Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Basal metabolic rate wikipedia , lookup
Metalloprotein wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Metabolic network modelling wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Biosynthesis wikipedia , lookup
Pharmacometabolomics wikipedia , lookup
Drug design wikipedia , lookup
Enzyme inhibitor wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
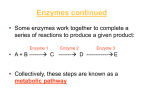
DRUG METABOLISM Department of Pharmaceutics Drug metabolism or Biotransformation is the major mechanism for elimination of drug from the body. It is the process by which the drug is chemically modified inthe body and the end product of modification is called METABOLITE Liver is the major site for metabolism,along with other organs like kidneys,lungs,blood,skin,saliva,etc; Drug metabolism involves conversion of one form of drug to another form………it may be enzymatic or non-enzymatic. Generally in liver major metabolism takes place at microsomes which are present in the endoplasmic reticulum.The microsomal enzymes are responsible for Metabolising the compounds. Hence drug metabolism can be classified as 1. Microsomal 2. Non-microsomal DRUG LATENTIATION: when a delayed or prolonged release/response of drug is required,normally inactive forms or precursors of the drugs can be commonly used in pharmaceutical practice.so that the active forms will generates in the body. Such approach is said to be DRUG LATENTIATION Ex: chloraamphenicol palmitate,Dichloralphenezone, Estolates and steroids. WHY DRUG METABOLISM/IMPORTANCE OF METABOLISM As all the chemical substance are not nutrients to the body,whatever the foreign compounds entering in to the body are called exogenous compounds or xenoboitic Generally drugs get excreted based on their lipophilicity, all the drugs available are not lipophilic,some may be hydrophilic,the hydrophilic moleculesmay get excreted through urine,but lipophilic molecules will undergorebsorption from renal tubules in to blood after glomerular filtration. So that the drug get accumilated in the body which leads to toxicity. The metabolic system will makes the lipophilic moeities to make water soluble. So the drug willl be easily excreted,hence the frug biotransformation isprocess is also called as DETOXIFICATION PROCESS PHASE 1 Oxidation(microsomal) Aromatic hydroxylation Aliphatic hydroxylation Epoxidation N-Dealkylation O-Dealkylation S-Dealkylation Oxidative deamination N-Oxidation S-Oxidation Phosphotionate oxidation Dehalogenation Oxidation(non-microsmal) Alcohol dehydrogenase Aldehyde oxidation Xanthine oxidase Amine oxidase Aromatases PHASE 2 Conjugation with sugars (1) Glucuronidation O-Glucuronides N-Glucuronides (2)Conjugation with other sugars. Sulfation Methylation Acetylation Aminoacid conjugation Glutathione conjugation Fattyacid conjugation Condensation reactions PHASE 1 Reduction Azo reduction Nitro reduction Reduction dehalogenation Hydrolysis Ester hydrolysis Amide hydrolysis Hydrazine&carbamate hydrolysis Hydration Other minor reactions PHASE2 OBJECTIVE OF PHASE 1 REACTIONS 1. Increase in hydrophilicity 2. Reduction in stability. 3. Facilitation of conjugation………leads to phase 2 reaction makes the drug hydrophilic. The compounds which are failed to undergo phase -2 reaction will preceeds to phase-3 to avoid 1. Toxicity to cell components 2. Hydrolysis of conjugates back to reactive species. 3. Inhibition of phase-2 enzymes. OXIDATION INVOLVING MICROSOMAL MIXED FUNCTION OXIDASE(MFO’S) Oxidation of compound r drug is catalysed by many enzymes located in microsomes.such enzymes requires both molecular oxygen and reducing agents NADPH to effect reaction.therefore they are refered as mixed function oxidases or mono oxidases (MFO) They are located in the endoplasmic reticulum of hepatic cells performs many functions.The MFO are structuraal enzymes requires NADPH,O2,CYT P 450,NADPH-CYTP450 reductase enzyme & phospholipids. CYT P450 is an enzyme responsible for oxidation and reduction reactions.Chemially it is a heme protien containing iron. reduction cycle. The following figure shows the CYT P 450 oxidation- NON MICROSOMAL OXIDATION In these type enzymes like alcohol dehydrogenase,aldehyde dehydrogenase, xanthine oxidase,amine oxidases,aromatase etc; are included…… REDUCTION Hepatic microsomes catalyses various reduction reactions and requires NADPH for this purpose.Azo and nitro reductions is catalysed by CYT P 450 reductase enzyme HYDROLYSIS Liver microsomes and ther tissues contain non specific esterases and Hydrolytic enzymes. so that they undergo hyrolytic reactions. HYDRATION Hydration can be regarded as specialised form of hydrolysis,where water is added to the compound with out causing the compound to dissociate in to no.of components. EX: Epoxides are converted in to di hydrodiols,by the enzyme epoxide hydratase PHASE 2 REACTIONS REACTION ENZYME FUNCTIONAL GROUP Glucoronidation UDP-Glucoronyl transferase OH,-COOH,-NH2,SH Glycosidation UDP-Glucoronyl transferase -OH,-COOH,-SH Sulfation sulfo Transferase -OH,-NH2,-SO2NH2 Methylation Methyl transferase -OH,NH2. Acetylation Methyl transferase -OH,-NH2,-SO2NH2,COOH. Aminoacid conjugation ………….. -COOH. Fattyacid …………… -OH. Glutathione conjugation Gluthion-sTransferase Epoxide organic halides condensation ………………. various GLUCORONIDATION Glucoronidation means conjugation reaction of sugars with D-Glucoronic acid, xylose,arabinose and glucose. Glucoronidation involves the reaction between the high energy form of conjugating agent with uridine di phosphate glucornic acid and drugs containing hydroxyl,carboxyl,amine or thiol groups. The reaction is mediated by glucoronyl transferase. GLUTATHIONE CONJUGATION Glutathione (GSH) is a tripeptide of glutamyl-cysteine-glycine That is recognized as a protective device with the cell for the Removal of potentially toxic electrophilic compounds GSH reacts non-enzymatically and enzymatically via glutathion-s-Transferase, through the nucleophilic sulfhydral group with Reactive electrophilic oxygen intermediates of certain drugs Formed during oxidative biotransformation reactions. These Reactive electrophilic intermediates my react with nucleophilic macromolecules such as proteins in the cell, leading to a cell Injury and cellular necrosis The enzyme catalyzing these reactions are the glutathione-s-transeferase located in the cytosol of the liver,kidney and gut of other tissues…….. 1. Conjugation of glutathion with the drug molecule through the sulfahydral Group of cysteine in the presence of glutathione-s-transeferase. Gly Glutathione-s-transferase Drug+GSH D-S-Cys Glutamyl Trans peptidase Gly D-S-Cys-NH2 Gln peptidase COOH N-Acetylase D-S-CH2-CH-NH-CO-CH3 COOH D-S-CH2-CH-NH2 2. Removal of glutamyl by glutamyl traspeptidase 3.Removal of glycine by peptidase. 4.N- acylation f the cysteine conjugate to form n acetylated cysteine. SULFATION • Conjugation with sulfate is common pathway for metabolism of phenols,but occur for alcohols,amines and thiols. • Sulfo transeferase is the enzyme involved in metabolism of sulphur METHYLATION o Methylation reactions mainly meant for endogenous substance. o High energy intermediate compound S-Adenosyl methionine (SAM) is required to form methyl conjugate. o Methylation leads to less polar products,which are not easily excreted from the body. ACETYLATION This reaction is common for aromatic amines and sulphonamide which requires a co-factor acetyl co enzyme A. It is obtained from the glycolysis pathway .This reaction occurs in kupffer cells,but not hepatocytes. It also occurs in reticuloendothelial cells of spleen,lung &gut. The acetylated product is usually less polar than parent drug.renal toxicity of sulphonamides can be attributed to precipitation of less polar acetylated sulphonamides. AMINOACID CONJGATION Amino acid conjugation is a special fprm of N- acylation.the usual amino acid in volved Glycine,glutamine,ornithine,arginine.and taurine Generally ornithine is the amino Conjugated reaction which predominantly occurs in ureotelic animals. The conversion of Benzoic acid to hippuric acid and salicylic acid are the examples of this metabolic pathway. FATTY ACID CONJUGATION The fatty acids involved in the conjugation reaction are stearic acid and palmitic acid. Microsomal enzymes of liver catalyse these reactions CONDENSATION REACTION These are not be enzymatic but purely chemical and have been found for amines and aldehydes. FACTORS EFFECTING DRUG METABOLISM The thereapeutic efficacy,toxicity and biological half life of drug depends upon the metabolic rate of the particular drug….the following are the Factors effecting drug metabolism……. 1.Physico chemical properties of drug 2.Chemical factors Induction of drug metabolising enzymes Inhibition of drug metabolising enzymes Environmental chemicals 3.Biological factors Strain difference Species diference Sex difference Age Diet Alterd physiological factors Pregnancy Hormonal imbalance Disease status Temporal factors Circadian rhythms Circannual rhythms PHYSICO CHEMICAL PROPERTIES OF DRUG Molecuar size shape,pka,acidity, basicity,lipophilicity, steric and electronic characteristicsof a drug influence its interaction with the active sites of the enzyme and biotrasnformation of the process in which it is subjected CHEMICAL FACTORS INDUCTION OF DRUG METBOLISING ENZYMES The phenomenon of increasing drug metabolic ability of the enzymes by several drugs and chemicals is called as enzyme induction,and the agents which bring about such effect are known as enzyme inducers PROPERTIES OF ENZYME INDUCERS: 1. They are lipophilic compounds. 2. They are substrate for the inducted enzyme system. 3. They have long elimination half life. MECHANISM INVOLVED IN ENZYME INDUCTION ARE: 1. Increase in both liver size and liver blood flow. 2. Increase in total µsomal protein content 3. Increase in stability of enzymes. 4. Increase in synthesis of CYT P 450. 5. Decreased degration of CTY P 450. 6. Proliferation of smooth endo plasmic reticulum. INDUCERS ARE OF 2 TYPES: phenobarbital type inducers poly-cyclic hydro carbon type inducers phenobarbital type inducers:several drugs and pesticides which incerase the rate of metaboism of a large no.of drugs.these type can increase the enzyme activity up to 4 times. EX: when phenobarbital and dicoumaral are co administered to avoid the failure of anti-coagulant therapy and the haemorragic crisis. poly-cyclic hydro carbon type inducers: such as 3-methyl cholanthrene &cigaret smoke which stimulates the metabolic rate of few drugs. Some drugs like carbamazipine,meprobamate,cyclophosphamide,rifampicin etc; stimulate their own metabolism…… the phenomena is called auto induction INHIBITION IF DRUG METABOLISING ENZYMES A decrease in the drug metabolising abilitty of an enzyme is called enzyme inhibition. 1. Direct inhibition a. Competitive inhibition b. Non competitive inhibition c. Product inhibition 2.Indirect inhibition a.Repression b. Altered physiology 1a.Competitive inhibition: When structurlly similar compounds compete for the same site on an enzyme.tis process is reversible,and can be overcome by high concentration of substrates. EX:metacholine inhibits metabolism of acetylcholine by competing with it for cholinesterase…. 2a.Non-competitive inhibition:when structurally unrelated agent interacts with the enzyme and prevents the metabolism of the drug. EX:lead,mercury,arsenic and orgophosphorous insecticides….. 1c. Product inhibition:when the metabolic product competes with the substrate for the same enzyme.the phenomenon is called aauto inhibition EX:certain specific inhibitors like xanthine oxidase inhibitors (allopurinol), MOA oxidase inhibitors(phenelzine) inhibits the enzyme activity directly. 2a. Repression:it is the decrease in enzyme content due to fall in the rate of enzyme synthesis. EX : Carbon tetra chloride,carbon disulphide,disulfiram. 2b.Altered physiology: due to nutritional deficiency or harmonal imbalance Enyme inhibitors and drugs effected by them inhibitors Drugs with decreased metabolism MOA inhibitors Barbiturates,tyramine Coumarins Phenytoin Allopurinol 6-mercaptopurine PAS Phenytoin,hexobarbital ENVIRONMENTAL CHEMICALS Several environmental influence the drug metabolising ability Haalogenated pesticides such as DDT and polycyclic aromatic Hydrocarbons contained in ciggarate smoke hav enzyme induction effect. organophosphate insecticides and heavy metals such as tin, Mercury, nickel,cobalt and arsenic inhibits drug metabolic ability of an enzyme BIOLOGICAL FACTORS SPECIES DIFFERENCE: species difference have been observed in both Phase -1 and phase-2 reactions. In phase-1 variations in enzyme and their activity have been observed Ex: metabolism of amphetamine and ephedrine,in men & rabbit they are predominantly metabolised by oxidative deamination where as in Rats the aromatic oxidation is major route. In phase-2 reactions,the variation is mainly due to complete lack of Certain conjugating enzymes. Ex: in pigs, phenol is excreted mainly as glucorunide where as its sulphares conjugates dominates in rats. Certain birds utilises ornithine fpr conjugating aromatic acids instead Of glycine. AGE In neonates(up to 2 months),the microsomal enzyme system is not fully developed and many drugs are bio-transformed slowly Ex: caffeine has half life of 4 days in sdults,but in neonates it rises Up to 4 days agent. Infants(between 2 months & one year) show almost a similar profile as neonates in metabolising drugs with improvement in the capacity as age advances and enzyme activity increases. chidren b\w 1 year &12 years and older infants metabolises several drugs much more rapid than adults as the rate of metabolism reaches to maximum level.as a result they require more dose than adults. In very elderly persons,liver size is reduced,due to decrease in microsomal enzyme activity,hepatic blood flow,cardiac output, of all of which contributes decreased metabolism of drug. DIET Low protein diet decreases and high protein diet increases the metabolising ability protein carbohydrate ratio in the diet is also important:a higgh ratio increases the microsomal mixed function oxidase activity. fat free diet depresses the CYT P 450 since phospholipids are important contents of microsomes. Dietary deficiency of vitamins & minerals may retard the metabolic activity of enzymes. Grape fruit inhibits metabolism of many drugs and improves their oral availability. starvation results in the decreased amount of glucorunides formed than under normal conditions . Malnutrition results in enhanced metabolism of sex harmones. Alcohol ingetion results in short term decrease followed by increase in enzyme activity ALTERED PYSIOLOGICAL FACTORS PREGNANCY: Studies in animals hav e shown the maternal drug metbolising ability is reduced during later stages of pregnancy.this was due to high levels of steroid harmones in circulation during pregnancy. HARMONAL IMBALANCE: Higher levels of one harmone may inhibit the activity of few enzymes while inducing that of others .adrenolectomy,thyroidectomy, alloxan-induced diabetes in animals showed impairment in the exzyme activity with a subsequent fall in the rate of meatabolism.a similar effect was observed in the pitutary growth harmone. DISEASE STATUS: Reduction in hepatic drug metabolising ability is apparent in conditions such as hepatic carcinoma,hepatits,cirrohsis,obstructive jaundice,etc;.congestive heart failure,myocardial infarction results in decrease in blood fllow to liver ,impaired metabolism of drugs having high hepatic extraction ratio. EX: Propanolol and lidocaine. TEMPORAL FACTORS CIRCADIAN RHYTHMS: Diurnal variations or variations in the Enzyme activity with light cycle is called as circadian rhythms in drug metabolism. It has been observed that the enzyme activity is maximum during early morning(6-9 a.m) and minimum at late afternoon(2-5 p.m) which was suggested to correspond with the high and low serum levels of corticosterone Study of variations in drug response as influenced by time is called as chronopharmacology Time dependent chnge in drug kinetics is known as chronokinetics REFERENCES 1. Text book of biopharmaceutics and pharmacokinetics by v.venkateswarulu, page no135-160. 2. Text book of biopharmaceutics and pharmacokinetics a treatise, page no139-193. 3. Bio-pharmacokinetics&clinical pharmacokinetics by milo gibaldi,3rd edition,pageno187-193 4. Encyclopedia of pharmaceutical technology by james swarbrick,3rd edition,volume-3. 5. Ppts downloaded from www.google.com