Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Circular dichroism wikipedia , lookup
Protein domain wikipedia , lookup
Rosetta@home wikipedia , lookup
Homology modeling wikipedia , lookup
Protein mass spectrometry wikipedia , lookup
Implicit solvation wikipedia , lookup
Protein design wikipedia , lookup
Protein folding wikipedia , lookup
Bimolecular fluorescence complementation wikipedia , lookup
Alpha helix wikipedia , lookup
Western blot wikipedia , lookup
Nuclear magnetic resonance spectroscopy of proteins wikipedia , lookup
Protein–protein interaction wikipedia , lookup
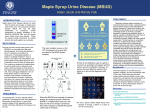
Maple Syrup Urine Disease – Clinical Management Pathway Positive Screen Clinical team notified-report before 12 noon Contact Family Instruct to go to local hospital if not inpatient Liaise with Local Hospital (may already be inpatient) Ix-Blood gas, U&E, LFTs, fbc, cultures, ketones dipstick Mx-stop feeds, IV 10% dextrose /0.45% saline + added potassium Ambulance Transfer If GCS < 8-intubate and ventilate and organise PICU retrieval Admit to Specialist IMD Centre Same day Diagnostic Tests + Consent to study Urgent Amino acids Organic acids MSUD Manage as MSUD Yes Alloisoleucine Positive? No Original NBS Card Alloisoleucine Positive? Yes ? Intermittent MSUD Send fibroblasts for enzymology Manage as MSUD until result known Maple Syrup Urine Disease nd Clinical Management Pathway V1.2 Dated 2 Oct 2012 Approved by Michael Champion No Presumptive False positive Investigate & treat Exclude liver disease including galactosaemia MSUD Management of Sick Neonate Stop breast feeding (continue expressing) and or standard formula feeds (temporarily) Consider dialysis/haemofiltration dependent on clinical condition and leucine level Promote anabolism Calories 120-140kcals/kg/day BCAA free protein MSUD Anamix infant oral or NG as tolerated, or MSUD Aid III if fluid restricted, to provide at least 3g/kg/day protein equivalent Give Isoleucine & Valine supplements, 100-200mg each, to maintain target levels (see below) If feeds poorly tolerated IV 10% dextrose + added electrolytes (+/- insulin if hyperglycaemic) + NG BCAA free formula/supplement (as tolerated) + IV Intralipid 2g/kg/day Use BCAA-free TPN if not absorbing and available Patients with decompensated MSUD are at risk of cerebral oedema Avoid hyponatraemia which may exacerbate this risk. Goals of Treatment Leucine decrease >750mol/L each 24 hours until within target range Isoleucine & Valine maintain in target range (avoid low levels which are rate limiting for protein synthesis) negative Ketones Leucine 200-400 Leucine (mol/L) > 800 Isoleucine 200-400 400-800 reintroduce 2 exchanges (100mg) Valine 200-400 200-400 reintroduce 4 exchanges (200mg) Target Levels (mol/L) Monitoring Fontanelle and head circumference BCAAs U&E Ketones (urine dip) bd daily bd bd Maple Syrup Urine Disease nd Clinical Management Pathway V1.2 Dated 2 Oct 2012 Approved by Michael Champion Guide to re-introducing protein (leucine exchanges) no natural protein MSUD Management of Asymptomatic Neonate Oral/NG feeds given as BCAA free formula (as tolerated) +/- natural protein as per guide below (given as EBM or formula feed) Promote Anabolism Calories 100-120kcals/kg/day BCAA free protein MSUD Anamix infant oral or NG as tolerated to provide at least 3g/kg/day protein equivalent and 150-180mL/kg/day Isoleucine & Valine Supplement to maintain target levels as needed Leucine Given as natural protein. 1 exchange = 50mg leucine 1 exchange = 45mL EBM 1 exchange = 35mL formula feed Goals of Treatment Target Levels (mol/L) Leucine 200-400 Isoleucine 200-400 Valine 200-400 Ketones Leucine (mol/l) > 800 Guide to re-introducing protein (leucine exchanges) no natural protein 400-800 reintroduce 2 exchanges (100mg) 200-400 reintroduce 4 exchanges (200mg) negative Monitoring Fontanelle and head circumference BCAAs Ketones daily until stable daily until stable daily until stable Maple Syrup Urine Disease nd Clinical Management Pathway V1.2 Dated 2 Oct 2012 Approved by Michael Champion MSUD Formulas & Supplements MSUD Anamix Infant (SHS) 15% dilution (1 level 5g scoop + 30ml water) Per 100g Energy (Kcal) 457 Protein (g) 13.1 CHO (g) 49.5 Fat (g) 23 Per 100ml 69 2 7.5 3.5 1 yellow scoop = 5g powder 1 large blue scoop = 26g powder MSUD AID III (SHS) 5% dilution (1 level 5g scoop + 100ml water) Per 100g Energy (Kcal) 334 Protein (g) 79 CHO (g) 4.5 Fat (g) nil Per 100ml 16.7 3.95 0.23 nil 1 yellow scoop = 5.7g powder 1 large blue scoop = 32g powder Valine Sachet Energy (Kcal) Valine (mg) CHO (g) Per 100g 384 1250 96 Per 4g sachet 15 50 3.8 Per 100g 384 1250 96 Per 4g sachet 15 50 3.8 Isoleucine Sachet Energy (Kcal) Isoleucine (mg) CHO (g) IV Dextrose % dextrose 10% 12.5% 15% 20% Energy (Kcal)/ml 0.34 0.43 0.51 0.68 Energy (Kcal)/100ml 34 43 51 68 Intralipid 10% solution (1.1Kcal/ml) 20% solution (2.0Kcal/ml) 0.8ml/kg/day 0.4ml/kg/day Maple Syrup Urine Disease nd Clinical Management Pathway V1.2 Dated 2 Oct 2012 Approved by Michael Champion = = 2g/kg/day 2g/kg/day Follow Up 1st Year Home Monitoring BCAAs weekly Urine ketones as required during intercurrent illness Weekly or fortnightly weighing until 1st outpatient appointment Outpatients 1st follow up 4-6 weeks Then 3-4 monthly for clinical and dietetic review/education Weight/length Amino acids Outcome Measures Age at diagnosis Time to leucine <400mcmol/L from notification Admissions first year Outpatient attendance (% of expected) Median leucine level for 1st year Frequency of blood tests 1st year (% of expected) Growth centiles end of year 1 Developmental Assessment at 1 year Maple Syrup Urine Disease nd Clinical Management Pathway V1.2 Dated 2 Oct 2012 Approved by Michael Champion