Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
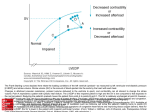
MP 2.02.16 Non-Invasive Measurement of Left Ventricular End Diastolic Pressure (LVEDP) in the Outpatient Setting Medical Policy Section Medicine Original Policy Date 12:2013 Issue 12:2013 Last Review Status/Date Reviewed with literature search/12:2013 Return to Medical Policy Index Disclaimer Our medical policies are designed for informational purposes only and are not an authorization, or an explanation of benefits, or a contract. Receipt of benefits is subject to satisfaction of all terms and conditions of the coverage. Medical technology is constantly changing, and we reserve the right to review and update our policies periodically. Description Left ventricular end diastolic pressure(LVEDP) is elevated in the setting of congestive heart failure, and its measurement may be useful in the management of patients with heart failure. However, to date, measurement of LVEDP has only been performed in the inpatient setting, since its measurement requires cardiac catheterization, either by direct measurement by placing a catheter in the left ventricle or indirect measurement by placing a catheter in the pulmonary artery to measure the pulmonary capillary wedge pressure. Noninvasive measurements of LVEDP have been developed based on the observation that the arterial pressure during the strain phase of the Valsalva maneuver may directly reflect the LVEDP. For example, arterial pressure response during the Valsalva maneuver generally shows 4 distinct phases, which can be recorded and analyzed. The VeriCor device (CVP Diagnostics, Boston, MA) is an example of a device for the noninvasive measurement of LVEDP that has received U.S. Food and Drug Administration (FDA) clearance through the 510(k) process with the following labeled indication: “The VeriCor is indicated for use in estimating non-invasively, left ventricular end-diastolic (LVEDP) pressure. This estimate, when used along with clinical signs and symptoms and other patient test results, including weights on a daily basis, can aid the clinician in the selection of further diagnostic tests in the process of reaching a diagnosis and formulating a therapeutic plan when abnormalities of intravascular volume are suspected. The device has been clinically validated in males only. Use of the device in females has not been investigated.” The VeriCor device consists of a digital expiratory manometer coupled with a continuous arterial pressure monitor and a medical grade computer. A tonometric sensor is attached to the patient’s wrist with a blood pressure cuff attached to the arm. After an 8-minute tonometric calibration period is completed, the VeriCor system is ready for use. For the test, the patient is prompted to perform a Valsalva maneuver by blowing into the mouthpiece of the digital monometer to produce an expiratory pressure of 20 to 30 mmHg for a minimum of 8 seconds. 42 Memorial Drive Suite 1 Pinehurst, N.C. 28374 Phone (910) 715-8100 Fax (910) 715-8101 FirstCarolinaCare Insurance Company, Inc. is a wholly-owned subsidiary of The digital signals are collected and stored on a medical grade computer. The arterial pressure signals are then analyzed according to algorithms that were developed to most accurately predict pulmonary capillary wedge pressure. The FDA labeling also notes that the Valsalva maneuver may be contraindicated in a variety of cardiovascular conditions, including, for example, hypertrophic obstructive cardiomyopathy, significant aortic valvular disease, and recent myocardial infarction. Policy Noninvasive measurement of left ventricular end diastolic pressure (LVEDP) in the outpatient setting is considered investigational. Policy Guidelines In 2005, a new category III CPT code is available that explicitly identifies noninvasive measurement of LVEDP: 0086T: Left ventricular fill pressure indirect measurement by computerized calibration by the arterial waveform response to Valsalva maneuver. Rationale Evaluation of a diagnostic technology typically consists of 3 steps: 1) evaluation of the technical performance of the test; 2) determination of the correlation of the technology to the gold standard of testing (i.e., noninvasive measurement of LVEDP to the gold standard of direct measurement of LVEDP with left heart catheterization or to pulmonary capillary wedge pressure), and 3) evaluation of the impact on the clinical management of the patient and a determination of whether the changes in clinical management based on the test result in an improvement in overall health outcomes. The ability to perform measurements of LVEDP noninvasively permits the outpatient use of this technology and potentially broadens the patient selection criteria for LVEDP measurement. For example, using conventional techniques, measurement of LVEDP was only performed in hospitalized patients whose symptoms were serious or unstable enough to warrant cardiac catheterization. The noninvasive measurement of LVEDP permits its use in non-acute settings, such as in the outpatient clinic as part of the ongoing management of stable patients. The manufacturer suggests that the device may be used to determine the need for hospitalization, or to monitor patients with heart failure to maintain LVEDP within a targeted range to prevent future hospitalizations. Technical Feasibility Measurement of the arterial wave form is an accepted and technically feasible technology. Diagnostic Performance Studies have shown a high correlation between invasive and non-invasive measurement of LVEDP. For example, McIntyre and colleagues reported that the 2 techniques were highly correlated in both stable and unstable and catheterized patients (R= 0.80-0.85). (1) More recently, Sharma and colleagues performed simultaneous measurements of the LVEDP based 42 Memorial Drive Suite 1 Pinehurst, N.C. 28374 Phone (910) 715-8100 Fax (910) 715-8101 FirstCarolinaCare Insurance Company, Inc. is a wholly-owned subsidiary of on 3 techniques: direct measurement of LVEDP, considered the gold standard, indirect measurement using pulmonary capillary wedge pressure (PCWP), and non-invasively using the VeriCor device in 49 patients scheduled for elective cardiac catheterization. The VeriCor measurements correlated well with the direct measures of LVEDP (r=0.86) and outperformed the PCWP, which had a correlation coefficient of 0.81 compared to the gold standard. Impact on Clinical Management A literature search did not identify any published articles that evaluated the role of noninvasive measurement of the LVEDP on the management of the patient. Therefore, data are inadequate to permit scientific conclusions regarding the clinical utility of this technology. For example, no studies examined whether including routine measurement of LVEDP in the outpatient setting resulted in improved management of congestive heart failure, as evidenced by improvement in the clinical signs and symptoms or the need for hospitalization. 2005 Update A literature search of the MEDLINE database was performed for the period of 2004 through June 2005. No additional published studies were identified that would prompt reconsideration of the policy statement, which remains unchanged. 2006 update A literature search of the MEDLINE database was performed for the period from March 2005 to November 2006. No new information regarding the clinical utility of outpatient monitoring of left ventricular end diastolic pressure was identified. The policy statement remains unchanged. 2007 Update A literature search was conducted using MEDLINE in October 2007. While research continues into the diagnostic performance of these devices, no studies were identified that reported on the impact of these measurements on clinical management and patient outcomes. Thus the policy statement is unchanged. References: 1. McIntyre KM, Parisi AF, Brown R et al. Validation and clinical applications of a noninvasive Valsalva response recorder. J Appl Cardiol 1987; 2:137-69. 2. Sharma GV, Woods PA, Lambrew CT et al. Evaluation of a noninvasive system for determining left ventricular filling pressure. Arch Int Med 2002; 162(18):2084-8. Codes Number CPT 0086T ICD-9 Diagnosis 428.0 – 428.9 Description Left ventricular fill pressure indirect measurement by computerized calibration by the arterial waveform response to Valsalva maneuver Heart failure code range Index 42 Memorial Drive Suite 1 Pinehurst, N.C. 28374 Phone (910) 715-8100 Fax (910) 715-8101 FirstCarolinaCare Insurance Company, Inc. is a wholly-owned subsidiary of Congestive Heart Failure, Left Ventricular End Diastolic Pressure, Noninvasive Measurement Left Ventricular End Diastolic Pressure, Noninvasive Measurement LVEDP, Noninvasive Measurement, VeriCor VeriCor, Left Ventricular End Diastolic Pressure 42 Memorial Drive Suite 1 Pinehurst, N.C. 28374 Phone (910) 715-8100 Fax (910) 715-8101 FirstCarolinaCare Insurance Company, Inc. is a wholly-owned subsidiary of