Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
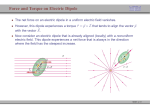
Clin. Cardiol. 15,752-758 (1992) Single Moving Dipole Obtained from Magnetic Field of the Heart in Patients with Left Ventricular Hypertrophy MASAHIRO NOMURA, M.D., m I K O NAKAYASU,* YUTAKA NAKAYA, M.D., KENSAITO,M.D., SHIGENOBU BANDO,M.D., SUSUMUITO,M.D. YUKIKO MIYOSHI, M.D., TETSUZO WAKATSUKI, M.D., The Second Department of Internal Medicine, School of Medicine;* Faculty of Integrated Arts and Science, The University of Tokushima, Tokushima, Japan Summary: Magnetocardiograms (MCGs) were recorded by means of a second-derivative SQUID (superconducting quantum interference device) magnetometer in 20 normal subjects and 28 patients with left ventricular overload to analyze the activation sequence of the heart and amplitude of estimated current source. In the normal subjects, the dipole was directed to the left and gradually superiorly 40 ms after the beginning of the QRS wave mainly due to the activation of the left ventricle. In the patients with hypertension, the direction and location of the dipoles were similar to those of the normal subjects, but their dipole moments were increased. In the patients with mitral regurgitation, the dipoles of late QRS were directed more inferiorly than in the normal subjects and their amplitude was increased. In the patients with aortic valve disease, the amplitude of the dipoles was increased markedly and their location was deviated more to the left than the dipoles of the normal subjects. We established the criterion for diagnosis of LVO from the dipole moment of 50 ms of 3.13X 10-3A or more. The sensitivity of this criterion is significantly higher in the diagnosis of left ventricular overload than the electrocardiogram (ECG). The present study shows that the moving dipole method is useful to determine the increased electromotiveforce in patients with left ventricular overload and that sensitivity in diagnosis of left ventricular overload is increased. Address for reprints: Masahiro Nomura, M.D. The Second Department of Internal Medicine School of Medicine The University of Tokushima 2-50, Kuramoto-cho Tokushima, Japan 770 Received February 13,1992 Accepted with revision: June 26,1992 Key words: magnetocardiogram,left ventricular overload, single moving dipole Introduction Detection of the increased electromotiveforce is essential in the diagnosis of left ventricular hypertrophy. However, the amplitude of electrical potential recorded from body surface is influenced by many factors, such as distance from the current source to the electrode and electrical conductivities of the intervening tissue, which makes it difficult to estimate increased electromotive force in each individual by conventionalelectrocardiogram(ECG).' The various voltage criteria are used to diagnose left ventricular overload2but their sensitivities and specificities are not satisfactory. In the present study, we developed for the first time single moving dipole methods from a magnetic field map to estimate the amplitude of the electromotive force and applied them to the diagnosis of left ventricular hypertrophy. One purpose of the electrocardiographic study is to localize the current dipole by the cardiac activities at a certain instant during the heart cycle. Development of the computer made it possible for us to determine the equivalent current dipole from body surface isopotential mapping? However, there have been few studies on the magnetocardiogram (MCG) because of recording difficulties. Recently, MCG has been considered to be a useful method to localize the cardiac source, and this method has been used for the study of the activation wave front, determination of the site of Kent and the origin of ventricular arrh~thmia.~-~ In the present study, we used the MCG to deduce the single equivalent current dipole of the heart at various cardiac cycles to analyze the activation sequence of the heart and the amplitude of estimated current source in patients with left ventricular hypertrophy. The results indicated that the increased electromotive forces can be detected more specifically by the moving dipole method than by ECG. M. Nomura et al.: Single moving dipole of MCG 753 TABLE I Subjects Number of subjects and sex (M, F) Normal 19 (13,6) EH 15 (4,ll) ASR 8 (33 4 (22) MR a Age LVDd LVWTh 55.3 f 9.2 59.1 f 7.6 51.0 f 7.6 48.3 f 11.7 46.8 f 4.3 47.5 f 2.9 54.0 f 10.5 55.3 f 8.7 9.3 rt: 1.0 9.8 f 206 12.0 f 2.3" 11.1 f 1.3 pc0.05. p<O.O1 from the control group. Abbreviations: EH =essential hypertension; ASR = aortic stenosis andor regurgitation; MR = mitral regurgitation; LVDd = left ventricular diastolic diameter: LVWTh = left ventricular wall thickness. Methods Subjects (Table I) The study included 20 normal subjects (control group) and 28 patients with left ventricular overload (LVO group). The control group consisted of 13 males and 6 females with a mean age of 55.3 f 9.2 years. They had no history of cardiac disorder, no physical abnormalities, a systolic blood pressure of < 140 mmHg, a diastolic pressure of c 90 mmHg at resting state, normal standard ECG findings, a normal chest x-ray, and normal urinalysis. The LVO group consisted of 9 men and 18 women with a mean age of 52.8 k7.2 years. This LVO group was subdivided into three subgroups based on the underlying disease: 16 patients with essential hypertension (EH), 8 patients with aortic stenosis andor regurgitation (ASR), and 4 patients with mitral regurgitation (MR). Table I lists the subjects and their echocardiographic findings. M-mode echocardiograms were recorded with a Polaroid camera using a 2.5 mHz transducer connected to an Aloka SSD-870 apparatus. The left ventricular diastolic diameter (LVDd) was measured at the peak of the R wave of the simultaneously recorded ECG, and left ventricular wall thickness (LVWTh) just before the time of atrial systole. In the ASR group, both left ventricular posterior wall thickness and end-diastolic dimension are significantly increased. In the MR group, left ventricular wall thickness was not increased but the dimension was increased significantly. In the EH group, the mean value of these indices was not increased significantly, suggesting that the left ventricular overload in this group is mild. 4, 5 , and 6 from right to left. Each grid was 2.5 cm X 2.5 cm and covered the left anterior chest wall. The subjects were kept in supine position on a wooden bed, and all metal objects such as watches, trousers with metal fasteners, contents of pockets, and hair pins were removed. The detector was positioned vertically, almost touching the anterior chest wall, and the magnetic components at each lead point were recorded with a lead I1 ECG and stored into a personal computer (NEC PC9801 UX2) via AD converter (Date1 HZ12BGC). The isofield map at each instance of the cardiac cycle was constructed every 2 ms from the beginning of the QRS waves of the lead I1 ECG with isofield interval of 1 pTesla by the methodof Nakay et al. lo Single Moving Dipole Analysis The position and strength of current dipole (dipole moments) of the heart were calculated using the methods of Williamson and Kaufmann.11J2 The position of the current dipole is under the midpoint between source and sink. 1 2 3 4 5 6 A MCG Recordings Right The MCG was recorded with a second-derivative SQUID gradiometer (BTi model BMP). Figure 1 shows the 36 recording points on the anterior chest wall with the xyphoid process as reference (E-2) to determine the 36 lead points by 6 X 6 grid system. The points were labeled in order A, B, C, D, E, and F from head to foot, and 1,2,3, C D FIG.1 Recording points of MCG. cr% Xyphoid process Clin. Cardiol. Vol. 15, October 1992 754 The depth (d) below the detecting coil and dipole moment are defined as follows: 20 ms 50 ms 70 ms d = D/21n,Q = 4 IC d2Bd0.385 po where D and Bm are the span between extrema and maximum field, respectively. The direction of the moving dipole is defined accordingto the Biot-Savartlaw. In the present study, each single moving dipole deduced from the isofieldmap at 1&8Oms was indicated as 1-8, respectively, in the isofield map. ReSUltS Isolleld Map Figure 2 shows the isofield maps of a normal subject (Fig. 2A)and patients with hypertension (Fig. 2B), aortic valve disease (Fig. 2C), and mitral regurgitation(Fig. 2D) at 20,50, and 70 ms. In each subject, at 50 ms, the positive area was located in the right lower portion and the negative area in the left superior portion, suggesting dipole movement to the left and inferiorly according to the Biot-Savart law. However, the amplitude of the maximum and minimum were increased in the LVO subgroups. Singie Moving Dipole In the normal subject, two negative areas were observed from 50 ms, suggestingthe presence of two dipoles. On the right, an upward dipole, reflecting the activation of the right ventricular outflow tract, was deduced and, on the left, a downward dipole was deduced. We analyzed only the dipole located in the left precordium to compare the electromotive force in the left ventricle in normal subjects FIG. 2 Isofield maps of a normal subject (panel A: 45-year-old male), patient with hypertension (panel B: 45-year-old male), aortic valve disease (panel C: 47-year-old female), and mitral regurgitation (panel D: 37-year-old female) at 20,50, and 70 ms. and patients with left ventricular overload. Figure 3 shows the single moving dipoles of each group. In the normal subject (Fig. 3A),at the beginning of the QRS wave, the current dipole was directed to the right and inferiorly due to the activation from left to right ventricle in the intraventricular septum. From 40ms, the dipole was directed to the left and gradually superiorly mainly due to the activation of the left ventricle.The rotation of the moving dipole was counterclockwise. FIG. 3 Isofield maps and single moving dipoles of a normal subject (panel A 63-year-old male), patient with hypertension (panel B: 62-year-old female), mitral regurgitation(panel C: 37-year-old female), and aortic valve disease (panel D: 47-year-old female). 1,2, * -,7 , 8 correspond to the moving dipole at 10,20, * a, 70,80 ms. 0 M. Nomura et al.: Single moving dipole of MCG 755 the minimum was significantly deviated inferiorly in the MR group, and was deviated superiorly in the EH group. Figure 4B shows the location of the maximum and minimum according to the severity of the overload. The LVO group is subdivided into two subgroups according to the echocardiographicfindings. One subgroup (advanced LVO group) comprises the patients whose LVDd or LVWTh are more than 50 or 11 mm, respectively. The other subgroup (mild LVO group) comprises the patients whose LVDd and LVWTh are less than 50 and 11 mm, respectively. The location of the maximum in the advanced LVO group was deviated more inferiorly and leftward and the minimum more superiorly than in the mild LVO group. Assuming the electric current source is a single dipole, the location of the current dipole is determined by positions of the maximum and the minimum in the isofield maps (single dipole method). The source of the current dipole of the advanced LVO group was deeper than that of the mild LVO group. FIG.4 Location of the maximum and minimum of the isofield map. (A) - = max SD; .... = min SD; 0= normal; = ASR; 0 = EH; A=MR. (B) -= max SD; ....= min SD; 0= normal; 0 =LVDd < 50 mm and LVWTh c 11 mm; I(,=LVDd2 50 mm or LVWTh2 11 mm. In the patient with hypertension (Fig. 3B), the direction and location of the dipoles were similar to those of the normal subject, but their dipole moments were increased. From 50 ms, the depth of the moving dipole was more shallow than that of the normal subjects. In the patients with mitral regurgitation (Fig. 3C), the dipoles of the late QRS were directed more inferiorly than in those of the normal subject, and their amplitudes were increased. In the patient with aortic valve disease (Fig. 3D), the amplitude of the dipoles was increased markedly and their location was deviated more to the left than those of the normal subject. Each moving dipole of this patient was located in a smaller region than that of the normal group. Amplitude and Dipole Moment Table 11 shows the dipole moment in each group. The EH group showed the significantly larger dipole moment only at 50 ms. In the MR group, dipole moments at 10 ms and the latter half of QRS (5CL70 ms) were significantly larger than those of the control group. In the ASR group, dipole moments from 40 to 70 ms were significantly larger than those of the control group. At 80 ms, there was no significant difference in dipole moments between the control group and LVO subgroups. MCG Criteria for Diagnosis of LVO Location of the Extrema of the Isofield Map Figure 5 shows the time from the beginning of the QRS wave to its peak amplitude (peak time) in each subject. In the ASR group this time was significantly increased compared with that of the control group. Table III shows the values of the maximum and minimum in the isofield map and amplitudes of the equivalent current dipole at 50 ms in each subgroup. There were significant differences in am- Figure 4A shows the location of the maximum and minimum in the isofield map of the control, EH, MR, and ASR groups. The location of the maximum was significantlydeviated to the left and inferiorly in the ASR and EH groups, and was deviated to the left and superiorly in the MR group, compared with the control group. The position of I1 Dipole moments in each group TABLE Am ~~~~~ 10 ms 20 ms Normal 42.4f29.8 101.4f91.3 EH MR ASR a 40 ms ~ 50 ms 182.1 f 108.3 185.9f90.0 165.5f73.8 45.3f30.8 74.7f41.6 137.6f76.1 224.5f125.1 262.3f163.9" 139.3 f 83.1" 186.2 f 120.2 233.7 f 78.2 271.9 f 152.8 438.0 f 123.3" 56.9 f 39.3 151.4 f 107.7 249.4 f 138.3 353.3 f 166.6" 534.3 f 352.v pe0.005. peo.01. peo.001. Abbreviations as in Table I. b 30 ms 60 ms 153.4f 129.8 209.3f176.1 369.5 f 72.6' 530.4 f 353.7b 70 ms 80 ms 107.6f56.0 57.9f22.7 190.8f156.1 79.2f50.6 315.7 f 158.1" 353.0 f 219.3b 115.9 f 112.3 Clin. Cardiol. Vol. 15, October 1992 756 TABLE I11 Values of the maximum and minimum in the isofield map and dipole moments Dipole moment Max (PTeslal Normal EH ASR MR 17.7 f 6.6 15.4 f 7.1 30.2 f 1.9b 19.8 f 7.1 Min (DTesla) 11.0 f 5.0 11.2 f 7.0 20.3 f 6.6" 14.1 f 3.6 Am) 165.5 f 78.8 262.3 f 163.9" 534.3 f 352.0" 438.0 f 123.3b ~~ pc0.05. p<O.O1 from the control group, Abbreviations as in Table I. a b FIG.5 Peak time in each group. In the ASR group, the peak amplitude of the QRS wave (peak time) is significantly increased (* = p < 0.05) compared with that of the control group. plitude of minimum and maximum of the isofield map between the control and ASR groups, but none between the control group and the EH or MR groups. However, the dipole moments at 50 ms were significantly increased in each subgroup of LVO. Based on these results, we established the criterion for diagnosis of left ventricular overload from the MCG as dipole moment of 50 ms of 3.13X lOW3A(mean + 2 SD of the normal control) or more. Table IV shows the diagnostic sensitivity and specificity of criteria of the ECG (SVi + SV5> 35 mV), amplitude of the minimum or maximum of the isofield map, and deduced dipole moment at 50 ms (dipole > 3.13X 10-3A) as based on the echocardiographic study. The specificity of the two criteria was not significantly different, but the MCG criterion showed significantly higher sensitivity in diagnosis of left ventricular overload. Discussion We first applied the single moving dipole method to diagnose the left ventricular overload. The present study shows that the single moving dipole determined by isofield map is useful to analyze the activation sequences in normals and patients with left ventricular overload and also helps to diagnose left ventricular overload more effectively than the conventional ECG or isofield map alone. The equivalent dipole is one of several mathematical models for estimating the cardiac electromotive forces from body surface potential distribution. The main advantages of the moving dipole method are to provide localization and quantification of the strength of the cardiac electromotive forces. There have been several studies on the solution of the dipole position in order to locate the site of electrical activity within the heart despite several methodological limitations such as instability of the inverse solution, inhomogeneity of the human body, and variation of individual body build. Since Wilson's concept of an equivalent double layer, electrical activity of the heart has been considered to be approximated by a fixed location dipole of variable magnitude and direction in homogeneous conducting medium. l3 This is the basic concept of vectorcardiography. However, detailed studies of the ventricular activation sequences and potential distributions on the thorax suggested that ventricular depolarization cannot be adequately represented by a single fixed location dipole. Most of the previous studies on the electrocardiographicinverse problem have been performed using the multiple expansion or moving dipole. Arthur et aZ.14 reported that the moving dipole during the QRS wave was within a small area in the region of the ventricle. In the present study, the main dipole was also IV Diagnostic sensitivity and specificity of the ECG, MCG and dipole moment at 50 ms TABLE ~~ ~ Normal ECG (SVl+RVS or RV6>35 mm) MCG (Max value > 2 SD) Dipole moment (Max > 2 SD) (n= 19) UCG (+) (n= 17) 1( 5.0) O( 0.0) 2( 10.5) 9(33.3) 5W.4 12(70.6) UCG(+):LVDd>SO mm or LVWTh > 11 mm a pc0.005. Abbreviations: ECG = electrocardiogram; MCG = magnetocardiogram. LVO-total (n = 27) 1.1" 9(52.9) 1l(40.7)a] 14(51.9) M. Nomura et al.: Single moving dipole of MCG approximately within the actual cardiac region. In normal subjects, two dipoles could be observed in most of the cases in the latter half of the QRS wave.15 In the present study, we analyzed only the dipole on the left because only one dipole could be observed in most patients with left ventricular overload.The direction of inscription of the normal QRS loop in the frontal plane was clockwise in 65% of patients.16In the present study, however, the inscription of the moving dipoles was counterclockwise not only in the LVO group but also in the control group, because only the dipole from the left ventricle could be detected. Tsunakawa et aL3 used moving dipole from isopotential map in patients with left bundle-branch block with and without myocardial infarction and found that the single dipole approximation is appropriate in patients with uncomplicatedleft bundle-branch block but not in those with myocardial infarction. However, they did not study the amplitude of the moving dipoles. As compared with the ECG, few studies on dipole analysis by MCG have been made. Hosaka et a1.17 reported on methods to display the current dipoles in various heart diseases and found that the arrow pattern was in good agreement with the previous results of experimental and simulation studies. Good correlationhas been found between the sites of accessory pathway and the origin of ventricular tachycardias recorded directly and the location deduced from MCG.49 The spatial accuracy of the MCG technique is in the range of 3 mm-5 cm.18 Fenici er aL6 reported that the location of the accessory pathway in Wolff-ParkinsowWhitesyndrome deduced by MCG was in good agreement with operation and electrophysiologicalfindings. In the present study, we used the single equivalent current dipole which is also an effective way to deduce current dipoles and activation sequence in normal and abnormal conditions. Fujino et a1.19 introduced criteria for the diagnosis of LVO by MCG and found that sensitivity and specificity were not different from those in the ECG. In the present study, the criterion of the amplitude of the MCG is as good as that of the ECG, but the corrected values by single equivalent dipole increased the sensitivitiesfor diagnosis of LVO significantly. This is due to the difference in the location of the dipole and peak time. In the LVO group, the dipole at 50 ms is located more deeply than in the control group, which reduced the amplitude of the body surface potential and magnetic field. The control group reaches the peak time earlier than the LVO group, so the amplitude becomes less in the control group at 50 ms compared with the LVH group which shows its largest values in this case. In the vectorcardiogram (VCG), the leftward forces of the QRS vector increase in aortic valve disease, while the posterior forces increase in hypertensive heart disease. We measured only the tangential current parallel to the frontal plane, so the dipole moment of the ASR group is larger than that of the HT group in the present study. In a future MCG study, we shall have to record the three-dimensional MCG with the new generation of SQUID gradiometers. 757 The single equivalent current dipole algorithm is used to localize current sources in the brain and heart. This study also shows that this method is useful to deduce the amplitude of the current sources. In the ECG, the voltage recorded at the body surface is influenced by the body shape and is reduced variously by the inhomogeneous tissues, such as lung, muscle, and fatty tissues.20The electrical conductivities of each tissue differ and the degrees of reduction vary greatly in each individual. Therefore, correct evaluation of the increased electromotive force by ECG is difficult. The current sources of the cardiac activation are not single, as suggested by the multiple activation front in the human model by Durrer et aL2' However, the single moving dipole could provide us with a rough approximation of the location of the activation front in certain instances, as well as with summation of the current dipoles at various portions of the activation front. The present study shows that the moving dipole method is useful to determine the increased electromotiveforce in patients with left ventricular overload and increases sensitivity in the diagnosis of left ventricular overload. References 1. Mori H, Nakaya Y Present status of clinical magnetocardiography. CV World Report 1,78-86 (1988) 2. Sokolow M, Lyon T P The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 37, 161-186 (1949) 3. Tsunakawa H, Nishiyama G, Kanesaka S, Harumi K Application of dipole analysis for the diagnosis of myocardial infarction in the presence of left bundle branch block. J Am Coll Cardiol 10, 1015-1021 (1987) 4. Nomura M, Nakaya Y, Watanabe K, Katayama M, Takeuchi A, Fujino K, Mori H: Detection of accessory pathway in patients with WPW syndrome by means of the isomagnetic map and MRI. In Advances in Biomagnetism (Eds. Williamson SJ, Hoke M, Stroink G, Kotani M). Plenum, New York (1989) 373-376 5. Katila T, Montonen J, Makijarvi M, Nenonen J, Raivio M, Siltanen P Localization of the accessory cardiac conduction pathway. In Biomagnetism '87 (Eds. Atsumi K, Kotani M, Ueno S, Katila T). Tokyo Denki University Press, Tokyo (1987) 274277 6. Fenici RR, Melillo G, Cappelli A, Luca CD, Masselli M: Magnetocardiographic localization of Kent bundles. In Advances in Biomagnetism (Eds. Williamson SJ, Hoke M, Stroink G, Kotani M). Plenum, New York (1989) 365-368 7. Erne SN, Trahms L, Trontelj Z: Current multipoles as sources of biomagnetic fields. In Biomagnetism '87. (Eds. Atsumi K, Kotani M, Ueno S, Katili T). Tokyo Denki University Press, Tokyo (1987) 302-305 8. Schmitz L, Oeff M, Erne SN: Localization of arrhythmogenic areas in the human heart. In Biomagnetism '87 (Eds. Atsumi K, Kotani M, Ueno S, Katila T). Tokyo Denki University Press, Tokyo (1987) 286-289 9. Fenici RR, Masseli M, Lopez L, Melillo G: Magnetocardiographic localization of the arrhythmogenic tissue. In Biomagnetism '87 (Eds. Atsumi K, Kotani M, Ueno S, Katila T). Tokyo Denki University Press, Tokyo (1987) 282-285 10. Nakaya Y, Sumi M, Saito K, Fujino K, Murakami M, Mori H: Analysis of current source of the heart using isomagnetic and vector arrow maps. Jpn Heart J 25,701-711 (1984) 758 Clin. Cardiol. Vol. 15, October 1992 11. Williamson SJ, Kaufman L Magnetic fields of the cerebral cortex. In Biomagnetism (Eds. Erne S, Hahlbohm HD, Lubbig H). Walter de Grutter, Berlin, New York (1984) 353-402 12. Romani GL, Williamson SJ, Kaufman L: Biomagnetic instrumentation. Rev Sci Instr 53, 1815-1845 (1982) 13. Wilson FN, MacLeod AG, Barker PS: The distribution of action c a n t produced by heart muscle and other excitable tissues immersed in extensive conducting medium. J Gen Physiol 16,423456 (1933) 14. Arthur RM, Geselowitz DB, Briller SA, Trost RF:The path of the electrical center of the human heart determined from surface electrocardiogram.J Electmcardiol4,29-33 (1971) 15. Nakayasu K, Nakaya Y, Ishihara S,Nomura M, Mori H: Isomagnetic maps in normal subjects. Comparison with isopotential maps. CV World Report 3,22-27 (1989) 16. Chou TC, Helm RA, Kaplan S: Left ventricular hypertrophy. In Clinical Vectorcardiography. Grune & Stratton, New York, London (1974) 71-84 17. Hosaka H, Cohen D: Visual determination of generators of the magnetocardiogram. J Electrocardiol9,426432 (1976) 18. Hart G: Biomagnetometry: Imaging the heart’s magnetic field. BrHeartJ65,61 (1991) 19. Fujino K, Sumi M, Saito K, Murakami M, Higuchi T, Nakaya Y, Mori H: Magnetocardiograms of patients with left ventricular overloading recorded with a second-derivative SQUID gradiometer. J Electrocardioll7,219-228 (1984) 20. Nakaya Y, Takeuchi A, Nii H, Ishihara S,Nomura M, Fujino K, Saito K, Mori H: Isomagnetic map in right ventricular overloading. J Electrocardiol21, 168-173 (1988) 21. Durrer D, Van Dam RT, Freud GE,Janse MJ, Meijer FL, Arzbaecher RC: Total excitation of the isolated human heart. Circulation 41,899-912 (1970)