LTE4) [S33] – a. Leukotriene are involves in the late onset of action; they cause bronchoconstriction, vascular permeability, and arterial constriction b. This is 3 or 4 hours after the initial event occurs c. For an acute asthmatic attack, if you can’t breathe right then because you have bronchial constriction, will these drugs be effective? Answer: No … you want to take these drugs to prevent this attack from happening XXVIII. Leukotriene Antagonists [S34] – a. Zileuton is the only one that you need to know; it’s an inhibitor; this will be a test question; the question will be is Zileuton (or Montelukast, Pranlukast, and Zafirlukast) an inhibitor of the enzyme or a blocker of the receptor binding b. There are more and more reports of liver disease and hypersensitivity and drug/drug interaction, a big one being if you take Warfarin and it interferes with that or it competitively binds to proteins, so you end up with increased clotting XXIX. Leukotriene Antagonists [S35] – a. Accolate; you have 20 mg 2x a day and it is a receptor antagonist and it can cause interactions with Warfarin and occasionally with liver disease XXX. Leukotriene Antagonists [S36] – a. Singulair: 5-10mg once a day; it’s also a receptor antagonist b. Cardinal one that’s out there once a day because it’s taken once a day XXXI. Review a. [S37] Which of the following drugs inhibits 5-lipoxygenase? i. Answer: Zileuton b. [S38] Which of the following drugs inhibits Leukotriene binding to its receptor? i. Answer: Montelukast, Zafirlukast, and Pranlukast XXXII. [end 36:55 min]