Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Rheumatic fever wikipedia , lookup
Artificial heart valve wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Aortic stenosis wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
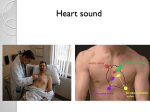
Heart/Neck Vessels & Peripheral Vascular/Lymphatics Anatomy Review 4 chambers – Right/left atrium – Right/left ventricle 4 valves – – – – Tricuspid Mitral Pulmonic Aortic Anatomy and Physiology Cardiac output (L/min) determined by: – Heart rate (beats/min) – Stroke volume (L/beat) • CO = SV x HR Measure Typical value Normal range end-diastolic 120 ml[1] volume (EDV) 65 - 240 ml[1] end-systolic 50 ml[1] volume (ESV) 16 - 143 ml[1] stroke volume 70 ml (SV) 55 - 100 ml ejection fraction (Ef) 58% 55 to 70%[2] heart rate (HR) 70 bpm 60 to 100 bpm[3] cardiac output (CO) 4.9 L/minute 4.0 - 8.0 L/min Health History Chest pain – Do you have any chest pain or discomfort? • OLDCART – Do you do you use any recreational drugs? – Do you have any increased life stress/anxiety? Dyspnea – Do you have any labored or difficulty breathing (dyspnea)? • OLDCART • Related to exercise (exertional dyspnea)? – Quantify: Have far can you walk before getting short of breath? • Related to position/lying supine (orthopnea)? – How many pillows do you sleep on at night? Health History Palpitations – Ever have palpitations/or unpleasant awareness of heartbeat? (“fluttering/ pounding”) Dizziness or Syncope – Have you felt dizzy or ever lost consciousness/passed out (syncope)? Fatigue – Do you seem to tire easily? Cyanosis or pallor – Ever noted your facial skin turn blue or ashen gray? Health History Cough – Any pink or blood tinged frothy sputum? Edema – Do you have any swelling in your feet or legs? Nocturia – Do you awaken at night with an urgent need to urinate? Health History Past Cardiac History – CHF, angina, MI, murmurs, rheumatic fever, congenital heart disease Assess for risk factors of coronary artery disease – Hypertension, hyperlipidemia, diabetes, physical inactivity, obesity, smoking, stress, increasing age. family history of CAD (especially in 1st degree relatives F<65, M<55) – Additional for women: Menopause or use of oral contraceptives What the History Can Tell You Angina (pain resulting from ischemia) – Onset: Abrupt, often precipitated by event such as emotion, exertion, cold or eating. – Location: Substernal or retrosternal pain. – Duration: Usually lasts a few minutes and then subsides. – Characteristic: Described as squeezing or heavy pressure – Radiation: May radiate to the neck, jaw, or arms – Relieving Factors/Treatments Tried: Often relieved with sublingual nitroglycerin What the History Can Tell You Myocardial Infarction – – – – Onset: Abrupt, often unrelated to precipitating event. Location: Substernal or over precordium. Duration: Prolonged Characteristic: Severe, described as viselike or crushing – Associated Symptoms: dyspnea, dizziness, nausea, diaphoresis, palpitations, anxiety (sense of doom) – Radiation: May radiate to neck, jaw, arms or hands. – Treatments Tried: Sublingual nitroglycerin without relief What the History Can Tell You Congestive Heart Failure – Right-sided • Dependent Edema • Nocturia – Left-sided • • • • • • • Coughing/Hemoptysis (pink frothy) Orthopnea Dyspnea with exertion Cyanosis or ashen color Cold, moist extremities Oliguria Restlessness/anxiety Carotid Artery Inspect for pulsation – Absent pulse wave with arterial occlusion or stenosis Palpate lightly & one at a time for: – Contour • Smooth with rapid upstroke – Amplitude • • • • • • 4+ Bounding 3+ Full 2+ Normal 1+ Weak 0 Absent Diminished or unequal with atherosclerosis or other arterial disease Auscultate – Over angle of jaw, mid-cervical, & base of neck with bell – For presence of bruit • Blowing, swishing sound indicating turbulence http://www.youtube.com/watch?v=yq74c6KhPuo Carotid arteries 2+ bilaterally without bruits. Jugular Venous Pressure Assessment of jugular veins gives estimation of heart function – Ie. CHF Internal Jugular Vein – Position patient supine at 45 degrees without a pillow – Use Angle of Louis to read CVP at highest level of pulsation • Normal-Pulsation <2.5cm • Abnormal- Pulsation >2.5cm – Indicates increased CVP associated with heart failure http://www.youtube.com/watch?v=yq74c6KhPuo If you cannot find internal jugular veins, use the external and note point where look collapsed Jugular Venous Pressure External jugular veins are lateral to sternomastoid muscle above the clavicles Assess if: – Visible (distended) @ 45 ° External jugular veins flat @ 45 ° Hepatojugular Reflux Very sensitive in detecting right-sided heart failure Elevate to 30 degrees Press firmly in right upper quadrant Observe neck for elevation in JVP – Rise of >1cm is abnormal http://www.youtube.com/watch?v=X9fKPIe6nDQ Inspection & Palpation Inspect & palpate precordium for: – Lifts/Heaves – Thrills • Use ball of your hand firmly on the chest – Apical impulse – http://www.youtube.com/watch?v=FkM6m uqmve0&feature=related Apical impulse @ 5th intercostal space midclavicular line. No lifts, heaves, or thrills noted. Note location of heart may also be determined by percussing for borders of dullness Apical Impulse AKA: Point of maximal impulse (PMI) Apical impulse specifically for apex beat. Localize apical impulse using one finger. Ask to exhale and hold breath may help find. May need to roll midway to left. – Note: location, size (1cm x 2cm), amplitude (short gentle tap), duration (short, occupies only first half of systole – Not palpable in obese, thick chest wall Increased size or location with volume overload, hypertrophy (HTN, CAD, CHF, cardiomyopathy) Increased amplitude & duration with high cardiac output states (anxiety, fever, hyperthyroidism, anemia Auscultation Wth the diaphragm auscultate @ the apex of the heart for: – Rate • Normal Adult Rate: 60-100 beats/min • Bradycardia–heart rate less than 60 • Tachycardia–heart rate greater than 100. – Rhythm • • • • Regular vs. irregular Sinus arrythmia (rhythm varies with breathing) Regularly irregular, irregularly irregular If pulse irregular assess for pulse deficit – Auscultate the apical beat while simultaneously palpating the radial pulse. Every beat hear should perfuse to periphery Apical pulse 80bpm and regular. No pulse deficit noted. Auscultation Proceed over precordium with bell – Best for low pitch Auscultate over: – – – – – – Aortic area Pulmonic area Erb’s point Tricuspid area Mitral area Epigastric For: – Gallops (best with bell) – Murmurs (depends) – Rubs Normal Heart Sounds S1 – “Lubb” – Sound of mitral & tricuspid valve closing simultaneously • Start of systole – Heard loudest at apex of heart • Approx 5th intercostal space, midclavicular line on left S2 http://www.youtube.com/watch?v=2aO0HKIP3vI – “Dubb” – Sound of simultaneous closing of pulmonic and aortic valves • End of systole – Heard loudest at base of heart • Best over 2nd intercostal space on right Gallops: S3 & S4 Heart Sound Associated Heart Process S3 Early diastolic Heard @ apex or LL sternal border with bell S4 Normal Characteristics Heard more often in children and Occurs after S2 young adults Late diastolic (atrial filling) Heard @ apex Occurs before with bell S1 Pathological Characteristics Cadence Word Clue Higher pitch “Ken-tu-cky.” Louder ““SLOSH-ingin” Waxes and Wanes More constant sound May disappear when pt sits up Associated with volume overload and left ventricular systolic dysfunction No typical characteristics Seen in uncontrolled hypertension “Ten-nes-see” “a-STIFF-wall” Murmurs – Swishing or blowing noises that occurs with turbulent blood flow in heart or great vessels. – Categorized as: • Innocent – Always systolic & without evidence of physiological/structural abnormalities • Functional – Associated with physiological alterations such as high cardiac output states » i.e. exercise, anemia, hyperthyroidism or increased blood volume associated with pregnancy • Pathologic – Caused by structural abnormalities in valves or chambers » Stenosis, regurgitation, patent ductus arteriosis Structural Abnormalities in Valves and Chambers Murmur Characteristics Timing • Systolic: Heard during systole (between S1 and S2) – If possible note: early, late or mid systolic) • Diastolic: Heard during diastole (between S2 and S1) – If possible note: early, late or mid diastolic • Continuous: Heard in both systole and diastole http://www.youtube.com/watch?v=XvtBpnV_lOE Valvular Disease & Murmur Locations Valve Systolic Murmur Diastolic Murmur Aortic Aortic stenosis Aortic regurgitation Pulmonic Pulmonic stenosis Pulmonic regurgitation Mitral Mitral regurgitation Mitral stenosis Tricuspid Tricuspid regurgitation Tricuspid stenosis http://www.merckmanuals.com/professional/resources/multimedia/name/audio.html Murmur Characteristics Quality (Shape/Pattern & Sound) – Shape/Pattern • Crescendo/Decrescendo – AKA- Diamond shaped murmur; ejection type murmur – Primary causes: Stenotic valves • Holosystolic – AKA- Pansystolic • Decrescendo – Primary causes: Aortic and pulmonic regurgitation, Mitral and tricuspid stenosis http://www.merckmanuals.com/professional/resources/multimedia/name/audio.html Murmur Characteristics Quality – Sound • Musical, blowing, harsh, or rumbling Pitch – High, medium, or low; Loud or soft Location – Area of maximal intensity Radiation – May be heard in another place on precordium or neck, back or axilla Murmur Characteristics – Intensity (loudness) • 1 - Very faint, heard only after listener has “tuned in;” may not be heard in all positions • 2 - Quiet, but heard immediately after placing the stethoscope on the chest • 3 - Moderately loud • 4 – Loud, with palpable thrill • 5 - Very loud, with thrill. May be heard when stethoscope is partly off the chest • 6 – Very loud, with thrill. May be heard with stethoscope just removed from and not touching the skin. Murmur Characteristic Example Aortic Stenosis – Timing: Midsystolic – Pitch: Loud – Quality: Harsh – Location: Loudest @ 2nd right interspace – Radiation: Widely to side of neck, down left sternal border, or apex http://www.merckmanuals.com/professional/resources/multimedia/name/audio.html Auscultation Pericardial friction rub – Membranous sac surrounding heart becomes inflamed – Differentiate pericardial from pleural friction rub by having patient hold breath http://www.merckmanuals.com/professional/resources/multi media/name/audio.html Physical Exam Findings for CHF Right-Sided Failure Distended neck veins Dependent edema Ascites Hepatomegaly Nocturia Left-Sided Failure Pulmonary Edema – – – – – – Coughing Hemoptysis Orthopnea Dyspnea/Tachypnea Crackles in lungs Cyanotic nail beds, ashen color – Cold, moist extremities – Restlessness/anxiety http://www.youtube.com/watch?v=QODCQ HwSfOU&feature=related S3 gallop rhythm Tachycardia Peripheral Vascular & Lymphatics http://images.google.com Peripheral Vascular System Arteries – Supply oxygenated blood to the body from the heart Veins – Return unoxygenated blood to the heart – Contain one-way valves that keep the blood from flowing backwards – Muscles help squeeze the blood in the veins to the heart Health History Common or concerning symptoms – Pain in the arms or legs – Intermittent claudication: leg or arm pain that is exercise induced – Cold, numbness, pallor in the legs; hair loss – Color change in fingertips or toes in cold weather – Swelling in calves, legs or feet – Swelling with redness or tenderness – High risk: Tobacco use, diabetes, HTN, Hyperlipidemia, CV disease – Severity of peripheral vascular disease closely parallels the risk for heart attack, stoke, and death from vascular causes Inspection Inspect upper and lower extremities for: – Color – Symmetry – Lesions – Clubbing – Edema – Capillary refill Pitting Edema- Apply pressure with finger for 5 seconds. – 1+: Slight pitting, 1cm or less, disappears rapidly – 2+: Deeper pitting, 1.5cm, disappears 10-15 sec. – 3+: Deep pitting, 2cm, disappears more than 1 minute – 4+: Very deep pitting, 2.5cm, disappears 2-5 minutes No pitting edema noted Inspection Inspect lower extremities for – Hair distribution – Varicosities – Muscle atrophy Palpation Palpate upper and lower extremities for: – Temperature – Texture – Capillary refill – Lymph nodes • Epitrochlear, Inguinal Lymph Nodes Epitrochlear – In antecubital fossa and drains: • Hand • Lower hand Inguinal – In groin and drains most of the lymph • Lower extremities • External genitalia • Anterior abdominal wall Palpation Peripheral Pulses – Brachial, radial, femoral, popliteal, posterior tibial, dorsalis pedis • Assess for symmetry in limbs • Force – – – – – 4+ Bounding 3+ Full, increased 2+ Normal 1+ Weak 0 Absent If pulse is difficult to palpate use a Doppler (ultrasound stethoscope) to amplify sound of pulse wave Peripheral Pulses- Brachial Located medial to biceps tendon Grade force bilaterally Peripheral Pulses-Radial Note: – Rate – Rhythm – Force Peripheral Pulses-Ulnar Modified Allen Test – Evaluate adequacy of collateral circulation prior to cannulating radial artery – Firmly occlude both ulnar and radial arteries – Release pressure on ulnar artery – Normal- return of color in 2-5 seconds Peripheral Pulses-Femoral Located just below inguinal ligament halfway between the pubis and anterior superior iliac spine. Grade force bilaterally If weak auscultate for bruit Peripheral Pulses-Popliteal Located just lateral to medial tendon Grade force bilaterally Peripheral Pulses-Posterior Tibial Located behind the groove between the malleolus and Achilles tendon Grade force bilaterally Peripheral Pulses-Dorsalis Pedis Located just lateral to & parallel with the extensor tendon of the big toe. Force should be symmetrical Assess for Deep Vein Thrombosis Assess for: – Erythema – Calf Edema – Increased warmth No calf erythema, edema, warmth No longer widely practiced – Tenderness with palpation – Homan’s sign No calf erythema, edema, or warmth. Venous vs. Arterial Insufficiency Assessment Criterion Venous Arterial Color Normal or cyanotic Pale; worsened by elevation; dusky red when extremity is lowered Temperature Normal Cool (blood flow blocked to extremity) Pulse Normal Decreased or absent Edema Often marked Absent or mild Skin Changes Brown pigment around ankles Thin, shiny skin; decreased hair growth; thickened nails. Arterial Venous Is that all? MIDTERM 40 points all multiple choice