Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
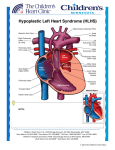
Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Hypoplastic left heart syndrome Oliver Stumper Heart 2010 96: 231-236 doi: 10.1136/hrt.2008.159889 Updated information and services can be found at: http://heart.bmj.com/content/96/3/231.full.html These include: Supplemental Material http://heart.bmj.com/content/suppl/2010/01/04/96.3.231.DC1.html References This article cites 20 articles, 12 of which can be accessed free at: http://heart.bmj.com/content/96/3/231.full.html#ref-list-1 Email alerting service Topic collections Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Articles on similar topics can be found in the following collections Congenital Heart Disease (9 articles) Notes To order reprints of this article go to: http://heart.bmj.com/cgi/reprintform To subscribe to Heart go to: http://heart.bmj.com/subscriptions Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart CONGENITAL HEART DISEASE Hypoplastic left heart syndrome Oliver Stumper < Additional references are published online only at http:// heart.bmj.com/content/vol96/ issue3 Correspondence to Dr Oliver Stumper, Birmingham Children’s Hospital NHS Trust, Birmingham, UK; [email protected] Hypoplastic left heart syndrome describes a range of congenital cardiac lesions, which have in common a small left ventricle which is unable to support the systemic circulation. Typically the volume of the small left ventricle is <20 ml/m2 body surface area (BSA). A number of fetal cardiac anomalies have been shown to cause this problemdnamely, aortic or mitral atresia, with or without mitral or aortic valve stenosis, or an unbalanced atrioventricular septal defect.1 Despite the heart being basically fully developed at some 8 weeks of gestation, the growth of cardiac structures is entirely dependent on a normal fetal circulation. Thus, it comes as no surprise that pronounced aortic stenosis, detected in a fetus at some 18e20 weeks gestation, may progress to present at birth as classical hypoplastic left heart syndrome (HLHS).2 The common presentation of newborns with hypoplastic left heart syndrome at birth is cardiovascular collapse and shock. The peripheral pulses are weak, without major difference between the brachial and femoral pulses. There is usually a mild to moderate degree of cyanosis, but no differential cyanosis. Chest x-ray normally shows cardiomegaly and plethoric lung fields. The ECG documents right ventricular hypertrophy and reduced left ventricular forces. If the diagnosis is suspected, the administration of a prostaglandin infusion at the rate of 5e20 ng/kg/min normally maintains patency of the ductus arteriosus, and will prevent further cardiovascular compromise, progressive acidosis and death. Assessment by cardiac ultrasound will make the definitive diagnosis, allow for optimisation of initial treatment and detailed discussion of the treatment options and outcomes with the parents. The initial description of a surgical procedure to palliate hypoplastic left heart syndrome in neonates was provided by William Norwood in 1982.3 This allowed neonates to survive into infancy when more palliative surgery was required. The evolution of these techniques has progressed over the past 25 years, and nowadays the Norwood/ Fontan palliation of children with HLHS can produce very acceptable early and medium term results. In the UK, the surgical treatment of a newborn with HLHS became available only in early 1993. Results of this initial Norwood procedure and the subsequent bidirectional cavopulmonary shunt and Fontan procedure have improved steadily over time, with 5 year survival now approaching 70%.4e6 Before this, attempts were made to bridge children Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889 to primary neonatal heart transplantation, either by medium term prostaglandin infusion or by stenting the arterial duct, together with banding the pulmonary arteries. However, results were disappointing in this early phase (1990) and neonatal primary heart transplantation can no longer be viewed as a viable option. GENETICS HLHS has been reported to occur in approximately 0.016e0.036% of all live births, representing some 2% of all congenital cardiac defects. Boys are twice as commonly affected as girls. Over the recent years the molecular basis for left heart obstructive lesions has been better understood, in part due to their dominant inheritance despite low penetrance and variable expression.7 Gene mutations of NKX2.5 and NOTCH1, involved in cardiac development, have been identified in some cases. Overall these new insights raise the prospect of improved genetic counselling in future. ANTENATAL DIAGNOSIS The percentage of children with HLHS who are diagnosed antenatally is increasing, due to the widespread establishment of adequate ultrasound screening programmes over the past two decades. Currently some 60% of fetuses are detected antenatally. Parents are given earlier and more detailed counselling regarding the treatment options and the anticipated outcome in their children. Nonetheless, improved antenatal diagnosis has generally not resulted in an improved outcome postnatally.8 This may be based on the fact that antenatal diagnosis allows more rapid and dedicated initial management, and allows for survival of neonates with HLHS and significant comorbidities such as a highly restrictive atrial septum or other organ system lesions. Currently about 50% of parents, following antenatal diagnosis of HLHS in their child before 20 weeks gestation, decide to electively terminate the pregnancy.9 The drive to perform antenatal scans at an earlier gestational age is likely to decrease the overall sensitivity of the screening programmes, as it is known that HLHS may develop late in pregnancy and thus may not be apparent at a 14 week scan. Several pilot studies have been conducted into catheter or surgical interventions in fetuses with antenatally detected HLHS. In particular, in fetuses with severe aortic stenosis, the aim was to open up the aortic valve and promote anterograde flow and ultimately growth of the left heart structures. Similarly, the subgroup of fetuses detected with 231 Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart a highly restrictive, or, occasionally, intact atrial septum are sometimes considered for fetal intervention (balloon atrial septostomy). Such procedures are currently experimental and the actual benefit of such interventions cannot be ascertained at present.10 INITIAL MANAGEMENT Neonates with HLHS are normally born at term and with a normal birth weightda reflection of the fact that this serious congenital cardiac defect is well tolerated during fetal development. Postnatally the ductus arteriosus will close and pulmonary vascular resistance will drop, resulting in cardiovascular collapse unless treated rapidly. Patency of the ductus arteriosus must be maintained by prostaglandin infusion (5e20 ng/kg/min). In the past, attempts were made to address the drop in pulmonary vascular resistance, and the resulting pulmonary over-circulation, by low frequency ventilation, raising the partial pressure of carbon dioxide (PCO2), using low inspired oxygen concentrations, increasing dead space ventilation, or even adding CO2 to the inspired gas. Thus, in the past, early management focused on increasing pulmonary vascular resistance and thereby limiting pulmonary blood flow. In contrast, nowadays, the thrust of preoperative management is towards better systemic tissue perfusion, using systemic afterload reducing agents, ino-dilators and addressing systemic acidosis early and aggressively.11 COUNSELLING HLHS remains a very severe congenital cardiac defect, which is not compatible with survival unless treated. Despite the improvements in cardiological and cardiac surgical management, the medium term survival remains limited and the functional status of the survivors is limited compared to normal. Even though stage I surgery can now be offered with an early mortality rate of some 15%, parents have to understand fully the implications of embarking on long term palliative care of their newborn child. Survival at 1, 5 and 10 years is some 75%, 70% and 65%, respectively, in the largest series reported. These figures, however, do not quote the risk of survival with very poor functional outcome or gross neurological deficit or the uncertainty about future limited treatment options if the systemic right ventricle fails. Consenting for treatment of children with hypoplastic left heart syndrome must include these issues, particularly as cardiac transplantation in this group of patients will never be an easy and widely available option. STAGE I NORWOOD PROCEDURE The original initial surgical palliation comprised aortic arch reconstruction, atrial septectomy, endto-side anastomosis of the main pulmonary artery to the, sometimes, diminutive ascending aorta, and creation of a BlalockeTaussig shunt to the reconstructed central pulmonary arteries.3 The aortic 232 arch reconstruction is almost universally achieved by opening the underside of the aortic arch longitudinally and by placing a generous patch of homograft material along the entire length, extending distally beyond the site of coarctation (figure 1dstage 1a). Various techniques have been employed to enlarge the proximal end of this reconstruction, so as to allow for an increased size of the native ascending aorta and improved coronary perfusion. The size of the Gore-Tex tube to create a BlalockeTaussig shunt has decreased over time, so as to limit diastolic run-off to the pulmonary arteries and avoid volume loading of the systemic right ventricle. The standard shunt size is now 3.5 mm (3 mm in neonates <2.5 kg bodyweight). This classical Norwood procedure was replaced, by many centres, by implanting a non-valved tube from the right ventricle to the left pulmonary artery (Sano modification12) and later, at Birmingham Children’s Hospital (BCH), to the right pulmonary artery, instead of the original modified BlalockeTaussig shunt (figure 1dstage 1b). These modifications have led, in many units, to an improved early survival and improved early postoperative course in the intensive care unit (ICU).13 The main advantage of this modification is improved coronary and systemic perfusion due to the absence of diastolic run-off down a BlalockeTaussig shunt. However, further analysis and comparison of detailed haemodynamic data and postoperative variables documented that systemic arterial mean pressures were comparable and that there were no significant differences in markers of pulmonary blood flow or in markers of systemic blood flow (blood lactate, oxygen extraction ratio), or in the estimated ratio of pulmonary:systemic blood flow (Qp:Qs). There were no significant differences in markers of cerebral blood flow or renal and hepatic function in the early postoperative period.14 The growth of the branch pulmonary arteries was found to be improved after creation of a right ventricle to pulmonary artery conduit instead of a BlalockeTaussig shunt.15 This is most likely due to the pulsatile nature of pulmonary blood flow after this modification. Nonetheless the incidence of significant branch pulmonary artery stenosis at the site of conduit insertion was found to be increased, and surgical reconstruction was cumbersome. The latter was the major stimulus for placing the right ventricleepulmonary artery (RV-PA) shunt to the right of the end-to-side connection of the pulmonary artery with the ascending aorta, as introduced at BCH in 2004. Any encountered branch pulmonary artery stenosis at the site of insertion of the non-valved tube is more easily relieved during the subsequent cavopulmonary shunt and can be roofed over by the superior caval vein. Despite these modifications, the 1 year survival that has been achieved by RV-PA approach is now also achieved by some centres utilising the classical Norwood procedure, utilising a BlalockeTaussig shunt. This has led to the design of a multicentre randomised trial carried out in the USA to compare these two approaches. Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889 Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart Pre-op Stage 1 a b c Stage 2 Stage 3 Figure 1 Hypoplastic left heart syndrome from birth to final palliation. Pre-op: hypoplastic left ventricle and a diminuitive ascending aorta with duct dependant systemic circulation. Stage 1: a. classical Norwood procedure with a modified BlalockeTaussig shunt. b. The Sano modification with a right sided RV-PA conduit. c. The hybrid stage 1 palliation with bilateral pulmonary artery bands and a stent within the systemic ductus arteriosus. Stage 2: the superior vena cava is anastomosed to the right pulmonary artery to provide the sole source of pulmonary blood flow. Stage 3: the inferior vena cava and the hepatic veins are rerouted to the pulmonary arteries by means of a Gore-Tex conduitdthe circulation is in series with a systemic right ventricle. Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889 233 Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart A further important cardiac surgical focus is on optimising bypass techniques, avoiding circulatory arrest and maintaining low flow cerebral perfusion throughout the arch reconstruction, so as to limit potential neurologic damage during the stage I procedure and to ensure best possible neurocognitive outcome in the long run. As yet, no significant differences between these techniques have been identified. Significant independent risk factors for early mortality in almost all reported surgical series include: low patient weight (<2.5 kg); a diminutive ascending aorta of <2 mm in size; a restrictive, or sometimes intact, atrial septum; an unbalanced atrioventricular septal defect; or associated noncardiac abnormalities or chromosomal defects. In such cases, a growing number of centres now offer an alternative to the classical or modified Norwood stage I palliation. This was introduced mainly by the Giessen group and was further modified by the Columbus group, and is now labelled a hybrid stage 1 procedure.16 17 Through a median sternotomy, bilateral pulmonary artery bands are placed surgically to limit pulmonary blood flow. A stent is placed across the systemic ductus arteriosus, either during the same procedure or at a later stage, to maintain unrestrictive flow from the right ventricle to the systemic circulation (figure 1dstage 1c). Restriction at the level of the atrial septum is addressed either by static or dynamic balloon septostomy or by stent placement. Despite the initial learning curve, the immediate results of this procedure are excellent. However, there remains a significant interstage mortality and also a notably increased risk of the so-called comprehensive stage 2 procedure. During this procedure the aortic arch and pulmonary artery reconstruction have to be performed, together with the anastomosis of the ascending aorta with the main pulmonary artery, the atrial septectomy and the cavopulmonary shunt. Again, in some pioneering centres, excellent results with this approach have been achieved. Medium term results and data on neurocognitive development and ability scores after these different strategies are needed, and are eagerly awaited, to formulate better the optimal management approach to this relatively common congenital cardiac lesion. Several studies have documented that overall survival at the different stages of the Norwood palliation is improved in centres with a high activity compared to those with very small numbers.18 The array of options currently available to embark on initial treatment of neonates with HLHS should not promote a decentralised approach to this complex problem. INTERSTAGE MORTALITY Early on during the experience with the Norwood palliation in larger series of patients with HLHS it became apparent that a fair number of hospital survivors after stage I palliation were discharged home in a very satisfactory condition, and then died suddenly at home before undergoing stage II 234 palliation. Retrospective analysis of these cases has revealed that, in particular, children with a diminutive sized ascending aorta are at risk of sudden death. This is likely to be related to inadequate coronary perfusion either at the level of the Damus connection or due to the small size of the ascending aorta. Further factors identified included an acute blockage of the BlalockeTaussig shunt, obstruction to the pulmonary arteries, development of obstruction of the reconstructed aortic arch, or a restriction to the atrial septum. All of these potential problems can be exasperated by an acute illness such as diarrhoea and vomiting, severe reflux with aspiration or a viral infection. Acute interstage mortality has remained an issue also with the newer Sano-modification (RV-PA conduit) or a hybrid stage I procedure. At present there is no significant difference in 1 year survival after any of these approaches, despite some apparent differences in stage I mortality. Over the years there has been much focus on reducing interstage mortality, by developing sophisticated home monitoring programmes and very frequent cardiological reviews.19 Although these measures have been shown to have significant impact, they have not completely eradicated this problem. Further work in this area is required to eventually produce better 1 year overall survival after palliative surgery for HLHS. STAGE II PROCEDURE After some 4e6 months of age, children who underwent stage I palliation (either the classical Norwood procedure or a modification utilising a conduit from the right ventricle to the pulmonary arteries), suffer from severe cyanosis due to very limited pulmonary blood supply. At the same time pulmonary vascular resistance has decreased significantly from the initially high levels shortly after birth. At this stage it is common practice to proceed to the surgical creation of a bidirectional cavopulmonary shunt with interruption of the original BlalockeTaussig shunt or the conduit from the right ventricle to the pulmonary artery. Most centres continue to perform a cardiac catheterisation procedure preoperatively, so as to obtain direct haemodynamic measurements and to address the relatively common finding of aortic arch obstruction by balloon angioplasty. After the cavopulmonary shunt, the systemic venous return of the upper body half is redirected to the lungs without the use of an effective pumping chamber (figure 1dstage 2). As long as the pulmonary arteries are of good size and there is a well developed pulmonary capillary bed and no restriction at the level of the pulmonary venous drainage or the atrial septum, this procedure provides a very good functional result. Initial resting saturations are commonly around 85e90% in air. As this “shunt” is created without the use of artificial material there is normally good growth of the anastomosis during early childhood. However, as there is a relative decrease in the amount of superior caval venous return towards later childhood, Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889 Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart children will again suffer from pronounced cyanosis towards 4e5 years of age. This is aggravated by the fact that common activities, such as running, will increase the amount of desaturated inferior caval venous blood to the circulation and will worsen the cyanosis very rapidly. Cardiac catheterisation is normally again performed before embarking on further surgical management to assess pulmonary artery size, distribution and pressures, but also to rule out any recurrent aortic arch obstructions, systemic venous fistulae or significant systemic collateral arteries to the pulmonary circulation. All of these lesions can be addressed by interventional cardiac catheter techniques with very good results, and reduce the risk of the subsequent Fontan procedure. STAGE III SURGERY At some 3e5 years of age, children with HLHS who have undergone stage I and II surgery will get increasingly tired, breathless and cyanosed after mild to moderate activity. Surgical connection of the inferior caval venous return to the pulmonary arteries, without the use of an effective pumping chamber, will redirect all desaturated blood to the pulmonary vasculature before returning to the heart. This is the completion of the Fontan circulation. Today most centres use an extracardiac PTFE (polytetrafluoroethylene) conduit to achieve this (figure 1dstage 3). The majority of centres create a fenestration with the pulmonary venous atrium, so as to allow for a small right-to-left shunt to limit the pressure within the Fontan circuit, and to prevent diastolic dysfunction of the systemic right ventricle in the early postoperative period due to a fall in overall cardiac output and ventricular preload. The early mortality of such a procedure now approaches zero in appropriately selected patients with maintained right ventricular function. In children with decreased right ventricular function and moderate-to-severe tricuspid valve regurgitation, an attempt at valve repair should be made first, rather than embarking on Fontan completion at the same time. The morbidity after Fontan completion in patients with HLHS remains high, mostly due to the common occurrence of prolonged pleural effusions. NEURODEVELOPMENTAL OUTCOME Presently, there are only very few studies available to assess the cognitive development and the neurodevelopmental outcome and quality of life of patients after surgical palliation for HLHS. Initial work suggests that the outcome measures are within the normal range, but the overall performance of the entire cohort is lower than that of the general age matched population. Comparison of outcome indices should ideally be performed by matching other groups of patients with cyanotic congenital heart disease, requiring bypass surgery during the first weeks of life, such as patients with complete transposition of the great arteries, or Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889 those with longstanding cyanosis in early childhood. There is some recent evidence that the cerebral arterial blood supply in infants with HLHS is reduced compared to normal, which, in itself, could have an impact on overall neurocognitive outcome.20 One of the factors identified for reduced cognitive development is the use of deep hypothermic circulatory arrest during the initial Norwood stage I palliation. Most centres now use continuous low flow cerebral perfusion during the stage 1 procedure. This is likely to reduce the potential for neurological damage during the early neonatal period. Studies are being designed to evaluate any differences in outcome among children who have undergone a classical Norwood stage I procedure compared to those who received a Sano modification. In due course this line of research will also be able to evaluate any potential differences in outcome in the growing group of patients who undergo a hybrid stage 1 procedure, without the use of cardiopulmonary bypass, during their initial palliation. THE POST-FONTAN STATE After completion of the Fontan the circulation is in series, being supported by only one ventricle, which is of right ventricular morphology. The myocardial architecture of the right ventricle is significantly different from the left ventricle, having only two layers of myocardial fibres and having a substantially different pattern of contraction and shortening. Systemic and pulmonary vascular resistances represent the combined afterload to this right ventricle. The right ventricle has to function in the context of a limited coronary flow reserve, due to the Damus connection and a generally small ascending aorta, which merely serves as a conduit to the coronary arteries themselves. Medium term survival in patients with either a right or a left ventricular dependent Fontan circulation is comparable, but more detailed functional assessments are currently still awaited. Systemic venous pressures are significantly elevated after the Fontan procedure, resulting in a degree of liver dysfunction and chronic gut oedema. The Fontan circulation is associated with a pro-coagulable state, suggesting the use of long term antiplatelet or anticoagulation therapy. As yet, no prospective trials in this field have been concluded and there is a wide variability to centre specific preference of postoperative chronic medication and management protocols. Furthermore, endothelial function is significantly altered in the context of non-pulsatile pulmonary blood flow, leading to an increased pulmonary vascular resistance. Selective pulmonary vasodilators have shown promising initial results in the management of some post-Fontan complications, as did de novo fenestration of the Fontan circuit to establish a right-to-left shunt and decreasing right atrial pressure. Despite the very significant strides in the initial treatment and palliation of neonates with HLHS, the medium to long term outcome of children and 235 Downloaded from heart.bmj.com on February 14, 2010 - Published by group.bmj.com Education in Heart < You can get CPD/CME credits for Education in Heart 5. Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiologydyou need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education. dtl < RCP credits: Log your activity in your CPD diary online (http://www. rcplondon.ac.uk/members/CPDdiary/index.asp)dpass mark is 80%. < EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQsdpass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/ newsite/?hit¼men02). Please note: The MCQs are hosted on BMJ Learningdthe best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit. 6. 7. 8. 9. 10. < 11. < 12. increasing numbers of adolescents and adults with Norwood palliation of HLHS remains uncertain. It will require the input of a highly dedicated and trained team of cardiologists, physicians and surgeons to achieve the best possible outcome and quality of life. Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The author has no competing interests. Provenance and peer review Commissioned; not externally peer reviewed. 13. 14. 15. 16. < 17. REFERENCES 1. 2. 3. 4. 236 Tchervenkov CI, Jacobs ML, Tahta SA. Congenital Heart Surgery Nomenclature and Database Project: hypoplastic left heart syndrome. Ann Thorac Surg 2000;69IV:S170e9. Makikallio K, McElhinney DB, Levine JC, et al. Fetal aortic valve stenosis and the evolution of hypoplastic left heart syndrome. Circulation 2006;113:1401e5. Norwood WI, Lang P, Hansen DD. Physiologic repair of aortic atresiaehypoplastic left heart syndrome. N Engl J Med 1983;308:23e6. Stasik CN, Goldberg CS, Bove EL, et al. Current outcomes and risk factors for the Norwood procedure. J Thorac Cardiovasc Surg 2006;131:412e17. 18. 19. < 20. Detailed analysis of a large single centre cohort of contemporary Norwood stage I procedures to assess risk factors and outcomes. Tweddell JS, Hoffman Gm, Mussatto KA, et al. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation 2002;106(Suppl I):182e89. Griselli M, McGuirk SP, Stumper O, et al. Influence of surgical strategies on outcome after Norwood Procedure. J Thorac Cardiovasc Surg 2006;131:418e26. McBride KL, Zender GA, Fitzgerald-Butt SM, et al. Linkage analysis of left ventricular outflow tract malformations (aortic valve stenosis, coarctation of the aorta, and hypoplastic left heart syndrome). Eur J Hum Genet 2009;17:811e9. Sullivan ID. Prenatal diagnosis of structural heart disease: does it make a difference to survival? Heart 2002;87:405e6. Rasiah SV, Ewer AK, Miller P, et al. Antenatal perspective of hypoplastic left heart syndrome. Arch Dis Child Fetal Neonatal Ed 2008;93:192e7. Pavlovic M, Acharya G, Huhta JC. Controversies of fetal cardiac intervention. Early Hum Dev 2008;84:149e53. Critical appraisal of the options, techniques and outcome of fetal cardiac interventions against current postnatal options and results. Wernovsky G, Ghanayem N, Ohye RG, et al. Hypoplastic left heart syndrome: consensus and controversies in 2007. Cardiol Young 2007;17:75e86. Review of the current practice in the preoperative management of children with hypoplastic left heart syndrome and perioperative stage 1 management. Sano S, Ishino K, Kawada M, et al. Right ventricleepulmonary artery shunt in first stage palliation of hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 2003;126:504e10. Pizarro C, Malec E, Maher KO, et al. Right ventricle to pulmonary artery conduit improves outcome after stage I Norwood for hypoplastic left heart syndrome. Circulation 2003;108:II155e60. Ghanayem NS, Jaquiss RD, Cava JR, et al. Right ventricle-topulmonary artery conduit versus Blalock-Taussig shunt: a hemodynamic comparison. Ann Thorac Surg 2006;82:1603e9. Rumball EM, McGuirk SP, Stumper O, et al. The RV-PA conduit stimulates better growth of the pulmonary arteries in hypoplastic left heart syndrome. Eur J Cardiothorac Surg 2005;27:801e6. Akintuerk H, Michael-Behnke I, Valeske K, et al. Stenting of the arterial duct and banding of the pulmonary arteries. Basis for combined Norwood stage 1 and 2 repair in hypoplastic left heart. Circulation 2002;105:1099e103. The initial experience with combined pulmonary artery banding and stenting of the ductus arteriosus as an alternative to classical Norwood palliation. Galantowicz M, Cheatham JP, Phillips A, et al. Hybrid approach for hypoplastic left heart syndrome: intermediate results after the learning curve. Ann Thorac Surg 2008;85:2063e71. Hirsch JC, Gurney JG, Donohue JE, et al. Hospital mortality for Norwood and arterial switch operations as a function of institutional volume. Pediatr Cardiol 2008;29:713e7. Ghanayem NS, Hoffman GM, Mussatto KA, et al. Home surveillance program prevents interstage mortality after the Norwood procedure. J Thorac Cardiovasc Surg 2003;126:1367e77. Impact of a dedicated home surveillance programme to improve on interstage mortality after stage I palliation. Licht DJ, Wang J, Silvestre DW, et al. Preoperative cerebral blood flow is diminished in neonates with severe congenital heart defects. J Thorac Cardiovasc Surg 2004;128:841e49. Heart 2010;96:231e236. doi:10.1136/hrt.2008.159889