Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
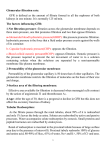
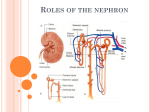
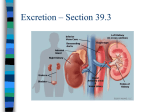
glomerulus is excreted in the urine. The most obvious element following this pattern is water (Fig. 7-2c). 7. URINE FORMATION In order to form urine the kidneys have to carry out three processes: glomerular filtration, tubular reabsorption and finally tubular secretion (Fig. 7-1). The last pattern consist in filtering a determined quantity in the glomerulus and then further have a net addition to the filtrate by tubular secretion of the same element, thus more Urine formation • Filtration –Crossing of filtration membrane –Formation of filtrate Glomerular filtration • Tubular reabsorption Tubular secretion –Solutes and water cross from filtrate into interstitial fluid and peritubular capillaries • Tubular secretion –Solutes are secreted into filtrate Tubular reabsorption • Filtrate = Urine Figure 7-1. General processes involved in the formation of urine The addition of the effects of each portion determines the composition and concentration of the urine. Different substances reach urine through different routes within this general pattern of filtration, reabsorption and secretion. Some materials are filtered in the glomerulus and are not reabsorbed at all in the tubules, thus, all what is filtered is excreted in urine. Understandable, since these products are not required by the organism, most waste, toxic materials follow this pattern of secretion (Fig. 7-2a). The opposite situation takes place with substances which are filtered in the glomerulus are shortly after reabsorbed in their entirety through the tubules, thus, urine under normal conditions does not carry any of these elements. Glucose, amino acids and small proteins follow this pattern of circulation (Fig. 7-2 b). of what was originally filtered appears in the urine (Fig. 72d). A C B D Figure 7-2. Alternative paths taken by different substances in the kidney. A =waste, B=glucose, aa, small prot., C=water, D= ions. Two other patterns of secretion can be identified in the nephrons. Some substances are filtered in the glomerulus but some portion of it is reabsorbed in the tubular component, thus, less of what is initially filtrated in the V BS 122 Physiology II 47 Class of 2013 Use of inulin to calculate GFR GLOMERULAR FILTRATION The initial filtrate is formed in the renal capsule and consists in the passage of a large proportion of all the component of plasma, from the circulation to the tubular structure of the kidney. Here the filtration barrier selectively permits the passage of water, solutes (electrolytes), amino acids, glucose, waste products and some small proteins, therefore the concentration of most components of the filtrate are almost identical to that of the plasma left in the capillaries. Large proteins, cellular components and cells are retained within the capillaries and do not enter the filtrate. Some material such as fatty acids, steroids and calcium can be partially retained in the capillaries because a fraction may be bound to proteins. The rate at which the filtrate is formed is called the glomerular filtration rate (GFR) (Fig. 7-3). To be able to determine the GFR we have to be able to determine the clearance of a substance that behaves as water in the glomerulus. The most common is to inject the plasma with inulin. Inulin is a natural polysaccharide synthesized by many plants (Fig 7-4). • • • • Natural polysaccharide Produced in plants Fibre (fructan) 5200 D MW • Filters completely • Not reabsorbed or secreted Figure 7-4. Characteristics of Inulin It is a type of fibre classified as a fructan with a molecular weight of 5200 daltons. Inulin has the special characteristic that the kidney is capable of completely filter it in the glomerulus but it does not get reabsorbed or secreted by the tubules. For the purposes of estimating GFR inulin behaves like water in the glomerulus. Therefore, once injected in the plasma its rate of excretion is directly proportional to the rate of filtration of water and solutes across the filtration barrier. Figure 7-3. Glomerular filtration rate Replacing plasma and urinary concentration of inulin and the urinary flow rate in the above equation we can calculate GFR (Fig. 7-5). HOW TO CALCULATE OR ESTIMATE GFR There are several techniques to measure or closely estimate the GFR. Renal clearance rate of a substance (Cs) can be established if we know the volume of urine being produced (V), the concentration of the substance in the urine (Us) and the concentration of the substance in the plasma (Ps). Plasma concentration of inulin (Pinu) = 0.1µmol/mL Urinary concentration of inulin (Uinu) = 6µmol/mL Urinary flow rate (V) = 2 mL/ min Then GFR= C inu = V x Uinu/ Pinu = 2 x 6/0.1 = 120 mL/min Cs= Us x V / Ps V BS 122 Physiology II 48 Class of 2013 Use of PAH to estimate renal plasma flow Para-aminohippuric acid (PAH), a product of aromatic amino acid metabolism can be used to estimate Renal Plasma Flow (RPF). When a substance is completely cleared from the plasma, then the clearance rate of such substance is equivalent to the total renal plasma flow. Such a substance does not exist but about 90 % of the PAH is excreted. That means in the average normal kidney the extraction rate of PAH is 90 % (Fig. 7-7). • Plasma inulin (PInu) = 0.1 µmol/mL • Urinary inulin (UInu) = 6 µmol/mL • Urinary flow rate (V) = 2 mL/min GFR = CInu = V x UInu/ PInu = 2 x 6/ 0.1= 120 mL/min Figure 7-5. Estimating GFR using inulin Use of creatinine to estimate GFR Muscle metabolism generates a waste by-product called creatinine (Fig. 7-6). This compound can be used to estimate GFR. Unlike inulin, creatinine does not have to be injected, thus makes the estimation techniques simpler. Creatinine clears in the glomeulus as water but the tubules also secret a small amount of creatinine into the filtrate, generating an overestimation of the amount cleared. Fortunately, there is also a similar overestimation in the technique to measure creatinine, thus, the combination of these two errors tend to balance out. • • • • • • • • Product of aromatic AA metabolism • Used to estimate RPF • 90 % is filtered in in kidney Figure 7-7. Characteristics of PAH Remember that ideally, if a compound is totally cleared from the plasma, the clearance rate of that compound would be equal to the total amount of that compound in the RPF. What gets in the kidneys (RPF x Ps) is the same quantity that is eliminated in the urine (Us x V) (Fig. 7-8). RPF = Us x V / Ps= Cs Protein metabolism waste product Fairly constant Does not require injection Clears glomerulus as water Tubules secrete small amount Technique to measure overestimate it They balance out But, since the extraction rate is only 90 % then Clearance of PAH/ Extraction rate of PAH RPF= And the extraction rate of PAH (EPAH) is the difference between the amount of PAH in the renal artery (APAH) and the amount left in the renal venous return (VPAH) divided by the concentration of PAH in the renal artery. EPAH = APAH- VPAH /APAH Figure 7-6. Estimating GFR using inulin For example an animal with the following values: (Fig. 7-9) V BS 122 Physiology II 49 Class of 2013 Furthermore, once we know the plasma flow rate, by knowing the blood hematocrit value we can determine the total blood flow through the kidney. If we measured hematocrit value is 0.45 then the total plasma flow would be 430 / (1 – 0.45) or 782 mL/min Volume of plasma flowing through the kidneys per minute RPF = Us x V/Ps = Cs Filtration fraction • Since PAH extraction rate = 90% • RPF = CPAH / EPAH Of all the plasma that circulates through the glomerulus about 19% is filtered into the tubular compartment. The exact amount at any given time is determined by several physiological factors. The hydrostatic and colloidal osmotic forces across the filtration barrier and the capillary filtration coefficient, which is in turn determined by the permeability and the surface area of the capillaries, determine the GFR. and • EPAH = APAH – VPAH / APAH Figure 7-8. Characteristics of PAH The volume of filtrate formed or filtrate fraction is = GFR x renal plasma flow. The components of the filtration barrier all contribute to determine the filtering capacity of this structure (Fig. 7-10). The fenestrations in the endothelial cells of the glomerular capillaries are large enough to permit the passage of all materials in blood except very large proteins and cells such as erythrocytes. The endothelial cells are, however, are densely loaded with negatively charged components. PPAH = 0.015 mg/mL UPAH = 5.8 mg/mL V = 1 mL/min RPF = Us x V/Ps = Cs • CPAH = 5.8 mg/mL x 1 mL/min 0.015 mg/mL = 387 mL/min = 430 mL/min 0.9 Figure 7-9. Estimating renal plasma flow Plasma concentration PAH of 0.015 mg/mL. Urinary concentration of PAH of 5.8 mg /mL Urinary flow rate of 1 mL/min The clearance of PAH in urine would be 5.8 mg/mL x 1 mL/min divided by the plasma concentration of PAH or 0.015 mg/mL= 387mL/min. If the extraction rate of PAH is 90% then the real plasma flow rate (PFR) can be determined by dividing 387 mL/min by 0.9 which would yield 430 mL/min. V BS 122 Physiology II 50 • Maximum size allowed through 7µm or 40 kD • Most proteins, cell components and cells are retained in capillaries • Small protein hormones cross • Protein bound FA and steroids are retained • Filtrate may contain 0.03% protein Figure 7-10. Characteristics of the filtration barrier This feature prevents the passage or filtration of many smaller proteins that would comfortably fit through the fenestrations. Class of 2013 The composition of the basement membrane determines its filtering capacity. This membrane is primarily made of proteoglycans and collagen chains interlocked, leaving large spaces through which most solutes and water can filter. Proteoglycans are charged with strong negative charges, thus preventing the passage of most proteins that could have crossed the fenestrations. The interdigtation of their extension create a series of filtration slits which further contribute to the filtration process. These elements are also charged negatively, thus further preventing the passage of proteins. If the filtration barrier is normal, this permits the passage of molecules smaller than 7µm in diameter or with a molecular mass of about 40,000 daltons (Fig. 7-10). Because most proteins are larger than these they are unable to be filtered out and they remain within the capillaries. Some proteins are, however, smaller than these thus, they cross the filtration membrane. Many protein hormones fall in this category. It is estimated that the filtrate can have about 0.03% of proteins in the glomerular space. Proteins are nonetheless, actively reabsorbed in the proximal convoluted tubule to the point that very little protein ever reach the urine. The last component of the filtration barrier is the layer of specialized epithelial cell that lay on top of the basement membrane, the podocytes (Fig. 6-11). For example an 80 kg hog under resting conditions will have a cardiac output (CO) of approximately 5.7L/min. As stated earlier the kidney receives approximately 20% of the volume of the CO so, in our case, the kidneys would be irrigated by about 1.14 L of blood/min that is the Renal Blood Flow (Fig 7-12). Volume of blood flowing through the kidneys per minute Cardiac output x % entering kidneys • • • • 80kg hog CO = 5.7L/min Renal fraction 20% RBF = 5.7 L/min x 0.2 = 1.14 L/min Figure 7-12. Calculation of renal blood flow How much urine is formed? Renal Blood Flow= CO X % Renal fraction To understand the process of urine formation is necessary to understand all the intermediary steps between blood moving through the circulatory system and the total amount of urine excreted by an animal. There are several concepts (Fig. 7-11) which will be explained with a mathematical example. RBF = 5.7 L/min X 0.2 = 1.14 L/min Of the volume of blood entering the kidney, only certain percentage is plasma. The rest is made up principally by hematocrites. Although these values can vary tremendously a standard percentage for a normal animal is 60% plasma (Fig 7-13). Renal Plasma Flow = RBF X % of plasma in blood RPF= 1.14 L/min X 0.6 = 0.684 L/min or 684 mL/min Of the plasma which enters the kidneys only about 19% goes through the filtration barrier. The rest leaves the glomerulus through the efferent arteriole with all the hematocrits and large proteins (Fig. 7-13). • Renal blood flow • Renal plasma flow • Glomerular filtration rate • Urine • Daily urine volume Glomerular Filtration Rate = RPF X % filtration fraction GFR = 684 mL/min X 0.19 = 130 mL of filtrate/min Of the volume that enters the capsular space only a very small fraction is excreted in urine, the rest is all reabsorbed Figure 7-11. Renal flow rates between circulation and urine V BS 122 Physiology II 51 Class of 2013 at different places in the nephron. The average volume which is not reabsorbed under normal conditions is onlyabout 0.8% of the filtrate (Fig. 7-14). Volume of no reabsorbed filtrate leaving the kidney per minute GFR x % no reabsorbed filtrate Volume of plasma flowing through the kidneys per minute • GFR =130 mL/min • Non reabsorbed filtrate (NRF) = 0.8% • Urine = 130 mL x 0.008 = 1.04 mL/min Renal blood flow x % plasma (blood-hematocrit) • RBF = 1.14 L/min • % plasma in blood = 60% • RPF = 1.14 L/min x 0.6 = 0.684 L/min = 684 mL/min Figure 7-15. Rate of urine formation Figure 7-13. Calculation of renal plasma flow • Urine = 1.04 mL/min • Day = 60 min x 24 h= 1440 min/day • L = 1000 mL • Daily volume urine = urine x min / 1000 Volume of plasma (filtrate) entering Bowman’s capsule per minute • Volume of urine = 1.04 mL/min x 1.44 = 1.49 L/Day Renal plasma flow x plasma entering the renal capsule • RPF = 684 mL/min • Filtration fraction (FF) = 19% • GFR = 684 mL/min x 0.19 = 130 mL /min Figure 7-16. Calculation of daily urine production volume Figure 7-14. Calculation of glomerular filtration rate Urine = GFR X % no reabsorbed filtrate Urine = 130 m L/min X 0.008 = 1.04 mL/min (Fig. 7-15). This volume per minute can be converted to L/day by multiplying by 1.44 (Number of minutes in one day/1000 mL) (Fig 7-16). Thus, this animal produces 1.04 mL/min X 1.44 = 1.4976 L/day Minimum obligatory volume of urine In order to eliminate all the solutes that are ingested over a given period of time the animal has to produce an obligatory volume of urine. The obligatory volume depends on the ability of the animal to concentrate urine. The more it can be concentrated the smaller is the required volume of urine excreted. Some animals adapted to life in the dessert have the ability to concentrate urine to levels as high as 10,000.00 mOsm/L while animals living in water can only concentrate urine to about 500 mOsm/L. Let’s assume that our 80 Kg hog has a daily solute intake of about 690 mOsm/day and it is only able to concentrate urine to 200 mOsm/L (Fig. 7-17). Then the obligatory volume for this animal will be: 690mOsm/day/1200mOsm/L = 575 mL/day V BS 122 Physiology II 52 Class of 2013 The GFR is determined by the filtration pressure and the filtration coefficient (Kf) (Fig. 7-19). GFR = FP X Kf • Smaller volume of urine • As concentrated as possible • Filtration pressure (PG‐PB‐πG+ πB) Intake = 690 mOsm/day Max. concentration = 1200 mOsm/L 690 mOsm/day = 575 mL/day 1200 mOsm/L – Glomerular capillary pressure (PG or GCP) – Capsular pressure (PB or CP) – Blood colloid osmotic pressure (πG or BCOP) – Capsular osmotic pressure (πB or COP) Figure 7-17. Calculation of the minimum obligatory daily volume of urine production • Filtration coefficient (Kf) This equation explains why animals, that in desperation drink sea water, undergo rapid dehydration. The sea water has a solute concentration of about 2400 mOsm/L. If they can only eliminate 1200 mOsm for each litter of urine, then, to eliminate the 2400 that they ingest with each litter of sea water that they drink they need to eliminate 2400mOsm/ 1200 mOsm = 2 L of water. Since they only ingested 1 litter the other litter has to come from internal sources causing rapidly an unbalance resulting in dehydration (Fig 7-18). • Sea water = 2400 mOsm/L • Max concentration = 1200 mOsm/L Figure 7-19. Factors influencing glomerular filtration rate The filtration coefficient is determined by the area of the capillary and the permeability of the filtration barrier. As a result there are many possible mechanisms to alter the GFR. A change in the filtration coefficient will change the GFR. These changes are, however, not responsible for the fine tuning of the GFR. Changes in Kf usually are observed under pathological conditions. A reduction in the total capillary surface resulting from loss of nephrons will reduce the Kf and in turn diminish the overall GFR. Thickening of the filtration barrier, as a result of hypertension, will also reduce the Kf and the GFR. The rate at which the glomerular filtration takes place is drastically influenced by the filtration pressure. The filtration pressure is the balance between the forces trying to push material out of the capillaries into the Bowman’s space, against those forces trying to prevent it (Figs. 7-19, 7-20). For each litter drank need 2400 mOsm = 2L to eliminate 1200 mOsm/L Figure 7-18. Minimum obligatory volume of urine required to eliminate all the ingested solutes The above described example assumes constant ideal conditions. In a living organism that is never the case. There are always physiological changes that influence the rate at which most processes take place. The glomerular filtration rate is no exception. V BS 122 Physiology II – Permeability FB – Capillary area GFR= Kf x (PG‐PB‐πG+ πB) 53 The main force in favour of filtration is the glomerular capillary pressure (GCP). This pressure is about 50 mm Hg and it is generated by low resistance (vasodilation) of the afferent capillary in conjunction with high resistance (vasoconstriction) of the efferent arteriole. Modifications in the resistance of these two arterioles can increase further or drastically reduce the GCP with the consequent increase or reduction in production of filtrate, respectively. Class of 2013 The main forces opposing filtration are the capsular pressure (CP) and the blood colloid osmotic pressure (BCOP). The CP is generated by the physical pressure exerted by the filtrate against the Bowman’s capsule. This usually reaches values of about 10 mm Hg. The BCOP is more variable and it is generated by the osmotic concentration existing in the capillary due to the high concentration of proteins that do not cross the filtration barrier. pressure, and as a result will increase the filtration pressure, thus increasing the GFR. The capsular pressure does not usually change much, unless there is a pathological situation such as deposit of calcium in the tubule or the formation of stones that prevent emptying of the content in the Bowman’s capsule. If this is the case the capsule pressure can increase to the point of eliminating the filtration pressure thus stopping GF. In order to try to maintain a somehow constant glomerular filtration pressure or to modify it according to the needs of the moment, the kidney resort to two mechanisms, autoregulation and sympathetic stimulation (Fig. 7-21). These mechanism permit that the animal maintains relatively constant GFR when mean arterial blood pressure oscillate within a large range (90 to 180 mm Hg). Dropping below that range triggers a significant reduction in GFR. Filtration pressure • Autoregulation Figure 7-20. Forces influencing the filtration pressure. GCP=glomerular capillary pressure, CP= capsular pressure, BCOP= blood colloid osmotic pressure Because of its nature, there is an increasing gradient within the capillaries from the end leaving the afferent arteriole towards the end of the capillary where it becomes the efferent arteriole. The increase in osmotic pressure takes place because as the blood flow within the capillary it becomes more concentrated as water leaves the capillary. The average value for the BCOP is about 30 mm Hg. Because the concentration of proteins in the filtrate is so low the capsular osmotic pressure is negligible, thus for calculations is considered to be zero. Therefore the filtration pressure can be equated as: FP= GCP- CP- BOCP or 50 - 10 - 30 = 10 mm Hg More subtle changes in GFR can be observed as a result of changes in the parameters that determine the filtration pressure. For example a small decrease in resistance by the afferent arteriole or a small increase in resistance by the efferent arteriole will increase the capillary hydrostatic V BS 122 Physiology II 54 – Modify afferent and / or efferent arteriole resistance – Tubuloglomerular feedback • Initiated by macula densa detecting flow • Activate renin‐angiotensin system • Sympathetic stimulation – Norepinephrine causes afferent arteriole vasoconstriction • Effective under severe stress or shock Figure 7-21. Mechanisms used to maintain glomerular filtration rate semi constant Autoregulation. The mechanism of autoregulation consists in modifying the resistance in the afferent and / or efferent arterioles. If the systemic mean arterial blood pressure increases, the afferent arteriole vasocontricts and or the efferent arteriole vasodilates reducing the pressure in the glomerular capillaries thus maintaining constant filtration pressure and GFR. The opposite takes place when the systemic mean arterial blood pressure decreases. Class of 2013 This auto regulatory mechanism can also be triggered by flow rate of filtrate through the distal convoluted tubule. This is described as tubuloglomerular feedback. If the cells in the macula densa detect a large change in the flow of filtrate they convey this information to the juxtaglomerular apparatus which then triggers a vasoconstriction or vasodilation in the afferent arteriole to reduce or increase filtration pressure, thus maintaining GFR constant. The signalling for this regulatory mechanism is not completely understood but it is suggested that it is implemented in the following manner. A decrease in GFR will result in a slower rate of passage of the filtrate though the loop of Henle. As a result there will be more time to reabsorb solutes from the filtrate. The filtrate leaving the loop of Henle and reaching the cells in the macula densa will have lower concentration of NaCl. This will be detected by the cells of the macula densa which will send information to the afferent arteriole to vasodilate, increasing the filtration pressure and the GFR. This signal also triggers the release of renin by the juxtaglomerular cells. Renin elevation translates in elevation of angiotensin II and, since this is a powerful vasoconstrictor for the efferent arteriole, it elevates filtration pressure and brings back the GFR to the normal rate (Fig. 7-21). Sympathetic stimulation. Sympathetic innervations uses norepinephrine as their neurotransmitter and this catecholamine has an effect in the afferent arterioles causing their vasoconstriction. This mechanism has a negligible effect when the stimulation is mild because the autoregulation mechanism takes over, but it may have a drastic effect when the stimulation is very strong. In situations of severe stress or shock, there is a drastic reduction in the irrigation of the kidney and if maintained for a long period it may cause kidney damage. A short term reduction is not harmful but provide the resources to maintain irrigated other vital organs (heart, brain, liver), and maintain homeostasis. Changes from filtrate to urine The second step in the process of making urine is to reduce the volume of the filtrate by removing most of their content, leaving the undesirable compounds to be voided in a small volume of fluid. This reduction is initiated in the tubular component of the nephron with the reabsorption of a large volume of water. The majority of the filtrate is reabsorbed in the proximal convoluted tubule. About 65% of the water is reabsorbed in this section. Another 15 % is V BS 122 Physiology II 55 reabsorbed in the loop of Henle and the final 19 % is reabsorbed in the collecting tubes leaving only about 1 % of the volume to be secreted as urine (Fig. 7-22). Reabsorption of filtrate Figure 7-22. Areas of the nephron where different volumes of filtrate are reabsorbed Reabsorption of the different components of the filtrate is achieved by active and passive mechanisms. The active mechanisms involve the expenditure of energy in the form of ATP to drive the movement of sodium against a concentration gradient from the intracellular space into the interstitial space through the basal membrane or the basolateral membrane of the tubular cells. This generates a Na+ gradient in the tubular cell with respect to the lumen of the tubule where the filtrate is located. The passive mechanisms involve diffusion, facilitated diffusion, cotransport or symport, and antiport. Proximal convoluted tubule Tubular cells are equipped with a variety of proteins, normally incorporated to the apical, lateral or basal membrane, which participate in the movement of ions and other molecules from the filtrate to the tubular cell and then to the interstitial fluid, so they can be eventually translocated to the capillaries and to circulations. These proteins make ATPases, symports, antiports, as well as, leek channels (Fig. 7-23). Class of 2013 Materials that are transported through this mechanism into the cell are, among others, amino acids, small proteins, glucose, fructose, Cl-, Ca+, K+, HCO3- and of course Na+. Water, the most abundantly reabsorbed molecule simply diffuses into the cell by osmosis. Once inside the cell most of the molecules are discarded into the interstitial fluid by facilitated diffusion. Amino acids, glucose, fructose, small proteins and K+ are all discarded through facilitated diffusion. Cl- is co transported with K+ and HCO3- is also co transported with Na+ into the interstitial fluid. Water follows by osmosis. From here all the solutes are uptaked by the peritubular capillaries and carried towards the interlobular and arcuate vein respectively. Figure 7-23. Components of a tubular cell of the proximal convoluted tubule In the proximal convoluted tubule, most of the reabsorption is dependent on the creation and maintenance of a low intracellular concentration of Na+. A low intracellular Na+ concentration generates a gradient respect to the filtrate in the tubule. The creation of this gradient is achieved by actively transporting Na+ out of the cell into the interstitial space using a pump driven by ATP (ATPase) (Fig. 7-24). In this process, for each Na+ which is removed from the cell, one K+ is incorporated into the cell from the interstitial space. This process is great to create a deficiency of Na+ but, at the same time, it accumulates K+ in the cell. After a lot of K+ is accumulated inside the cell most of it is discarded into the interstitial space by facilitated diffusion or leak channels. Once the Na+ gradient is created, a large variety of cotransporters located in the apical membrane of the tubular cell became active. These symports are proteins capable of binding a variety of solutes and molecules as well as Na+. They bind the substance first and then Na+. When Na+ binds then the protein rotate, propelled by the energy of the Na+ attraction to the inside of the cell. As it rotates the protein brings into the cell the co-transported material. Once inside the cell both Na+ and the accompanying solute or molecules are released and the protein counter rotates back to the original position, again exposing the binding sites to the lumen of the tubule. V BS 122 Physiology II 56 The net result is that large reduction I filtrate volume (about 65%). Because the cells of the convoluted tubule are so permeable to water, still at this point the filtrate maintains the same osmolal concentration than the interstitial fluid of about 300 mOsm/kg. Loop of Henle Depending on the type of nephron the loop of Henle may only descend a little bit into the medulla (cortical nephrons), or, in the case of Juxtamedullary nephrons, extend the loop of Henle deep into the medulla (Fig. 6-9). The osmolal concentration of the interstitial fluid gradually increases towards the medulla, reaching values of 1200 mOsm/kg in the area close to the tip of the renal pyramid (Fig. 7-24). This feature permits progressively increase removal of water from the filtrate. The thin descending segment of the loop of Henle is very permeable to water and less permeable to other substances as urea, sodium and other ions. As the filtrate moves in the descending limb of the loop of Henle an additional 15 % of the water is removed. Since not many solutes are removed in this section the filtrate becomes more concentrated. Furthermore, towards the end of the thin segment of the loop of Henle, some solutes are incorporated into the filtrate making it more concentrated. Once the lowest point is reached, the characteristics of the thin segment changes in such a way that the thin ascending segment of the loop of Henle is totally impermeable to water but permeable to solutes. In this section, then, no further water is removed but many solutes diffuse out of the filtrate in the lumen into the interstitial fluid and then into the vasa recta making the filtrate less concentrated. The thick segment of the ascending limb of the loop of Henle is not permeable to Class of 2013 water or to solutes but some solutes (Na+, K+ and Cl-) are symported from the filtrate to the inside of the tubular cells and once in the cell they are discarded towards the interstitial fluid by facilitated diffusion. The fact that only solutes are removed in this section make the filtrate reach concentrations of only 100 mOsm/kg as it reaches the distal convoluted tubule while the interstitial fluid at this point in the cortex is about 300 mOsm/kg (Fig. 7-24). The Starling forces are a combination of hydrostatic and oncotic forces determining the net filtration of fluids across the capillary membranes (Fig. 7-25). These can be represented by the following simplified equation: Jv = Kf ([Pc – Pi] – [πc –πi]) where Jv represents the net movement of fluids between inside and outside the capillaries. It is agreed that a positive value of Jv indicates that blood is leaving the capillary while a negative value indicates that fluid is entering the capillary. Kf represents the filtration coefficient which in turn depends of the capillary surface area and the permeability. Pc represents the hydrostatic pressure of the capillary. Pi represents the hydrostatic pressure of the interstitial space Figure 7-24. Concentration of the filtrate and the interstitial fluid at different depth of the glomerulus The movement of fluid (mainly water) between the interstitial space and the interior of the capillaries in the pericapillary bed, as well as, in the vasa recta is determined by the balance of Starling forces between these two mediums. • Hydrostatic and oncotic forces • Determine net filtration of fluids across a capillary membrane • • • • • • • πi represents the osmotic pressure of the interstitial fluid Distal convoluted tubule In the distal convoluted tubule and first section of the collecting duct there is further removal of solutes. Cl- is symported with Na+ through the apical membrane into the tubular cells and discarded into the interstitial fluid through the basal membrane by symport with K+. All of this is possible because the intracellular concentration of Na+ is maintained very low by the ATPase pump (Fig. 7-26). Collecting Duct Jv = Kf([Pc-Pi] – [πc – πi]) Jv = Net movement of fluid Kf = Filtration coefficient Pc = Hydrostatic pressure of capillaries Pi = Hydrostatic pressure interstitial space πc = Osmotic pressure of capillaries πi = Osmotic pressure of interstitial space Fig 7-25. Forces influencing the passage of fluid through capillaries V BS 122 Physiology II πc represents the capillary osmotic pressure 57 As the collecting tube enters the medulla of the kidney the interstitial fluid becomes again more and more concentrated. This concentration gradient will facilitate initially the diffusion of water from the filtrate towards the interstitial fluid. However, the permeability of the collecting duct cells to water becomes hormonal dependent. In the collecting duct the final removal of water takes place leaving the filtrate converted into urine which can be carried towards the ureter and bladder Class of 2013 Fate of other solutes In the initial filtrate there are many other solutes not mentioned so far. Urea, a product of gluconeogenesis from amino acids is one of them. Creatinine, sulphates, nitrates and phosphates are other compounds that all filtered in the renal corpuscle but eventually only partially reabsorbed. This leaves a large proportion of these materials dissolved in the urine, destined for excretion. As the filtrate reaches the collecting duct these materials are very concentrated in urine. Between 40 and 60 % of the urea in the filtrate is passively reabsorbed. The rest is concentrated and eliminated. Distal convoluted tubule Fig 7-26. The role of these cells is to further remove solutes and water. No removal of glucose or amino acids takes place in here V BS 122 Physiology II 58 Class of 2013