Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Immunocontraception wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Vaccination policy wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
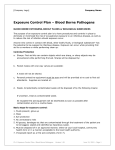
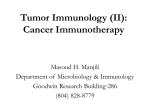
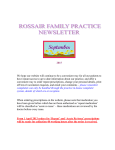
Clavreul et al. Autologous tumor cell vaccination plus infusion of GM-CSF by a programmable pump in the treatment of recurrent malignant gliomas Anne Clavreula, Nicole Piardb, Jean-Yves Tanguyc, Eric Gamelind, Marie-Christine Rousselete, Pierre Leyniad, Philippe Meneia a Département de Neurochirurgie, CHU, Angers, F-49933 France; INSERM U646, Angers, F-49100 France; UNAM, Angers, F-49100 France b c Département de Radiologie, CHU, Angers, F-49933 France d e EFS, Angers, F-49100 France Centre Paul Papin, CRLCC, Angers, F-49933 France Laboratoire Pathologie Cellulaire et Tissulaire, CHU, Angers, F-49933 France Corresponding author: Dr Anne Clavreul Département de Neurochirurgie CHU 49933 Angers, France Tel: +33 241 354822 Fax: +33 241 354508 E-mail: [email protected] This work was supported by a PHRC from National Health Department and a grant from the Ligue Départementale de Lutte contre le Cancer. 1 Clavreul et al. Abstract This phase I study reports on the safety and feasibility of autologous cell vaccination combined with infusion of GM-CSF by a programmable pump in the treatment of recurrent malignant gliomas. The trial enrolled nine patients who had previous surgery, radiation and were successfully weaned off steroids. Unfortunately, only five patients completed the protocol and were monitored for side effects, local reactions, delayedtype hypersensitivity (DTH) responses and survival. The treatment was well tolerated. Two patients developed DTH reactions after vaccination and three patients had an unusually long survival without any other treatment. Despite the small number of patients treated, this study is informative and encouraging. The programmable pump is a promising tool to infuse cytokines subcutaneously for vaccination purposes. Nevertheless, this study as others highlights also the specific difficulties encountered in such vaccination paradigms for the treatment of glioma. Key Words: GM-CSF, immunotherapy, malignant glioma, vaccination 2 Clavreul et al. 1. Introduction Malignant gliomas have a poor prognosis despite aggressive treatment using surgery, radiotherapy and chemotherapy 1, 2. One therapy emerging over the last few years is active immunotherapy to initiate T-cell-mediated antitumor immune responses 3, 4. This therapy offers several advantages such as tumor specificity with low side effects and a durable antitumor effect owing to the phenomenon of immunologic memory. Two main active immunotherapy strategies are used for glioma patients: peripheral injections of irradiated autologous tumor cells (ATC) along with an adjuvant for immune stimulation or vaccinations with autologous dendritic cells primed with tumor antigens ex vivo 3, 4. The use of irradiated ATC vaccines is considered an advantage, given the lack of knowledge regarding the relevant tumor associated antigens (TAAs) in glioma. Furthermore, injection of these irradiated ATC allows an antigenic treatment in vivo without manipulation of dendritic cells ex vivo. To render these ATC more immunogenic, different cytokines and chemokines have been used as immune adjuvants. One of the most frequently used cytokine is granulocyte-monocyte colonystimulating factor (GM-CSF) which is a potent activator of dendritic-cell antigen presentation, and participates in the initiation of danger signals needed to activate the immune system, break tolerance, and develop an antitumor immune response 5. Several preliminary studies using ATC plus GM-CSF alone showed promising results in brain tumors 6-12. To date, in clinical studies, administration of GM-CSF to the vaccination site is achieved principally by ATC, allogeneic tumor cells or even normal bystander cells, genetically modified to express GM-CSF 13-17. This approach allows a prolonged GM-SF delivery but is time and labor consuming 14. Furthermore, the safety of this method still needs to be addressed. Another GM-CSF delivery approach consists in the 3 Clavreul et al. use of pump which allows a continuous infusion of the cytokine with a good safety profile 9, 18, 19. This clinical trial was therefore designed to investigate the safety and feasibility of vaccination with ATC and infusion of GM-CSF by a programmable pump in the treatment of recurrent malignant gliomas. 2. Materials and Methods 2.1. Patient eligibility This trial was an open, nonrandomized phase-I study. The protocol was approved by the Committee on the Right of Human Subjects and the biotherapy department of French Health Products Safety Agency. All patients provided informed consent before treatment. Inclusion criteria were patients presenting a recurrent grade III or IV malignant glioma that was amenable to surgical resection, an age between 18 and 68 years, a Karnofsky index (KI) > 60. Patients must have been previously treated by conventional radiotherapy (60 Gy) and tapered off steroids and cytotoxic drugs for at least one month at the time of vaccination. Exclusion criteria included pregnancy, severe pulmonary, cardiac or other systemic diseases. 2.2. Assessment of extent of tumor resection before vaccination In the 72 h following the surgery, a MRI was performed including T1 with and without gadolinium, T2 and Fluid Attenuated Inversion Recovery (FLAIR) weighted sequences. The extent of resection was defined as biopsy (less than 10% resected), sub-total resection (10% to 90% resected) and gross-total resection (more than 90% resected). The resection volume has been calculated on MRI slices. 2.3. Autologous tumor culture 4 Clavreul et al. After surgery, tumor tissue was mechanically disaggregated into a suspension and then passed through nylon meshes of decreasing pore size. The cell suspension was cultured in Dulbecco’s modified Eagle’s medium (DMEM) (Lonza, Verviers, Belgium) supplemented with 10% human AB serum or FCS (Hyclone, PerbioScience, Bredières, France) and 1% penicillin/streptomycin (Lonza). Following in vitro expansion, cells were irradiated at 45 Gy using a 137Cs source (EFS, Angers, France), checked for viability by trypan blue exclusion and stored at -80°C. Prior to inoculation, culture media were tested for bacterial contamination. 2.4. Tumor vaccine preparation On the day of vaccination, the cells were thawed, washed two times with physiological serum and counted. Between 2 to 5106 ATC in 600 µl of physiologic serum were injected subcutaneously. 2.5. GM-CSF infusion RhGM-CSF (Leucomax®, Novartis, Schering-Plough, Levallois Perret, France or Leukine®, Berlex, Seattle, United States) was infused at the site of cell inoculation. The infusion was performed using a programmable pump MiniMed 407C and standard insulin infusion sets, Sof-Set (Medtronic MiniMed, Northridge, United States). Reservoirs containing GM-CSF were changed weekly and the remaining GM-CSF was quantified by ELISA (R&D Systems, Lille, France). 2.6. Vaccination shedule Two sets of vaccination protocols have been performed (Figure 1). Protocol 1 consisted in four subcutaneous vaccinations with ATC every 7 days in abdomen and a continuous infusion of GM-CSF (10 µg/24 h) during 28 days. Protocol 2 was composed of four subcutaneous vaccinations with ATC every 21 days close to cervical lymph nodes and 5 Clavreul et al. an infusion of GM-CSF (20 µg/24 h) 3 days before and during 14 days after each vaccination. 2.7. Evaluation of clinical status Patients were followed by clinical and MRI examination and blood cell counting (BCC). Toxicity was monitored using the National Cancer Institute Common Toxicity Criteria. Response to the treatment was analyzed using Mac Donald criteria 20: complete response (total disappearance of all enhancing tumor, patient stable or improved), partial response (50% or greater reduction in size, patient stable or improved), stable (reduction of 050% in tumor size, patient stable or improved), progressive disease (25% or greater increase in size or any new tumor, or patient worse). 2.8. Delayed-type hypersensitivity reaction Delayed type hypersensitivity (DTH) was tested before and after the final vaccination. For this, an intradermal ATC inoculation (1106 cells) was performed in the shoulder, followed by a cutaneous punch biopsy 48 h later. Formalin-fixed, paraffin-embedded sections of the cutaneous samples were stained with hematoxylin-phloxin-saffron and studied by immunohistochemistry for astrocyte-, T-, B-, monocyte-macrophage-, Langerhans cell-, and NK cell-differentiation antigens using a streptavidin-biotin peroxidase method on a DAKO automatic immunostaining device. The specificity and source of the antibodies are listed in Table 1. 2.9. Autoimmunity detection Sera of patients were collected before and after the treatment to determine if autoimmunity develops against myelin. Autoantibodies directed against myelin associated glycoprotein (MAG) were quantified by ELISA according to the manufacturer’s instructions (Bühlmann, Mulhouse, France). 6 Clavreul et al. 2.10. Statistical analysis The prevaccination and postvaccination data were compared using the Student’s t-test modified for small samples. Statistical significance was determined at P < 0.05 level. 3. Results 3.1. Patient characteristics Nine patients were enrolled in this phase I trial between 2001 and 2005, seven in Protocol 1 and two in Protocol 2. Their characteristics are summarized in Table 2. They were four women and five men with an age range from 33 to 65 years (mean 49.9 years). All patients have been previously treated by radiotherapy, six by chemotherapy. Histopathological diagnosis made after second surgery was the same as the one made after the initial surgery: glioblastoma (n=6), anaplastic oligodendroglioma (n=2) and anaplastic oligoastrocytoma (n=1). The extent of resection was a sub-total resection for six patients and a gross-total resection for three patients (Table 2). 3.2. Vaccine preparation Preparation of irradiated tumor cells was initiated after a mean interval of 4.5 weeks (1.4 to 9 weeks) after surgery and the cell viability was consistently 80-90% before freezing. For 6/9 patients, cell yields were not sufficient to allow four vaccinations. 3.3. Vaccine administration Among the nine patients enrolled in this trial, four have not been vaccinated. Three patients (n°3, n°6 and n°9) because tumors have progressed and clinical status worsened during the time of the tumor cell culture and one patient (n°7) because the Health Agency has suspended the utilization of the human serum produced by our first supplier, a biotechnology company. Among the four patients treated in Protocol 1, three 7 Clavreul et al. received two vaccinations (patients n°1, n°4 and n°5) and one three vaccinations (patient n°2) (Table 2). The patient n°8 treated in Protocol 2 received four vaccinations. Between 2 to 5106 ATC (mean 3.0106 1.1106) were inoculated for vaccination. 3.4. GM-CSF infusion A dose of 10 µg/24 h (Protocol 1) or 20 µg/24 h (Protocol 2) was administrated to vaccinated patients. The infusion device was well tolerated. GM-CSF in the pump reservoir was changed every week and the stability of the cytokine was analyzed by ELISA. For patients receiving a dose of 10 µg/24 h, the initial concentration of GMCSF in the reservoir was 30 µg/ml and after 7 days, the remaining concentration of GMCSF was 26.5 3.2 µg/ml. 3.5. Safety The two serious adverse effects reported were due to the surgery, one hemiplegia of vascular origin (patient n°4) and one post operative hematoma necessitating a reintervention (patient n°7). The others side effects observed during the treatment were minor and can be attributed to GM-CSF: vomiting (n=1), asthenia (n=1), astheniaanorexia-arthralgia (n=1), episode of shivering, cyanosis, low blood pressure, vomiting, fever, 15 min after the first DTH (n=1). An increase of peripheral blood eosinophils was observed in the four patients treated in Protocol 1 (1.18% 0.12% before vaccination to 6.53% 1.64% three weeks after the first vaccination; P < 0.05). This increase was also noticed in the patient treated in Protocol 2 but in a less important manner. No cutaneous complication was observed at the inoculation site. There was no evidence of growth of tumor cells at the vaccine site in any patient. No sign of leucoencephalopathy (clinical or on the MRI-FLAIR sequence) was detected, nor autoantibodies against MAG. 3.6. Response to immunization 8 Clavreul et al. Between 0.6 to 1.6106 ATC (mean 1.1106 0.4106) were inoculated for DTH before and after the vaccination schedule. No patients developed local DTH reactions before vaccination. Punch biopsies showed a normal epidermis and, in the superficial dermis, a mild perivascular accumulation of T lymphocytes, mostly CD4 positive, with rare Langerhans cells and no or exceptional B lymphocytes. In the reticular dermis, rare neutrophils were observed close to a few glial cells in patients n°1 and n°2. In patients n°4, n°5 and n°8, some glial cells and GFAP positive fragments were embedded in a larger inflammatory reaction composed of macrophages and polymorphonuclear leukocytes (mostly neutrophils and a few eosinophils) with some leukocytoclasis. There were no NK cells. After vaccination, the punch biopsy of two patients (n°5 and n°8) showed an increase of perivascular T cells and Langerhans cells in the superficial dermis compatible with a DTH reaction (Figure 2). Other patients did not develop cellular infiltrates characteristic of DTH despite the fact that a small induration (5 mm) with erythema developed to the site of the inoculation for patient n°4. 3.7. Clinical response Clinical responses are detailed in Table 2 and in Figure 3. Three patients (n°4, n°5 and n°8) were clinically stable after vaccination. They presented an unusually long survival, respectively 62, 42 and 88 weeks after the second surgery without corticoids and adjuvant treatments. The two other patients (n°1 and n°2) had a progressive disease after vaccination. 4. Discussion This phase I study was designed to investigate the safety and feasibility of vaccination using irradiated ATC and infusion of GM-CSF in patients with recurrent malignant 9 Clavreul et al. glioma. While the concept of this trial is quite similar in many ways to previous studies, the novel aspect of this study was the use of programmable pump with standard insulin infusion sets to deliver GM-CSF at the vaccination inoculation site. This infusion technology allows a sustained subcutaneous delivery in a flow as small as 1 µl/h. The principal concern with this technology was the instability of GM-CSF and the possibility of its degradation in the reservoir at room temperature. For this reason, reservoirs were changed every week. Interestingly, in this study, after 7 days at room temperature, GM-CSF showed a satisfactory stability. Furthermore, GM-CSF administration induced an increase of peripheral blood eosinophils. This hyper eosinophilia has been already described after subcutaneous administration of low doses of GM-CSF (as 7.5 to 45 µg/day for 10 days) 21. These results indicate that programmable pump could ensure the release of a biologically active GM-CSF during vaccination avoiding the use of ATC retrovirally transduced with GM-CSF which is time and labor consuming 14. This clinical trial was originally designed to enroll fifteen patients. However, we closed the trial after nine patients due to the unavailability of GM-CSF and the difficulty to enclose patients tapered off steroids. Unfortunately, among the nine patients enrolled, only five patients completed the protocol because in others patients, tumors had progressed and clinical status worsened during the time of the tumor cell culture. This small number of patients does not allow drawing conclusions about the safety and clinical response of vaccination with ATC and infusion of GM-CSF by pump. Furthermore, we could not comment meaningfully on the efficacy between the Protocol 1 and 2. Nevertheless, three treated patients (patients n°4, n°5 and n°8) had an unusually long survival without any other treatment (respectively 61, 42 and 88 weeks after the 10 Clavreul et al. second surgery). Mean survival in glioblastoma after recurrence is 23 weeks after surgery alone and 31 weeks after surgery plus local chemotherapy 22. Interestingly, these three patients developed a larger inflammatory reaction at their first DTH site and had a moderate size of the recurrence at the time of vaccination. Furthermore, two of these three patients (n°5 and n°8) showed a histological DTH reaction after vaccination suggesting the development of a peripheral antitumor immune response. The two other treated patients (n°1 and n°2) did not show prolong survival nor the development of an immune reaction after vaccination. However, it is important to note that patient n°1 was vaccinated despite a low KI and an important tumor recurrence. Patient n°2 was vaccinated although its MRI showed, at the time of the first vaccination, a recurrence at distance of the surgical cavity. If these results are encouraging, they point out several issues linked to the methodology of vaccination against glioma. Firstly, the difficulty of re-intervention, especially when the goal is to perform a sub-total resection. Two reported serious adverse effects were due to this second surgery. Unfortunately, the resection is necessary since extent of disease at enrollment seems to correlate strongly with poor response to active immunotherapy 14, 23 . Secondly, this study, as others, shows the difficulty to rapidly and reliably obtain sufficient ATC for vaccination 14, 24, 25. In our study, a mean interval of 4.5 weeks was necessary to prepare irradiated tumor cells after surgery. The use of cultured ATC as vaccines seemed to us a good compromise since no glioma-specific, immunologic-relevant TAAs have been identified. While there is a lot of evidence in the literature that tissue culture conditions change the phenotype of tumors, we showed in a previous study that our culture conditions preserved at early passage cultures the cell population of interest present in the original tumor and TAA expression 26. However, it 11 Clavreul et al. is clear that efforts should be made to obtain sufficient cell number in a relatively short period of time to avoid large recurrence. To increase the cell yield, some clinical studies used frozen tumor digest or formalin-fixed tumor tissue for vaccination with no cultured cells 6, 27, 28. However, these preparations contain tumor cells but also normal cells which could induce autoimmunity after their injection. Besides, the induction of lethal experimental allergic encephalomyelitis has been described in primates and guinea pigs after vaccination with human glioblastoma tissue 29. In our study, we do not have noticed demyelination with MRI-FLAIR sequence, which is considered the most sensible sequence to show demyelination within the white matter of the cerebral hemispheres 30, nor autoantibodies directed against MAG in sera of patients. Another alternative to solve the problem of time-consuming ATC expansion is the use of synthetic glioma peptides or allogeneic tumor cells as vaccines 31-34. Finally, despite the high number of active immunotherapy clinical trials conducted in malignant gliomas, there is still a lack of definite proof for efficacy 3. In fact, this clinical trial as others shows that induction of a peripheral antitumor immune response is possible in glioma patients but not sufficient to preclude disease progression. Several studies point out the importance of the immunosuppressive tumor microenvironment in the glioma immunotherapy resistance 3, 19, 35. Counteracting this immunosuppressive tumor microenvironment is essential in the success of the future anti-glioma vaccines. Acknowledgments: We are grateful to Medtronic Minimed, Northridge, United States, for the kind gift of pumps and infusion sets. We thank the Laboratory of Cellular Biology (Prof A. Barthelaix/L. Denéchaud), the Laboratory of Bacteriology (Prof F. Lunel-Fabiani) and the Laboratory of Hematology (Prof M. Zandecki/Dr F. Genevieve), 12 Clavreul et al. CHU, Angers, France, for technical assistance. We also thank the members of the Clinical Trial Department, Cancer Center Paul Papin, Angers, France, for the facilities provided. 13 Clavreul et al. References 1. Westphal M, Hilt DC, Bortey E, et al. A phase 3 trial of local chemotherapy with biodegradable carmustine (BCNU) wafers (Gliadel wafers) in patients with primary malignant glioma. Neuro Oncol 2003;5:79-88. 2. Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987-96. 3. Okada H, Kohanbash G, Zhu X, et al. Immunotherapeutic approaches for glioma. Crit Rev Immunol 2009;29:1-42. 4. Yamanaka R. Dendritic-cell- and peptide-based vaccination strategies for glioma. Neurosurg Rev 2009;32:265-73; discussion 73. 5. Chang DZ, Lomazow W, Joy Somberg C, et al. Granulocyte-macrophage colony stimulating factor: an adjuvant for cancer vaccines. Hematology 2004;9:207-15. 6. Plautz GE, Barnett GH, Miller DW, et al. Systemic T cell adoptive immunotherapy of malignant gliomas. J Neurosurg 1998;89:42-51. 7. Plautz GE, Miller DW, Barnett GH, et al. T cell adoptive immunotherapy of newly diagnosed gliomas. Clin Cancer Res 2000;6:2209-18. 8. Lefranc F, Cool V, Velu T, et al. Granulocyte macrophage-colony stimulating factor gene transfer to induce a protective anti-tumoral immune response against the 9L rat gliosarcoma model. Int J Oncol 2002;20:1077-85. 9. Wallenfriedman MA, Conrad JA, DelaBarre L, et al. Effects of continuous localized infusion of granulocyte-macrophage colony-stimulating factor and inoculations of irradiated glioma cells on tumor regression. J Neurosurg 1999;90:1064-71. 14 Clavreul et al. 10. Yu JS, Burwick JA, Dranoff G, et al. Gene therapy for metastatic brain tumors by vaccination with granulocyte-macrophage colony-stimulating factor-transduced tumor cells. Hum Gene Ther 1997;8:1065-72. 11. Herrlinger U, Kramm CM, Johnston KM, et al. Vaccination for experimental gliomas using GM-CSF-transduced glioma cells. Cancer Gene Ther 1997;4:345-52. 12. Sloan AE, Dansey R, Zamorano L, et al. Adoptive immunotherapy in patients with recurrent malignant glioma: preliminary results of using autologous whole-tumor vaccine plus granulocyte-macrophage colony-stimulating factor and adoptive transfer of anti-CD3-activated lymphocytes. Neurosurg Focus 2000;9:e9. 13. Ward JE, McNeel DG. GVAX: an allogeneic, whole-cell, GM-CSF-secreting cellular immunotherapy for the treatment of prostate cancer. Expert Opin Biol Ther 2007;7:1893-902. 14. Parney IF, Chang LJ, Farr-Jones MA, et al. Technical hurdles in a pilot clinical trial of combined B7-2 and GM-CSF immunogene therapy for glioblastomas and melanomas. J Neurooncol 2006. 15. Soiffer R, Hodi FS, Haluska F, et al. Vaccination with irradiated, autologous melanoma cells engineered to secrete granulocyte-macrophage colony-stimulating factor by adenoviral-mediated gene transfer augments antitumor immunity in patients with metastatic melanoma. J Clin Oncol 2003;21:3343-50. 16. Luiten RM, Kueter EW, Mooi W, et al. Immunogenicity, including vitiligo, and feasibility of vaccination with autologous GM-CSF-transduced tumor cells in metastatic melanoma patients. J Clin Oncol 2005;23:8978-91. 15 Clavreul et al. 17. Borrello I, Sotomayor EM, Cooke S, et al. A universal granulocyte-macrophage colony-stimulating factor-producing bystander cell line for use in the formulation of autologous tumor cell-based vaccines. Hum Gene Ther 1999;10:1983-91. 18. Jean WC, Spellman SR, Wallenfriedman MA, et al. Effects of combined granulocyte-macrophage colony-stimulating factor (GM-CSF), interleukin-2, and interleukin-12 based immunotherapy against intracranial glioma in the rat. J Neurooncol 2004;66:39-49. 19. Clavreul A, Delhaye M, Jadaud E, et al. Effects of syngeneic cellular vaccinations alone or in combination with GM-CSF on the weakly immunogenic F98 glioma model. J Neurooncol 2006;79:9-17. 20. Macdonald DR, Cascino TL, Schold SC, Jr., et al. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol 1990;8:1277-80. 21. Kaplan G, Walsh G, Guido LS, et al. Novel responses of human skin to intradermal recombinant granulocyte/macrophage-colony-stimulating factor: Langerhans cell recruitment, keratinocyte growth, and enhanced wound healing. J Exp Med 1992;175:1717-28. 22. Brem H, Piantadosi S, Burger PC, et al. Placebo-controlled trial of safety and efficacy of intraoperative controlled delivery by biodegradable polymers of chemotherapy for recurrent gliomas. The Polymer-brain Tumor Treatment Group. Lancet 1995;345:1008-12. 23. De Vleeschouwer S, Fieuws S, Rutkowski S, et al. Postoperative adjuvant dendritic cell-based immunotherapy in patients with relapsed glioblastoma multiforme. Clin Cancer Res 2008;14:3098-104. 16 Clavreul et al. 24. Kikuchi T, Akasaki Y, Irie M, et al. Results of a phase I clinical trial of vaccination of glioma patients with fusions of dendritic and glioma cells. Cancer Immunol Immunother 2001;50:337-44. 25. Schneider T, Gerhards R, Kirches E, et al. Preliminary results of active specific immunization with modified tumor cell vaccine in glioblastoma multiforme. J Neurooncol 2001;53:39-46. 26. Clavreul A, Jean I, Preisser L, et al. Human glioma cell culture: two FCS-free media could be recommended for clinical use in immunotherapy. In Vitro Cell Dev Biol Anim 2009. 27. Wood GW, Holladay FP, Turner T, et al. A pilot study of autologous cancer cell vaccination and cellular immunotherapy using anti-CD3 stimulated lymphocytes in patients with recurrent grade III/IV astrocytoma. J Neurooncol 2000;48:113-20. 28. Ishikawa E, Tsuboi K, Yamamoto T, et al. Clinical trial of autologous formalinfixed tumor vaccine for glioblastoma multiforme patients. Cancer Sci 2007;98:1226-33. 29. Bigner DD, Pitts OM, Wikstrand CJ. Induction of lethal experimental allergic encephalomyelitis in nonhuman primates and guinea pigs with human glioblastoma multiforme tissue. J Neurosurg 1981;55:32-42. 30. Fazekas F, Barkhof F, Filippi M, et al. The contribution of magnetic resonance imaging to the diagnosis of multiple sclerosis. Neurology 1999;53:448-56. 31. Yajima N, Yamanaka R, Mine T, et al. Immunologic evaluation of personalized peptide vaccination for patients with advanced malignant glioma. Clin Cancer Res 2005;11:5900-11. 17 Clavreul et al. 32. Izumoto S, Tsuboi A, Oka Y, et al. Phase II clinical trial of Wilms tumor 1 peptide vaccination for patients with recurrent glioblastoma multiforme. J Neurosurg 2008;108:963-71. 33. Stathopoulos A, Samuelson C, Milbouw G, et al. Therapeutic vaccination against malignant gliomas based on allorecognition and syngeneic tumor antigens: proof of principle in two strains of rat. Vaccine 2008;26:1764-72. 34. Mahaley MS, Jr., Bigner DD, Dudka LF, et al. Immunobiology of primary intracranial tumors. Part 7: Active immunization of patients with anaplastic human glioma cells: a pilot study. J Neurosurg 1983;59:201-7. 35. Liau LM, Prins RM, Kiertscher SM, et al. Dendritic cell vaccination in glioblastoma patients induces systemic and intracranial T-cell responses modulated by the local central nervous system tumor microenvironment. Clin Cancer Res 2005;11:5515-25. 18 Clavreul et al. Legends of figures Figure 1: Vaccination schedules. Figure 2: Cutaneous biopsy before vaccination in patient n°5 showed a mild perisvascular lymphocytic infiltration in the superficial dermis (A, original magnification 200) and only rare CD1a positive Langerhans cells (B, original magnification 400). After vaccination, there was an increase in perivascular T lymphocytes (C, original magnification 200) and in CD1a positive Langerhans cells (D, original magnification 400). Figure 3: MRI from patients n°1, n°2, n°4, n°5 and n°8, before surgery (A, D, H, L, P), 24 h after surgery (B, E, I, M, Q), 24 h before the first vaccination (C, F, J, N, R) and 8 weeks after the final vaccination (G, K, O, S). 19