Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
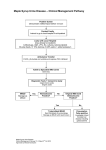
Please see this child immediately Emergency Letter: MAPLE SYRUP URINE DISEASE (MSUD) Date: RE: Name DOB: [NAME] is followed by the Metabolic Clinic at the University of Utah for Maple Syrup Urine Disease. This inborn error of metabolism confers a high risk for brain edema with severe and permanent brain damage or death if inadequately treated when the child is sick. Such risk is highest in case of fasting, dehydration, or fever, when the body is catabolic and needs to use endogenous proteins for calories. This child needs to be seen by the ER physician as soon as possible. In MSUD, chronic treatment is based on a special diet with medical formula devoid of leucine, isoleucine and valine. Treatment of acute events aims at providing substantial amounts of extra fluids and calories, using insulin as needed to induce an anabolic state and reduce blood leucine levels, and preventing hyponatremia. Parents have been instructed to bring the child to the Emergency Room if unable to eat for more than 12 hours or if the child has high fever/vomiting. Immediate Recommended Treatment in case of fever, vomiting, diarrhea, or fasting, to prevent the neurologic complications STOP protein intake, but allow special medical formula if tolerated (e.g., KETONEX 1 and 2 diluted to 24 cal/oz). Enteral feeds are the most effective, use NG tube if necessary. START immediately IV fluids (even if the child does not look dehydrated) to give extra fluids and calories: o Use D10W or D12.5W, in half-normal Saline, with 20 mEq/L KCl, infused at 1.5 to twice maintenance (after second birthday, use one quarter normal saline instead of half normal saline) o Add Intralipids 20% if available, infused at one tenth of the rate of D10W infusion MONITOR for signs of BRAIN EDEMA: can give mannitol IV (0.5 g/kg per dose) if suspected. GET the following labs: Basic Metabolic Panel, CBC with differential, Plasma Ammonia, Urine organic acids, Urine analysis (for ketones) MONITOR glucose every 3 hours: if >180 mg/dl, use insulin bolus (0.1 U/kg) as needed. Insulin is very effective at reducing plasma leucine levels. Stop insulin when glucose drops under 140. Keep glucose between 90 and 150 mg/dL. MONITOR serum Sodium every 4 hours, for risk of hyponatremia. Keep above 136 to prevent brain edema. Consider using 3% NaCl (1 ml/kg) to keep Na from dropping under 136. CALL Geneticist: please phone (801) 581-2121 and ask for the geneticist on call to be paged. Try to identify cause of decompenstion (usually infection) and start causal treatment as necessary. DISCHARGE only when afebrile, stable, well hydrated, able to eat adequately, without vomiting or diarrhea, without ketones in urine and with normal basic metabolic panel (including normal sodium) Thank you in advance, Lorenzo Botto, MD / Nicola Longo, MD PhD/Ashley Warnock MD Genetics/Pediatrics, University of Utah (801) 585-2457