Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Microevolution wikipedia , lookup
Medical genetics wikipedia , lookup
Public health genomics wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Cancer epigenetics wikipedia , lookup
Genome (book) wikipedia , lookup
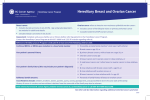
v14.1 UNMC Human Genetics Laboratory Hereditary Breast6 Cancer Panel INDICATIONS FOR TESTING DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary Breast6 Cancer Panel analyzes six genes for genetic variants that predispose a person to breast cancer and, in some cases, other cancers or noncancerous conditions. Identifying causative genetic variants in any of the genes included in this panel provides medically actionable results (treatment and/or risk reduction) and allows for targeted familial screening. Up to 10% of women affected by breast 1 cancer have an inherited genetic syndrome. The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. INCIDENCE In the general population, approximately 1 in 300 and 1 in 800 individuals have BRCA1 and BRCA2 mutations, respectively. These mutations are more frequently observed in individuals of certain ethnicities; for example, 1 in 40 individuals in the Ashkenazi Jewish population harbor a BRCA1 or BRCA2 mutation. The frequency of 1 mutations in TP53, PTEN, STK11, and CDH1 are more rare. GENES & DISORDERS INCLUDED IN THIS PANEL BRCA1 & BRCA2 TP53 PTEN STK11 CDH1 -- Hereditary breast and ovarian cancer syndrome -- Hereditary diffuse gastric cancer -- Li-Fraumeni syndrome -- PTEN hamartoma tumor (Cowden) syndrome -- Peutz-Jeghers syndrome • Known familial variant in any of the genes included in this panel (targeted analysis) INHERITANCE • • • • • • Breast cancer diagnosed ≤ age 45 • Breast cancer diagnosed ≤ age 50 and a close relative with breast cancer at any age • Breast cancer diagnosed ≤ age 50 with limited or unknown family history • Bilateral breast cancer or two separate breast primary cancers with the first ≤ age 50 • Breast cancer diagnosed ≤ age 60 with triple negative pathology • Male breast cancer diagnosed at any age • Ovarian, fallopian tube, or primary peritoneal cancer diagnosed at any age • Pancreatic cancer or aggressive prostate cancer in someone who also has a family history of breast, ovarian, pancreatic or aggressive prostate cancer • Family history of the above indications (typically when affected family members are unavailable for testing or deceased) or limited family history • Ashkenazi Jewish ancestry and breast or ovarian cancer • Personal and/or family history raising concern for the syndromes included in this panel Hereditary breast and ovarian cancer syndrome Li-Fraumeni syndrome PTEN hamartoma tumor (Cowden) syndrome Peutz-Jeghers syndrome Hereditary diffuse gastric cancer 1. National Comprehensive Cancer Network (NCCN). Genetic/Familial High-Risk Assessment: Breast and Ovarian (Version 1.2014). http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#breast_screening. April 11, 2014. METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. SPECIMEN REQUIREMENTS •3-5 ml blood in an EDTA tube (purple top) TURN-AROUND-TIME •Results are typically available in 2-3 weeks UNMC Human Genetics Laboratory 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Breast Ovarian Uterine26 Cancer Panel INDICATIONS FOR TESTING INHERITANCE • Breast cancer diagnosed ≤ age 45 • Breast cancer diagnosed ≤ age 50 and a close relative with breast cancer at any age • Breast cancer diagnosed ≤ age 50 with limited or unknown family history • Bilateral breast cancer or two separate breast primary cancers with the first ≤ age 50 • Breast cancer diagnosed ≤ age 60 with triple negative pathology • Male breast cancer diagnosed at any age • Ovarian, fallopian tube, or primary peritoneal cancer diagnosed at any age • Uterine or ovarian cancers and a family history of gastrointestinal cancers • Pancreatic cancer or aggressive prostate cancer in someone who also has a family history of breast, ovarian, pancreatic or aggressive prostate cancer • Breast, ovarian, or uterine cancer with a second primary tumor • Family history of the above indications (typically when affected family members are unavailable for testing or deceased) or limited family history • Ashkenazi Jewish ancestry and breast or ovarian cancer • Personal and/or family history raising concern for the syndromes included in this panel INCIDENCE • Known familial variant in any of the genes included in this panel (targeted analysis) DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary BreastIOvarianIUterine26 Cancer Panel analyzes 26 genes for genetic variants that predispose a person to breast, ovarian, and uterine (endometrial) cancer and, in some cases, other cancers or noncancerous conditions. Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, treatment and risk reduction options, surveillance (early screening for other associated cancers), and familial screening. The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. Breast cancer affects about 1 in 8 women, while ovarian and uterine (endometrial) cancers affect approximately 1 in 71 and 1 in 38 women, respectively.1 A detectable, inherited familial mutation is present in approximately 5-15% of women with these types of tumors.2 While BRCA1 and BRCA2 are most commonly involved, inclusion of the rarer, high-risk genes markedly increases the number of families with an identifiable genetic cause. GENES INCLUDED IN THIS PANEL -- Hereditary breast and ovarian cancer syndrome -- Hereditary diffuse gastric cancer -- Li-Fraumeni syndrome -- Lynch syndrome -- MUTYH-associated polyposis (MAP) -- PTEN hamartoma tumor (Cowden) syndrome -- Peutz-Jeghers syndrome METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. ATM CHEK2 MSH2 PMS2 TP53 SPECIMEN REQUIREMENTS BARD1 EPCAM MSH6 PTEN XRCC2 •3-5 ml blood in an EDTA tube (purple top) BRCA1 FAM175A MUT YH RAD50 BRCA2 FANCC NBN RAD51C BRIP1 MLH1 NF1 RAD51D CDH1 MRE11A PALB2 STK11 1. National Cancer Institute (NCI). Surveillance, Epidemiology, and End Results (SEER). http://seer.cancer.gov 2. National Comprehensive Cancer Network (NCCN). Genetic/Familial High-Risk Assessment: Breast and Ovarian (Version 1.2014). http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#breast_screening. April 11, 2014. TURN-AROUND-TIME •Results are typically available in 3-4 weeks UNMC Human Genetics Laboratory 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Colorectal20 Cancer Panel INDICATIONS FOR TESTING •Family history of colon, endometrial, ovarian, or stomach cancer in multiple individuals •Colorectal cancer diagnosed < age 50 •Multiple primary cancers in the same person •10 or more colon polyps •Tumor testing positive for high microsatellite instability (MSI) and/or abnormal immunohistochemistry (IHC) indicating mismatch repair deficiency • Personal and/or family history raising concern for the syndromes included in this panel DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary Colorectal20 Cancer Panel analyzes 20 genes for genetic variants that predispose a person to colorectal cancer and, in some cases, other cancers and noncancerous conditions. Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, risk reduction options, surveillance (early screening for other associated cancers), and familial screening. -- Familial adenomatous polyposis (FAP) -- Hereditary diffuse gastric cancer -- Juvenile polyposis syndrome -- Li-Fraumeni syndrome -- Lynch syndrome -- MUTYH-associated polyposis (MAP) -- Peutz-Jeghers syndrome -- PTEN hamartoma tumor (Cowden) syndrome •Known familial variant in any of the genes included in this panel (targeted analysis) INHERITANCE The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. INCIDENCE Colorectal cancer is one of the most common cancers representing 9-10% of all new cancers annually. Inherited, single gene causes are identified in 5-10% of colorectal cancers.1 GENES INCLUDED IN THIS PANEL METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. SPECIMEN REQUIREMENTS APC CHEK2 MSH2 POLE ATM EPCAM MSH6 PTEN AXIN2 GALNT12 MUT YH SMAD4 TURN-AROUND-TIME BMPR1A GREM1 PMS2 STK11 •Results are typically available in 3-4 weeks CDH1 MLH1 POLD1 TP53 1. Haggar, FA and Boushey, RP. Colorectal Cancer Epidemiology: Incidence, Mortality, Survival, and Risk Factors. Clin Colon Rectal Surg, 22:191-197, 2009. •3-5 ml blood in an EDTA tube (purple top) UNMC Human Genetics Laboratory 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Endocrine Paraganglioma-Pheochromocytoma17 Cancer Panel INDICATIONS FOR TESTING •Family history of paraganglioma, pheochromocytoma, or other neuroendocrine tumors, which may include tumors of the thyroid, parathyroid, pituitary gland, lung, pancreas, kidney, and/or gastrointestinal tract (e.g., gastrointestinal stromal tumors [GIST]) •Neuroendocrine tumor with a second primary lesion •Personal and/or family history of -- Sympathetic or malignant extra-adrenal paragangliomas -- Bilateral or multifocal paragangliomas or pheochromocytomas -- Paraganglioma or pheochromocytoma DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary EndocrineIParaganglioma-Pheochromacytoma17 Cancer Panel analyzes 17 genes for genetic variants that predispose a person to paragangliomas (PGLs), including pheochromocytomas (PCCs), and other neuroendocrine tumors. Many neuroendocrine tumors are benign, localized, and sporadic; however, they may also be part of a hereditary cancer predisposition syndrome and may increase the patient’s risk for other medical conditions, such as hypertension and stroke.1-4 Individuals with hereditary neuroendocrine tumors are more likely to present earlier, to have multifocal or bilateral disease, and to experience recurrence and metastisis.4-5 Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, medical management, malignancy potential, surveillance (early screening for other associated tumors), and familial screening. INHERITANCE The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. INCIDENCE The incidence of neuroendocrine tumors is reported to be 5.25 cases per 100,000 people and is currently thought to be rising in the United States.8 An underlying genetic cause has been identified in greater than 25% of patients with neuroendocrine tumors.1-2,4,6-7,9 GENES INCLUDED IN THIS PANEL • Personal and/or family history raising concern for the syndromes included in this panel -- Carney complex -- Familial medullary thyroid carcinoma (FMTC) -- Hereditary paraganglioma-pheochromocytoma syndrome (PGL/PCC) -- Hyperparathyroidism-jaw tumor syndrome -- Li-Fraumeni syndrome -- Multiple endocrine neoplasia (MEN2) type I and II -- Neurofibromatosis type I (NF1) -- PTEN hamartoma tumor (Cowden) syndrome -- Tuberous sclerosis complex (TSC) -- von Hippel-Lindau disease (VHL) •Known familial variant in any of the genes included in this panel (targeted analysis) METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. CDC73 NF1 RET SDHB TMEM127 TSC2 SPECIMEN REQUIREMENTS MAX PRKAR1A SDHA SDHC TP53 VHL •3-5 ml blood in an EDTA tube (purple top) MEN1 PTEN SDHAF2 SDHD TSC1 TURN-AROUND-TIME •Results are typically available in 3-4 weeks 1. Kirmani S and Young WF. “Hereditary Paraganglioma-Pheochromocytoma Syndromes.” In GeneReviewsTM, edited by Roberta A PAgon, Margaret P Adam, Thomas D Bird, Cynthia R Dolan, Chin-To Fong, and Karen Stephens. Seattle (WA): University of Washington, Seattle, 1993. http://www.ncbi.nlm.nih.gov/books 2. Fishbein, L., and Nathanson, K. Pheochromocytoma and paraganglioma: understanding the complexities of the genetic background. Cancer Genet, 205(1-2):1-11, 2012. 3. DeLellis, R., et al. World health organization classification of tumors. Pathology and Genetics of Tumours of Endocrine Organs. Lyon, France: IARC Press, 2004. 4. National Cancer Institue (NCI). Pheochromocytoma and Paraganglioma Treatment. http://www.cancer.gov/cancertopics/pdq/treatment/pheochromocytoma/HealthProfessional/ 5. Gimenez-Roqueplo AP, Lehnert H, Mannelli M, Neumann H, Opocher G, Maher ER,et al. Phaeochromocytoma, new genes and screening strategies. Clin Endocrinol (Oxf).65(6):699-705, 2006. 6. Neumann HP, Bausch B, McWhinney SR, et al.: Germ-line mutations in nonsyndromic pheochromocytoma. N Engl J Med, 346 (19): 1459-66, 2002. 7. Amar L, Bertherat J, Baudin E, et al.: Genetic testing in pheochromocytoma or functional paraganglioma. J Clin Oncol, 23 (34): 8812-8, 2005. 8. National Comprehensive Cancer Network (NCCN). Neuroendocrine Tumors. http://nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. July 15, 2014. 9. Jiménez C, Cote G, Arnold A, et al.: Review: Should patients with apparently sporadic pheochromocytomas or paragangliomas be screened for hereditary syndromes? J Clin Endocrinol Metab, 91 (8): 2851-8, 2006. UNMC Human Genetics Laboratory 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Neuro17 Cancer Panel INDICATIONS FOR TESTING •Personal and/or family history of -- Brain tumor(s) -- Central nervous system (CNS) tumor(s) -- Peripheral nervous system (PNS) tumor(s) •Brain or CNS tumor associated with multiple genetic conditions, such as ependymoma, glioblastoma, meningioma, and medulloblastoma •Personal and/or family history raising concer for the syndromes included in this panel DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary Neuro17 Cancer Panel analyzes 17 genes for genetic variants that confer an increased risk of developing a brain tumor and, in some cases, other cancers and noncancerous conditions. Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, medical management, surveillance (early screening for other associated cancers), and familial screening. -- Familial adenomatous polyposis (FAP) -- Nevoid basal cell carcinoma (Gorlin) syndrome -- Li-Fraumeni syndrome -- Lynch syndrome -- Neurofibromatosis type I and II (NF1 and NF2) -- PTEN hamartoma tumor (Cowden) syndrome -- Tuberous sclerosis complex (TSC) -- von Hippel-Lindau disease (VHL) • Known familial variant in any of the genes included in this panel (targeted analysis) INHERITANCE The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. Many of the genes on the Neuro19 Cancer Panel have high de novo rates and, therefore, family history may be negative despite a person’s genetic predisposition. The exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. INCIDENCE In the United States, approximately 24,600 individuals per year are diagnosed with a malignant brain tumor.1 Approximately 5% of patients with brain cancers have an identifiable underlying genetic cause.2 METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. SPECIMEN REQUIREMENTS GENES INCLUDED IN THIS PANEL •3-5 ml blood in an EDTA tube (purple top) ALK MLH1 NBN PHOX2B SUFU TSC2 APC MSH2 NF1 PMS2 TP53 VHL MEN1 MSH6 NF2 PTCH1 TSC1 TURN-AROUND-TIME •Results are typically available in 3-4 weeks UNMC Human Genetics Laboratory 1. American Brain Tumor Association. Brain Tumor Statistics. http://abta.org 2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin 2013;63(1):11-30, 2013. 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Pancreatic14 Cancer Panel INDICATIONS FOR TESTING •Pancreatic cancer diagnosed < age 50 •Pancreatic cancer at any age and a second primary cancer in one individual •Pancreatic cancer in multiple generations of a family • Personal and family history of pancreatic and non-pancreatic cancers (especially breast, ovarian, colon, melanoma, and uterine) • Personal and/or family history raising concern fo the syndromes included in this panel DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary Pancreatic14 Cancer Panel analyzes 14 genes for genetic variants that predispose a person to pancreatic cancer and, in some cases, other cancers and noncancerous conditions. Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, medical management, surveillance (early screening for other associated cancers), and familial screening. -- Familial adenomatous polyposis (FAP) -- Melanoma-pancreatic cancer syndrome -- Hereditary breast and ovarian cancer syndrome -- Li-Fraumeni syndrome -- Lynch syndrome -- Malignant melanoma syndrome -- Peutz-Jeghers syndrome -- von Hippel-Lindau disease (VHL) •Known familial variant in any of the genes included in this panel (targeted analysis) INHERITANCE The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. INCIDENCE Approximately 1.5% of people will develop pancreatic cancer. It is estimated that about 10% of these cases are due to an inherited familial mutation.1 GENES INCLUDED IN THIS PANEL APC CDKN2A MSH6 TP53 ATM EPCAM PALB2 VHL BRCA1 MLH1 PMS2 BRCA2 MSH2 STK11 METHODS This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. SPECIMEN REQUIREMENTS •3-5 ml blood in an EDTA tube (purple top) TURN-AROUND-TIME •Results are typically available in 3-4 weeks UNMC Human Genetics Laboratory 1. National Cancer Institute (NCI). Surveillance, Epidemiology, and End Results (SEER). http://seer.cancer.gov 402.559.5070 unmc.edu/geneticslab [email protected] v14.1 UNMC Human Genetics Laboratory Hereditary Renal19 Cancer Panel INDICATIONS FOR TESTING •Family history of renal cancer in multiple individuals •Renal cancer diagnosed < age 45 •Multifocal or bilateral renal cancer •Multiple primary cancers in the same person which may include the skin, brain, heart, lungs, pancreas, colon, paraganglioma, pheochromocytoma, or other neuroendocrine tumors •Renal cancer and other findings, such as cysts in the lung, kidneys, pancreas, adnexa or epididymis; pneumothorax; uterine fibroids; or skin findings such as cutaneous leiomyoma, fibrofolliculoma, or angiofibroma • Personal and/or family history raising concern for the syndromes included in this panel DESCRIPTION Using sequencing and high resolution deletion/duplication analysis, the Hereditary Renal19 Cancer Panel analyzes 19 genes for genetic variants that predispose a person to renal cancer and, in some cases, other cancers or noncancerous conditions. Identifying a causative genetic variant provides valuable information for the patient’s diagnosis, medical management, surveillance (early screening for other associated cancers), and familial screening. Affected individuals often warrant increased surveillance due to earlier onset of disease and have an increased potential for complex medical issues such as bilateral kidney involvement. -- Birt-Hoge-Dubé syndrome -- Hereditary leiomyomatosis and renal cell cancer -- Hereditary papillary renal carcinoma -- Hereditary paraganglioma-pheochromocytoma syndrome (PGL/PCC) -- Li-Fraumeni syndrome -- Lynch syndrome -- PTEN hamartoma tumor (Cowden) syndrome -- Tuberous sclerosis complex (TSC) -- von Hippel-Lindau disease (VHL) •Known familial variant in any of the genes included in this panel (targeted analysis) INHERITANCE The inheritance of hereditary cancer predisposition syndromes is typically autosomal dominant, meaning that all individuals who inherit the mutation will be at risk for developing cancer. However, the exact risk and cancer type is dependent on the gene and mutation involved. Additionally, the age at which an individual develops cancer and the site of cancer diagnoses may vary within a family. METHODS Approximately 65,000 individuals in the United States will develop renal cancer in 2014, and 2-4% of cases are thought to be hereditary in nature.1-3 This hereditary cancer panel utilizes next generation sequencing for the identification of sequence-based variants and a customized oligonucleotide array for the identification of deletions/duplications in the genes included in this panel. GENES INCLUDED IN THIS PANEL SPECIMEN REQUIREMENTS INCIDENCE CDC73 MET MSH6 SDHB TSC1 EPCAM MITF PMS2 SDHC TSC2 FH MLH1 PTEN SDHD VHL FLCN MSH2 SDHA TP53 •3-5 ml blood in an EDTA tube (purple top) TURN-AROUND-TIME •Results are typically available in 3-4 weeks UNMC Human Genetics Laboratory 1. Bausch B., Jilq C., Glasker S., Vortmeyer A., Lutzen N., Anton A., Eng C., and Neumann HP. Renal cancer in von Hippel-Lindau disease and related syndromes. Nat Rev Nephrol, 9(9):529-38, 2013. 2. National Cancer Institute (NCI). Surveillance, Epidemiology, and End Results (SEER). http://seer.cancer.gov 3. Chan-Smutko G. Genetic Testing by Cancer Site: Urinary Tract. The Cancer Journal, 18(4):343-349, 2012. 402.559.5070 unmc.edu/geneticslab [email protected]