Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
Immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Innate immune system wikipedia , lookup
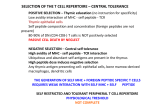
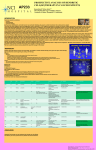
DENDRITIC CELL(DC)THERAPY AP224 IN TRIPLE NEGATIVE BREAST CANCER Kananathan.R*,Khan Jamal** *NCI Hospital,Nilai Negeri Sembilan, Malaysia **Institute of Cellular Therapy(ICT) ,Noida,India INTRODUCTION Cancer is caused by mutations. Familial Environmental Unknown etiology. During cancer development, self-cells become non-self cells. Mutating cells acquire a shield mechanism for evading immune attack. They may hide their antigenic nature by topographic shield or produce IL-10 for negative chemotaxis or develop an unknown hidden mechanism to evade their arrest. Once the cancer cells start proliferating, the immune mechanisms become so ineffective, that it actually starts contributing towards cancer proliferation. At this stage, cancer develops rapidly and profoundly. Otherwise cancer growth may become slower or delayed if immune system is still able to check it irregularly. The deranged immune system can be corrected passively by chemotherapy and/or surgery. If it happens this way, cancer patients become cancer survivors, or otherwise, cancer returns with vengeance making itself more resistant to chemotherapeutic drugs used earlier. Normal anti-cancer immunology can be enhanced in laboratory as well. The peripheral blood mononuclear cells are isolated from peripheral blood and cultured with specific cytokines for changing their morphology to dendritic cells. The dendritic cells are given a basic information of cancer type, by adding tumor associated antigens (TAA) and tumor specific antigens (TSA) to the culture plates. First described by the late Professor Ralph Steinmen in the late 1980 dendritic cells are now found to have essential roles in cancer therapy Dendritic cells recognize the antigen feedback and respond by producing specific antigenic peptides (representation) on their surfaces. These mature dendritic cells are re-infused to the same patient after eight days of culture for generating specific anti-cancer immunity. After infusion, these dendritic cells along with specific cytokines are carried to various lymph nodes and station themselves in these lymph nodes. They start their physiological action on naïve T cells. Upon physiological contact with dendrites of DC, T cells become committed in the vicinity of dendritic cells. Each dendritic cell has the potential to mature to about 3000-5000 T cells/hour. Dendritic cell survives on an average of 3 weeks to months, and during this period it is able to selectively transform trillions of T cells. The robust anticancer immunology doesn’t allow new malignant cells to grow and effectively stops or delays tumor progression. Dendritic cells leading to IL-12 and TNF-alpha generation also generate humoral immunology which results in reducing cachexia. CASE REPORT AR 36years old lady first diagnosed on 13th Jan 2005 with CA Left Breast Stage IIIC and Triple negative disease was treated at St Elsewhere with FAC 6cycles and radiotherapy. She develop her 1st local recurrence late 2007 and underwent local surgical excision and was subjected to single agent Taxotere for 6 cycles at the same centre. Six months post Taxotere she develop a second recurrence at the area of excision and she was given local radiotherapy over 10times at the same centre. She came to see the primary author for DC Therapy as she felt it would recur in less than 6 months . She was started on DC cell therapy on 16th Jan 2010.Her Full blood count,renal function and liver function improved with time and she did not have any side effects post infusion. She was given monthly infusions over 4 months. She opted to stop in view of cost. Her husband made a comment that after such along period they have being able to stay away from the hospital. Her last admission was one year ago. She is seen regularly at the clinic. She was seen every 3 months at the outpatient clinic. Her latest clinical examination and radiography evaluation done shows she is clear from disease. She has been progression free since 16th Jan 2010 coming to 22months. CONCLUSION DC therapy for our patient had no side effects. Triple negative breast cancer in the young patient runs a virulent course. New modalities of therapy needs to be investigated. The role of Denvax following a second recurrence of a triple negative should be investigated. . Presented at the 21st Asian Pacific Cancer Conference 10 to 12th November 2011 Dedicated to Late Dr G Selvaratnam ,patients and the staff’of NCI