Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Common cold wikipedia , lookup
Immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Adaptive immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
DNA vaccination wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Henipavirus wikipedia , lookup
Innate immune system wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
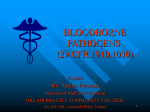
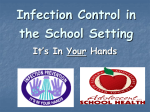
Clinical Science (2013) 124, 77–85 (Printed in Great Britain) doi: 10.1042/CS20120169 Hepatitis B virus: from immunobiology to immunotherapy Daniel GRIMM, Maximilian HEEG and Robert THIMME Department of Medicine II, University of Freiburg, D-79106 Freiburg, Germany Abstract Owing to the major limitations of current antiviral therapies in HBV (hepatitis B virus) infection, there is a strong need for novel therapeutic approaches to this major health burden. Stimulation of the host’s innate and adaptive immune responses in a way that results in the resolution of viral infection is a promising approach. A better understanding of the virus–host interaction in acute and chronic HBV infection revealed several possible novel targets for antiviral immunotherapy. In the present review, we will discuss the current state of the art in HBV immunology and illustrate how control of infection could be achieved by immunotherapeutic interventions. Key words: hepatitis B virus (HBV), immunity, immunobiology, infection, liver disease. INTRODUCTION Infection with HBV (hepatitis B virus) is a major healthcare problem, with up to 400 million people affected worldwide. The infection accounts annually for approximately 1 million deaths from cirrhosis, liver failure and HCC (hepatocellular carcinoma). Despite the availability of potent antiviral drugs such as NUCs (nucleoside/nucleotide analogues) (e.g. Entecavir or Tenofovir) and the application of PEGylated IFN (interferon) α in the treatment of chronic HBV infection, sustained virological response in terms of HBsAg (HBV surface antigen) loss and anti-HBs (HBV surface antibody) seroconversion is rarely achieved. Moreover, each of these therapeutical approaches has additional drawbacks. For NUC therapy, the optimum duration is still undefined and long-term therapy is needed. This costly therapy carries the risk of viral resistance and drug toxicity. Treatment with PEGylated IFNα has the advantage of a finite duration of treatment. However, significant side effects and low tolerability must be considered [1]. Therefore novel therapeutic approaches to this major health burden are urgently needed. A promising strategy is the development of an immunotherapy for viral control. The potential benefit of immunotherapy is supported by the facts that: (i) HBV infection is successfully controlled by natural immune responses in approximately 90 % of the individuals infected as adults; and (ii) resolution of chronic HBV infection can be achieved by bone marrow transplantation from an immune donor [2,3]. In the present review, we will recapitulate the virus–host interaction in HBV infection and show how a comprehensive understanding of immunobiology may result in promising immunotherapeutic approaches. INNATE IMMUNE RESPONSES AGAINST HBV The innate immune system has evolved as the host’s first line of defence against viral infections. By a timely recognition of viral nucleic acids, viral proteins and tissue damage it has the capacity to limit viral spread early during the course of infection. The sensing of viral components for activation of innate immune responses by PRRs (pattern recognition receptors) is a complex process that is still not completely defined. Usually, the early antiviral state consists of three major mechanisms, namely (i) production of type I IFN, (ii) killing of infected cells via NK (natural killer) cells and (iii) production of pro-inflammatory cytokines and chemokines that contribute to the maturation and recruitment of adaptive immune responses [4,5]. The role of the innate immune response in HBV infection is still not very well defined. This can be attributed to the fact that the recruitment of patients in the very early, asymptomatic phase of acute HBV infection is very difficult. Moreover, the experimental systems of HBV infection that can be used in analysing innate immune responses have major drawbacks. Animal models (e.g. mouse models, woodchucks or chimpanzees) are limited in terms Abbreviations: cccDNA, covalently closed circular DNA; CTLA-4, cytotoxic T-lymphocyte antigen 4; HBV, hepatitis B virus; HBsAg, HBV surface antigen; HCV, hepatitis C virus; HSC, hepatic stellate cell; IFN, interferon; IL, interleukin; LCMV, lymphocytic choriomeningitis virus; NK, natural killer; NUC, nucleoside/nucleotide analogue; PD-1, programmed cell death 1; rcDNA, relaxed circular DNA; TCR, T-cell receptor; TGF-β, transforming growth factor-β; TLR, Toll-like receptor; Treg, regulatory T-cells; WHV, woodchuck hepatitis virus. Correspondence: Professor Robert Thimme (email [email protected]). www.clinsci.org 77 D. Grimm, M. Heeg and R. Thimme of ethical concerns, costs and difficulties with standardization [6– 9]. Despite recent advances in cell culture models, these models suffer from a low infection efficacy and poor virus replication levels [10,11]. HBV: a ‘stealth virus’? In a prominent study from the chimpanzee model, HBV has been described as a ‘stealth virus’ that does not directly activate the host’s innate immune system in the liver [7]. Indeed, by analysing the intrahepatic gene expression after infection with a monoclonal inoculum, the authors did not observe an induction of a type I IFN response in the liver in the early infection phase. This observation has been supported by studies in humans [12,13]. For example, Dunn et al. [12] showed that circulating type I IFN was barely detectable throughout the early course of infection when analysing a cohort of 21 acute HBV patients. From the clinical point of view, this is in line with the fact that acute HBV infection usually does not induce ‘flu-like’ symptoms [14]. A possible explanation for the evasion of HBV from innate immunity may be its replication strategy. After binding of the viral particle to the hepatocyte, the nucleocapsid is released and transported to the nucleus. In the nucleus, the partially double-stranded viral rcDNA (relaxed circular DNA) is repaired and eventually cccDNA (covalently closed circular DNA) is formed [15,16]. The cccDNA remains in the nucleus of infected cells, and capped and polyadenylated viral mRNA is produced that resembles the cellular transcripts. Eventually, the viral replicative genome is sequestered within viral capsids into the cytoplasm. Thus the virus is almost invisible to the innate sensing machinery [14,17,18]. It is a hallmark of HBV infection that, owing to the persistence of cccDNA in the nucleus of infected hepatocytes, the infection can scarcely be eradicated completely [1,19]. However, the interpretation that HBV completely evades the innate immune recognition was challenged by various observations. (i) It could be shown that HBV replication in HepaRG cell lines induced a type I IFN response. The physiological relevance of this observation remains unclear, as an overexpression system based on recombinant baculoviruses was used [20]. (ii) A study in the woodchuck model showed that infection with high doses of WHV (woodchuck hepatitis virus) has the capacity to induce intrahepatic gene expression affiliated with innate and adaptive immune responses [6]. For that study, the rather high dose of WHV has to be considered, as the size of the viral inocula was discussed to be important for intracellular DNA sensing and outcome of infection [4,9,21,22]. (iii) In uPA (urokinase-type plasminogen activator)/SCID (severe combined immunodeficiency) mice harbouring human hepatocytes, baseline levels of human ISGs (interferon-stimulated genes) were slightly increased in HBVinfected animals when compared with uninfected mice [23]. This further supports the hypothesis that HBV does not completely evade innate immune recognition. (iv) Finally, activation of innate immunity might even be possible without substantial type I IFN production. Hösel et al. [24] found that, upon infection of primary human liver cells, IL (interleukin)-6 was produced. Mechanistically, IL-6 was proposed to contribute to early viral control, limiting adaptive immune responses and preventing hepatocyte death after HBV infection [24]. 78 C The Authors Journal compilation C 2013 Biochemical Society Viral measures to counteract the host’s innate immune responses Besides evidence that HBV eludes recognition by the innate immune system, several studies propose that viral proteins actively counteract the host’s innate immune response. Interference between the HBV X protein and VISA (virus-induced signalling adaptor) has been reported as a mechanism for the inhibition of type I IFN induction [25–27]. Moreover, the HBV polymerase was shown to inhibit IFNβ induction via interaction with the transcriptional factor DDX3 (dead-box 3) [28,29]. A hallmark of HBV infection is the production of a large amount of secretory proteins during the viral replication cycle, namely HBsAg and HBeAg. A possible evolutionary explanation for this could be the immunomodulatory effects of these proteins [4]. Indeed, two studies described an interference of HBV secretory proteins with TLR (Toll-like receptor)-mediated innate immune responses [30,31]. Role of NK cells in HBV infection Numerous studies have been performed in order to elucidate the role of NK cells in HBV infection. NK cells are abundant in the cellular infiltrate of the liver. They account for up to 30–40 % of the resident intrahepatic lymphocytes [32]. A hallmark of NK cells is that these cells can be activated in an antigen-independent manner either (i) by a complex interaction between inhibitory and activating receptors or (ii) via cytokines, for example IL-12, IL-15 and IL-18 [33]. In the HBV transgenic mouse model it has been shown that NK cells can inhibit HBV replication upon activation. Interestingly, the role of NK cells in HBV infection has also been analysed in a cohort of HBV infected patients in the preclinical phase and in a follow-up until resolution of the infection [12]. In this important study, the authors could show that NK cell activation and effector functions were suppressed during peak viraemia. This could be attributed to an increase in IL-10 early in infection that occurred in parallel with the rapid increase in HBV viral load [12,34]. In chronic HBV infection, NK cells upregulate the death ligand TRAIL (tumour-necrosis-factor-related apoptosis-inducing ligand) and have even been described as hypercytolytic, consequently causing liver injury [35,36]. However, NK cells have an impaired capacity to produce IFNγ in chronic HBV infection [37]. Importantly, this functional defect could not be reversed by antiviral therapy, whereas blockade of IL-10 with or without blockade of TGF-β (transforming growth factor-β) corrected the functional defect in vitro (Figure 1) [37]. Possible immunotherapeutic approaches modulating the innate immune response Overall, the stimulation of the innate immune system by TLRmediated activation has been discussed as a therapeutical approach in HBV infection (Figure 1) [4]. It could be shown in HBV-transfected hepatoma cell lines and in HBV transgenic mice that TLR activation can suppress HBV replication [38,39]. Moreover, the therapeutic efficacy of a TLR-7 agonist in woodchucks and chimpanzees has been reported recently [40,41]. The stimulation of innate immune responses is particularly promising in HBV infection, since the ability of the virus to counteract innate immune responses seems to be rather weak [42]. In addition, the activation of intrahepatic NK cells directly by cytokines Hepatitis B virus: from immunobiology to immunotherapy Figure 1 Possible targets for the modulation of innate immune responses in HBV infection The use of TLR agonists for the stimulation of innate immune responses in HBV-infected hepatocytes is a very promising immunotherapeutic approach. Furthermore, effects of antiviral drugs such as IFNα might be increased by a targeted delivery to infected cells by vehicles functioning as TCR-like antibodies. Inversely, this targeted approach might help to limit side effects. Apart from direct effects on infected hepatocytes, reconstitution of NK cell function by the blockade of inhibitory cytokines such as IL-10 might be used for the modulation of the innate immune response to HBV. (IL-12, IL-18 or IFNα) or indirectly via TLR activation as proposed by Tu et al. [43,44] for immunotherapy may be promising. Finally, TCR (T-cell receptor)-like antibodies that specifically target HBV-infected cells have been proposed as a vehicle for drug delivery (Figure 1) [45]. Using such vehicles, the targeted delivery of, for example, IFNα to infected cells could be beneficial and should be evaluated. ADAPTIVE IMMUNE RESPONSES AGAINST HBV The crucial role of virus-specific T-cells in the control of HBV infection has been shown in important studies [46,47]. After an initial quiescence of a few weeks after infection, HBV-specific CD4 + and CD8 + T-cell responses are detectable. These cell types are critical for liver disease and viral control [48,49]. Role of CD4 + T-cells In patients with acute HBV infection who ultimately clear the virus, the CD4 + T-cell response is multispecific and vigorous (Table 1). In contrast, the CD4 + response is relatively weak in patients with chronic HBV infection [18,50]. Interestingly, no effect on viral clearance and liver disease was observed when CD4 + T-cells were depleted at the peak of infection in the chimpanzee model. However, when CD4 + T-cells were depleted prior to infection, persistent infection evolved [9]. This indicates that CD4 + T-cells play a critical role in viral control without having major direct antiviral effects, for example by supporting efficient virus-specific CD8 + T-cell responses [9,18,51]. Reconstitution of CD4 + T-cell failure might be critical for a successful immunotherapy. Thus further understanding of the mechanisms behind CD4 + T-cell failure in chronic HBV is crucial [52]. The role of classical FoxP3 + CD4 + Treg (regulatory T-cells) in chronic HBV is elusive. Treg can suppress HBV-specific T-cell functions [53,54]. However, this also holds true in patients that successfully control the virus [55]. In addition, an inverse correlation between Treg frequency and ALT (alanine transaminase) levels could be shown. This observation gave rise to the hypothesis that Treg mainly have anti-inflammatory effects without having major effects on HBV persistence [4]. Role of CD8 + T-cells Several studies have clearly shown a correlation between vigorous and multi-specific CD8 + T-cell responses and HBV clearance (Table 1). The central role of CD8 + T-cells has been further confirmed by depletion studies [47]. In acute self-limiting infection, HBV-DNA falls rapidly after the peak of viral replication. The mechanisms of CD8 + T-cell-mediated viral control are still debated [52]. It has been shown that non-cytolytic mechanisms, depending on cytokines such as IFNγ or TNFα contribute to viral control, for example in chimpanzees, HBV transgenic mice and in a cell culture model [56,57]. However, the contribution of cytolytic effects must not be underestimated. This is supported by the fact that viral clearance seems to occur in the presence of liver disease in chimpanzees. Cell death might play an important role in the eradication of cccDNA from the liver [19,58]. For an immunotherapeutic approach to HBV infection, where a large proportion of liver cells is infected, a sequential restoration of noncytolytic and cytolytic mechanisms would probably be beneficial www.clinsci.org 79 D. Grimm, M. Heeg and R. Thimme Table 1 NK cell and T-cell responses at various stages of HBV and HCV infection HBV HCV Acute/resolving Chronic Chronic NK cells Suppressed during peak viraemia Impaired IFNγ production, hypercytolytic Polarization towards cytotoxicity, impaired IFNγ production CD4 + T-cells Multispecific and vigorous Weak, monospecific, dysfunctional Weak or absent, dysfunctional CD8 + T-cells Multispecific and vigorous Weak, monospecific dysfunctional, Multispecific, but exhausted to avoid major immunopathology with a potentially fatal outcome [52,59]. Furthermore, an important role for CD8 + T-cells in the development of liver cirrhosis has been shown. Indeed, it was demonstrated that CD8 + T-cells contribute to hepatic fibrosis by activating human HSCs (hepatic stellate cells) in vivo and in vitro [60]. Thus the interaction between HSCs and T-cells might represent an interesting and promising target for regulating the course of hepatic fibrosis in HBV infection. Causes of CD8 + T-cell dysfunction and ways of reconstitution HBV persistence is associated with impaired CD8 + T-cell functions, irrespective of the patient’s age at infection [4]. Probably owing to the long-term exposure of T-cells to viral antigens, HBVspecific T-cells are deleted or functionally inactivated during the course of infection [61–63]. Specifically, CD8 + T-cells targeting major HBV epitopes have been shown to be hardly detectable if viral load exceeds 107 copies/ml [62]. As viral load decreases in the first months of antiviral therapy, an increase in HBV-specific T-cell responses has been described [64,65]. However, these responses were rather transient [66]. Many different mechanisms have been suggested for T-cell failure [3]. An example for a T-cell intrinsic defect is the upregulation of the pro-apoptotic member of the Bcl-2 superfamily Bim in HBV-specific CD8 + T-cells obtained from patients with chronic HBV infection [3,67,68]. Downstream blockade of Bim restored multispecific functional responses directly ex vivo [3,67]. It has been postulated that this pro-apoptotic phenotype is fostered by tolerogenic activation by antigen-presenting cells in the liver [3]. Importantly, it could be shown that premature elimination of T-cells after antigen presentation by T-cells is also mediated by Bim [3,69,70]. Therefore specific blockade of this pro-apoptotic pathway could be a promising target in future HBV immunotherapy [3]. The balance between co-inhibitory and co-stimulatory signals during intrahepatic antigen presentation is critical for maintaining functional CD8 + T-cells. For example, an excess in co-inhibitory signals can potentially induce Bim-mediated apoptosis of HBVspecific CD8 + T-cells [61,71–74]. Amongst others, co-inhibition via the PD-1 (programmed cell death 1) pathway has been demonstrated to contribute to HBV-specific CD8 + T-cell failure in chronic HBV infection. Indeed, PD-1 expression is increased on HBV-specific CD8 + T-cells [61,71]. Moreover, expression of 80 C The Authors Journal compilation C 2013 Biochemical Society PD-1 ligands is increased on intrahepatic cells in chronic HBV infection [75]. Thus the blockade of the PD-1 pathway can serve as a potential target for immunotherapy in chronic hepatitis. Indeed, it was shown that treatment of mice with antibodies to PD-1 ligand 1 restored CD8 + T-cell functions and reduced virus replication in the LCMV (lymphocytic choriomeningitis virus) mouse model [76]. The potential relevance of blocking this inhibitory pathway in HBV was further demonstrated in the HBV mouse model [77]. Here, treatment of HBV-transgenic mice with blocking antibodies for PD-1 ligand 1 resulted in an increase in the number of IFNγ -producing CD8 + T-cells in the liver and in a delay in suppression of IFNγ -producing CD8 + T-cells (Figure 2). This approach is particularly promising, as PD-1 blockade seems to be well tolerated in cancer immunotherapy trials [78]. However, as HBV-specific CD8 + T-cells express multiple inhibitory receptors, a carefully tailored approach might be necessary for a successful HBV immunotherapy. A more detailed insight into synergy and redundancy of the multiple pathways is essential [3,52]. Combined modulation of several co-inhibitory and costimulatory pathways including, for example, 2B4 (CD244) and CTLA-4 (cytotoxic T-lymphocyte antigen 4) might be beneficial (Figure 2) [3,4,79,80]. This supposition results from the following observations. (i) In chronic HBV infection, 2B4 and PD-1 are highly co-expressed on virus-specific CD8 + T-cells. Therefore blocking 2B4 or its ligand CD48 may contribute in the restoration of CD8 + T-cell function and might as well be independent of the PD-1 pathway [80]. However, recent observations in HCV (hepatitis C virus)-specific CD8 + T-cells showed that cross-linking of 2B4 can lead to inhibition and activation of virus-specific CD8 + T-cells, depending on expression levels of 2B4 and the intracellular adaptor molecule SAP [SLAM (signalling lymphocyte activation molecule)-associated protein]. Consequently, a better understanding of the effects of 2B4 blockade in HBV infection is essential [81]. (ii) CTLA-4 is expressed by HBV-specific CD8 + T-cells with high levels of Bim. Blocking CTLA-4 resulted in an increased expansion of IFNγ -producing HBV-specific CD8 + T-cells. Apparently, this pathway is not redundant with PD-1 [79]. For a functional T-cell response, additive factors such as the liver microenvironment have to be considered [3]. This includes, among others, nutritional factors, the intrahepatic cytokine milieu and cellular constraints. At peak viraemia, HBV-specific CD8 + T-cells are activated. However, it has been shown that these cells are exhausted and that the proliferation of these cells is limited [82]. This effect has been correlated with an increase in IL-10 Hepatitis B virus: from immunobiology to immunotherapy Figure 2 Mechanisms underlying CD8 + T-cell dysfunction that might be addressed in antiviral immunotherapy Restoration of CD8 + T-cell dysfunction by interference with co-inhibitory signals is a promising approach in antiviral immunotherapy. CD8 + T-cell mediated viral control might be achieved by (i) blockade of co-inhibitory receptors such as PD-1 or 2B4 and (ii) blocking inhibitory cytokines such as TGF-β or IL-10. Reprinted from Journal of Hepatology, 52, Maini, M.K. and Schurich, A., The molecular basis of the failed immune response in chronic HBV: therapeutic implications, c (2010), with permission from Elsevier. 616–619, production (Figure 2) [82]. Moreover, this phenomenon has also been discussed as being related to an arginase release by hepatocytes, consequently leading to a lack of arginine in the inflamed liver. This was shown to interfere with CD8 + T-cell receptor signalling indirectly [83,84]. Consequently, this leads to a decrease in IL-2 production and in a defective T-cell proliferation. Therefore supplementation of IL-2 has been proposed as a therapeutic approach. However, data from the LCMV mouse model show that timing of IL-2 administration and differentiation status of T-cells are critical parameters in designing IL-2 therapies [85]. In addition, TGF-β has been discussed for HBV immunotherapy [86]. This cytokine can be produced by HBV-specific CD8 + T-cells and seems to contribute to the auto-immunosuppression of these cells [3,87]. Data from the LCMV mouse model raise hope that selective blockade of TGF-β might contribute to CD8 + T-cell restoration (Figure 2) [88]. The recent observation that IL-21 correlates with viral control defined another important cytokine that might have implications in the therapeutic augmentation of immune responses to HBV [89]. Further immunotherapeutic approaches based on adaptive immune responses On the basis of the results discussed above, reconstitution of CD4 + and CD8 + T-cell functions are very promising for HBV immunotherapy. Focusing on the reconstitution of virus-specific CD8 + T-cells, we have discussed the possible role of (i) the downstream blockade of Bim, (ii) the modulation of co-inhibitory and co-stimulatory receptors, and (iii) the modulation of inhibitory and stimulatory cytokines (Figure 3). Besides the restoration of T-cell defects, other experimental approaches have been proposed for immunotherapy in HBV infection. Several efforts have been made to develop a therapeutic vaccination in HBV infection (Figure 3). This strategy aims to eliminate viral infection by stimulation the host’s immune response. The state of the art of this antiviral approach has been reviewed elsewhere [90]. Gehring et al. [91] described the engineering of functional HBV-specific T-cells by T-cell receptor gene transfer that could potentially be used in immunotherapy (Figure 3). Another promising strategy for viral control is an immunological approach that does not rely on the restoration of HBV-specific CD8 + T-cells. In the HBV mouse model, a recombinant HBV carrying influenza epitopes was generated. These epitopes were selectively expressed in HBV-infected cells. Thus HBV-infected hepatocytes were targeted by functional influenza-specific memory T-cells. This system was shown to be effective in viral control without causing major liver injury in mice [92]. Moreover, a TCR-like antibody has been described that specifically targets HBV-infected cells (Figure 3) [45]. Thus a potential application of this TCR-like antibody could be the delivery of antiviral drugs directly to virus-infected cells [45]. www.clinsci.org 81 D. Grimm, M. Heeg and R. Thimme Figure 3 Overview of therapeutic interventions that might help to achieve viral control in HBV infection Each single approach might contribute to viral control. However, a combination of interventions is most promising. Rational combinations of immunomodulatory and antiviral therapeutics need to be tested. pegIFN-α, PEGylated IFN-α. CONCLUSIONS Comprehensive studies of innate and adaptive immune responses have highlighted several potential targets for immunotherapeutic approaches in HBV infection. The first pre-clinical and clinical trials are already ongoing in order to evaluate effects and side effects of novel therapies and have shown promising results [93,94]. Overall, the field of HBV immunotherapy shows nicely how the results of basic research can be used in order to improve patient care. 9 10 11 12 REFERENCES 13 1 2 3 4 5 6 7 8 82 European Association for the Study of the Liver (2009) EASL clinical practice guidelines: management of chronic hepatitis B. J. Hepatol. 50, 227–242 Ilan, Y., Nagler, A., Adler, R., Tur-Kaspa, R., Slavin, S. and Shouval, D. (1993) Ablation of persistent hepatitis B by bone marrow transplantation from a hepatitis B-immune donor. Gastroenterology 104, 1818–1821 Maini, M. K. and Schurich, A. (2010) The molecular basis of the failed immune response in chronic HBV: therapeutic implications. J. Hepatol. 52, 616–619 Bertoletti, A. and Ferrari, C. (2011) Innate and adaptive immune responses in chronic hepatitis B virus infections: towards restoration of immune control of viral infection. Gut, doi:10.1136/gutjnl-2011-301073 Akira, S., Uematsu, S. and Takeuchi, O. (2006) Pathogen recognition and innate immunity. Cell 124, 783–801 Guy, C. S., Mulrooney-Cousins, P. M., Churchill, N. D. and Michalak, T. I. (2008) Intrahepatic expression of genes affiliated with innate and adaptive immune responses immediately after invasion and during acute infection with woodchuck hepadnavirus. J. Virol. 82, 8579–8591 Wieland, S., Thimme, R., Purcell, R. H. and Chisari, F. V. (2004) Genomic analysis of the host response to hepatitis B virus infection. Proc. Natl. Acad. Sci. U.S.A. 101, 6669–6674 Roggendorf, M. and Tolle, T. K. (1995) The woodchuck: an animal model for hepatitis B virus infection in man. Intervirology 38, 100–112 C The Authors Journal compilation C 2013 Biochemical Society 14 15 16 17 18 19 20 21 22 Asabe, S., Wieland, S. F., Chattopadhyay, P. K., Roederer, M., Engle, R. E., Purcell, R. H. and Chisari, F. V. (2009) The size of the viral inoculum contributes to the outcome of hepatitis B virus infection. J. Virol. 83, 9652–9662 Gripon, P., Rumin, S., Urban, S., Le Seyec, J., Glaise, D., Cannie, I., Guyomard, C., Lucas, J., Trepo, C. and Guguen-Guillouzo, C. (2002) Infection of a human hepatoma cell line by hepatitis B virus. Proc. Natl. Acad. Sci. U.S.A. 99, 15655–15660 Hantz, O., Parent, R., Durantel, D., Gripon, P., Guguen-Guillouzo, C. and Zoulim, F. (2009) Persistence of the hepatitis B virus covalently closed circular DNA in HepaRG human hepatocyte-like cells. J. Gen. Virol. 90, 127–135 Dunn, C., Peppa, D., Khanna, P., Nebbia, G., Jones, M., Brendish, N., Lascar, R. M., Brown, D., Gilson, R. J., Tedder, R. J. et al. (2009) Temporal analysis of early immune responses in patients with acute hepatitis B virus infection. Gastroenterology 137, 1289–1300 Stacey, A. R., Norris, P. J., Qin, L., Haygreen, E. A., Taylor, E., Heitman, J., Lebedeva, M., DeCamp, A., Li, D., Grove, D. et al. (2009) Induction of a striking systemic cytokine cascade prior to peak viremia in acute human immunodeficiency virus type 1 infection, in contrast to more modest and delayed responses in acute hepatitis B and C virus infections. J. Virol. 83, 3719–3733 Bertoletti, A., Maini, M. K. and Ferrari, C. (2010) The host–pathogen interaction during HBV infection: immunological controversies. Antiviral Ther. 15 (Suppl. 3), 15–24 Grimm, D., Thimme, R. and Blum, H. E. (2011) HBV life cycle and novel drug targets. Hepatol. Int. 5, 644–653 Urban, S., Schulze, A., Dandri, M. and Petersen, J. (2010) The replication cycle of hepatitis B virus. J. Hepatol. 52, 282–284 Wieland, S. F. and Chisari, F. V. (2005) Stealth and cunning: hepatitis B and hepatitis C viruses. J. Virol. 79, 9369–9380 Chisari, F. V., Isogawa, M. and Wieland, S. F. (2010) Pathogenesis of hepatitis B virus infection. Pathol. Biol. 58, 258–266 Levrero, M., Pollicino, T., Petersen, J., Belloni, L., Raimondo, G. and Dandri, M. (2009) Control of cccDNA function in hepatitis B virus infection. J. Hepatol. 51, 581–592 Lucifora, J., Durantel, D., Testoni, B., Hantz, O., Levrero, M. and Zoulim, F. (2010) Control of hepatitis B virus replication by innate response of HepaRG cells. Hepatology 51, 63–72 Unterholzner, L. and Bowie, A. G. (2011) Innate DNA sensing moves to the nucleus. Cell Host Microbe 9, 351–353 Coffin, C. S. and Michalak, T. I. (1999) Persistence of infectious hepadnavirus in the offspring of woodchuck mothers recovered from viral hepatitis. J. Clin. Invest. 104, 203–212 Hepatitis B virus: from immunobiology to immunotherapy 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 Lutgehetmann, M., Bornscheuer, T., Volz, T., Allweiss, L., Bockmann, J. H., Pollok, J. M., Lohse, A. W., Petersen, J. and Dandri, M. (2011) Hepatitis B virus limits response of human hepatocytes to interferon-α in chimeric mice. Gastroenterology 140, 2074.e2–2083.e2 Hosel, M., Quasdorff, M., Wiegmann, K., Webb, D., Zedler, U., Broxtermann, M., Tedjokusumo, R., Esser, K., Arzberger, S., Kirschning, C. J. et al. (2009) Not interferon, but interleukin-6 controls early gene expression in hepatitis B virus infection. Hepatology 50, 1773–1782 Kumar, M., Jung, S. Y., Hodgson, A. J., Madden, C. R., Qin, J. and Slagle, B. L. (2011) Hepatitis B virus regulatory HBx protein binds to adaptor protein IPS-1 and inhibits the activation of β interferon. J. Virol. 85, 987–995 Wang, X., Li, Y., Mao, A., Li, C. and Tien, P. (2010) Hepatitis B virus X protein suppresses virus-triggered IRF3 activation and IFN-β induction by disrupting the VISA-associated complex. Cell. Mol. Immunol. 7, 341–348 Wei, C., Ni, C., Song, T., Liu, Y., Yang, X., Zheng, Z., Jia, Y., Yuan, Y., Guan, K., Xu, Y. et al. (2010) The hepatitis B virus X protein disrupts innate immunity by downregulating mitochondrial antiviral signaling protein. J. Immunol. 185, 1158–1168 Wang, H. and Ryu, W. S. (2010) Hepatitis B virus polymerase blocks pattern recognition receptor signaling via interaction with DDX3: implications for immune evasion. PLoS Pathog. 6, e1000986 Yu, S., Chen, J., Wu, M., Chen, H., Kato, N. and Yuan, Z. (2010) Hepatitis B virus polymerase inhibits RIG-I- and Toll-like receptor 3-mediated β interferon induction in human hepatocytes through interference with interferon regulatory factor 3 activation and dampening of the interaction between TBK1/IKKε and DDX3. J. Gen. Virol. 91, 2080–2090 Wu, J., Meng, Z., Jiang, M., Pei, R., Trippler, M., Broering, R., Bucchi, A., Sowa, J. P., Dittmer, U., Yang, D. et al. (2009) Hepatitis B virus suppresses toll-like receptor-mediated innate immune responses in murine parenchymal and nonparenchymal liver cells. Hepatology 49, 1132–1140 Visvanathan, K., Skinner, N. A., Thompson, A. J., Riordan, S. M., Sozzi, V., Edwards, R., Rodgers, S., Kurtovic, J., Chang, J., Lewin, S. et al. (2007) Regulation of Toll-like receptor-2 expression in chronic hepatitis B by the precore protein. Hepatology 45, 102–110 Norris, S., Collins, C., Doherty, D. G., Smith, F., McEntee, G., Traynor, O., Nolan, N., Hegarty, J. and O’Farrelly, C. (1998) Resident human hepatic lymphocytes are phenotypically different from circulating lymphocytes. J. Hepatol. 28, 84–90 Fauriat, C., Long, E. O., Ljunggren, H. G. and Bryceson, Y. T. (2010) Regulation of human NK-cell cytokine and chemokine production by target cell recognition. Blood 115, 2167–2176 Velikova, V., Salerno, G., Frati, F., Peri, E., Conti, E., Colazza, S. and Loreto, F. (2010) Influence of feeding and oviposition by phytophagous pentatomids on photosynthesis of herbaceous plants. J. Chem. Ecol. 36, 629–641 Zhang, Z., Zhang, S., Zou, Z., Shi, J., Zhao, J., Fan, R., Qin, E., Li, B., Li, Z., Xu, X. et al. (2011) Hypercytolytic activity of hepatic natural killer cells correlates with liver injury in chronic hepatitis B patients. Hepatology 53, 73–85 Dunn, C., Brunetto, M., Reynolds, G., Christophides, T., Kennedy, P. T., Lampertico, P., Das, A., Lopes, A. R., Borrow, P., Williams, K. et al. (2007) Cytokines induced during chronic hepatitis B virus infection promote a pathway for NK cell-mediated liver damage. J. Exp. Med. 204, 667–680 Peppa, D., Micco, L., Javaid, A., Kennedy, P. T., Schurich, A., Dunn, C., Pallant, C., Ellis, G., Khanna, P., Dusheiko, G. et al. (2010) Blockade of immunosuppressive cytokines restores NK cell antiviral function in chronic hepatitis B virus infection. PLoS Pathog. 6, e1001227 Guo, H., Jiang, D., Ma, D., Chang, J., Dougherty, A. M., Cuconati, A., Block, T. M. and Guo, J. T. (2009) Activation of pattern recognition receptor-mediated innate immunity inhibits the replication of hepatitis B virus in human hepatocyte-derived cells. J. Virol. 83, 847–858 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 Isogawa, M., Robek, M. D., Furuichi, Y. and Chisari, F. V. (2005) Toll-like receptor signaling inhibits hepatitis B virus replication in vivo. J. Virol. 79, 7269–7272 Menne, S., Tennant, B. C., Liu, K. H., Ascenzi, M. A., Baldwin, B. H., Bellezza, C. A., Cote, P. J., Zheng, X., Wolfgang, G. and Tumas, D. (2011) Anti-viral efficacy and induction of an antibody response against surface antigen with the TLR7 agonist GS-9620 in the woodchuck model of chronic HBV infection. 46th Annual Meeting of the European Association for the Study of the Liver, Berlin, 30 March–3 April 2012, Abstract 992 Wadsworth, C. A., Dixon, P. H., Zabron, A. A., Wong, J. H., Chapman, M. H., McKay, S. C., Sharif, A. W., Spalding, D. R., Pereira, S. P., Wasan, H. S. et al. (2011) Genetic variation in biliary transporters as a susceptibility factor for cholangiocarcinoma., 46th Annual Meeting of the European Association for the Study of the Liver, Berlin, 30 March–3 April 2012, Abstract 384 Muhammed, R., Bremner, R., Protheroe, S., Johnson, T., Holden, C. and Murphy, M. S. (2011) Resolution of parenteral nutrition associated jaundice on changing from a soya-oil emulsion to a complex mixed-lipid emulsion. J. Pediatr. Gastroenterol. Nutr. 54, 797–802 Tu, Z., Hamalainen-Laanaya, H. K., Crispe, I. N. and Orloff, M. S. (2011) Synergy between TLR3 and IL-18 promotes IFN-γ dependent TRAIL expression in human liver NK cells. Cell. Immunol. 271, 286–291 Tu, Z., Bozorgzadeh, A., Pierce, R. H., Kurtis, J., Crispe, I. N. and Orloff, M. S. (2008) TLR-dependent cross talk between human Kupffer cells and NK cells. J. Exp. Med. 205, 233–244 Sastry, K. S., Too, C. T., Kaur, K., Gehring, A. J., Low, L., Javiad, A., Pollicino, T., Li, L., Kennedy, P. T., Lopatin, U. et al. (2011) Targeting hepatitis B virus-infected cells with a T-cell receptor-like antibody. J. Virol. 85, 1935–1942 Fisicaro, P., Valdatta, C., Boni, C., Massari, M., Mori, C., Zerbini, A., Orlandini, A., Sacchelli, L., Missale, G. and Ferrari, C. (2009) Early kinetics of innate and adaptive immune responses during hepatitis B virus infection. Gut 58, 974–982 Thimme, R., Wieland, S., Steiger, C., Ghrayeb, J., Reimann, K. A., Purcell, R. H. and Chisari, F. V. (2003) CD8 + T cells mediate viral clearance and disease pathogenesis during acute hepatitis B virus infection. J. Virol. 77, 68–76 Whalley, S. A., Murray, J. M., Brown, D., Webster, G. J., Emery, V. C., Dusheiko, G. M. and Perelson, A. S. (2001) Kinetics of acute hepatitis B virus infection in humans. J. Exp. Med. 193, 847–854 Webster, G. J., Reignat, S., Maini, M. K., Whalley, S. A., Ogg, G. S., King, A., Brown, D., Amlot, P. L., Williams, R., Vergani, D. et al. (2000) Incubation phase of acute hepatitis B in man: dynamic of cellular immune mechanisms. Hepatology 32, 1117–1124 Ferrari, C., Penna, A., Bertoletti, A., Valli, A., Antoni, A. D., Giuberti, T., Cavalli, A., Petit, M. A. and Fiaccadori, F. (1990) Cellular immune response to hepatitis B virus-encoded antigens in acute and chronic hepatitis B virus infection. J. Immunol. 145, 3442–3449 Glover, G., Bernabe, M. J. and Carbonell, P. (2001) Diagnosis of fragile X syndrome. Rev. Neurol. 33 (Suppl. 1), S6–S9 Callendret, B. and Walker, C. (2011) A siege of hepatitis: immune boost for viral hepatitis. Nat. Med. 17, 252–253 Xu, D., Fu, J., Jin, L., Zhang, H., Zhou, C., Zou, Z., Zhao, J. M., Zhang, B., Shi, M., Ding, X. et al. (2006) Circulating and liver resident CD4 + CD25 + regulatory T-cells actively influence the antiviral immune response and disease progression in patients with hepatitis B. J. Immunol. 177, 739–747 Stoop, J. N., van der Molen, R. G., Baan, C. C., van der Laan, L. J., Kuipers, E. J., Kusters, J. G. and Janssen, H. L. (2005) Regulatory T cells contribute to the impaired immune response in patients with chronic hepatitis B virus infection. Hepatology 41, 771–778 Franzese, O., Kennedy, P. T., Gehring, A. J., Gotto, J., Williams, R., Maini, M. K. and Bertoletti, A. (2005) Modulation of the CD8 + -T-cell response by CD4 + CD25 + regulatory T cells in patients with hepatitis B virus infection. J. Virol. 79, 3322–3328 www.clinsci.org 83 D. Grimm, M. Heeg and R. Thimme 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 84 Phillips, S., Chokshi, S., Riva, A., Evans, A., Williams, R. and Naoumov, N. V. (2010) CD8 + T cell control of hepatitis B virus replication: direct comparison between cytolytic and noncytolytic functions. J. Immunol. 184, 287–295 Guidotti, L. G., Rochford, R., Chung, J., Shapiro, M., Purcell, R. and Chisari, F. V. (1999) Viral clearance without destruction of infected cells during acute HBV infection. Science 284, 825–829 Mason, W. S., Litwin, S., Xu, C. and Jilbert, A. R. (2007) Hepatocyte turnover in transient and chronic hepadnavirus infections. J. Viral Hepat. 14 (Suppl. 1), 22–28 McMahan, R. H., Golden-Mason, L., Nishimura, M. I., McMahon, B. J., Kemper, M., Allen, T. M., Gretch, D. R. and Rosen, H. R. (2010) Tim-3 expression on PD-1 + HCV-specific human CTLs is associated with viral persistence, and its blockade restores hepatocyte-directed in vitro cytotoxicity. J. Clin. Invest. 120, 4546–4557 Muhanna, N., Doron, S., Wald, O., Horani, A., Eid, A., Pappo, O., Friedman, S. L. and Safadi, R. (2008) Activation of hepatic stellate cells after phagocytosis of lymphocytes: a novel pathway of fibrogenesis. Hepatology 48, 963–977 Boni, C., Fisicaro, P., Valdatta, C., Amadei, B., Di Vincenzo, P., Giuberti, T., Laccabue, D., Zerbini, A., Cavalli, A., Missale, G. et al. (2007) Characterization of hepatitis B virus (HBV)-specific T-cell dysfunction in chronic HBV infection. J. Virol. 81, 4215–4225 Webster, G. J., Reignat, S., Brown, D., Ogg, G. S., Jones, L., Seneviratne, S. L., Williams, R., Dusheiko, G. and Bertoletti, A. (2004) Longitudinal analysis of CD8 + T cells specific for structural and nonstructural hepatitis B virus proteins in patients with chronic hepatitis B: implications for immunotherapy. J. Virol. 78, 5707–5719 Maini, M. K., Boni, C., Lee, C. K., Larrubia, J. R., Reignat, S., Ogg, G. S., King, A. S., Herberg, J., Gilson, R., Alisa, A. et al. (2000) The role of virus-specific CD8 + cells in liver damage and viral control during persistent hepatitis B virus infection. J. Exp. Med. 191, 1269–1280 Boni, C., Penna, A., Ogg, G. S., Bertoletti, A., Pilli, M., Cavallo, C., Cavalli, A., Urbani, S., Boehme, R., Panebianco, R. et al. (2001) Lamivudine treatment can overcome cytotoxic T-cell hyporesponsiveness in chronic hepatitis B: new perspectives for immune therapy. Hepatology 33, 963–971 Boni, C., Bertoletti, A., Penna, A., Cavalli, A., Pilli, M., Urbani, S., Scognamiglio, P., Boehme, R., Panebianco, R., Fiaccadori, F. and Ferrari, C. (1998) Lamivudine treatment can restore T cell responsiveness in chronic hepatitis B. J. Clin. Invest. 102, 968–975 Boni, C., Penna, A., Bertoletti, A., Lamonaca, V., Rapti, I., Missale, G., Pilli, M., Urbani, S., Cavalli, A., Cerioni, S. et al. (2003) Transient restoration of anti-viral T cell responses induced by lamivudine therapy in chronic hepatitis B. J. Hepatol. 39, 595–605 Lopes, A. R., Kellam, P., Das, A., Dunn, C., Kwan, A., Turner, J., Peppa, D., Gilson, R. J., Gehring, A., Bertoletti, A. and Maini, M. K. (2008) Bim-mediated deletion of antigen-specific CD8 T cells in patients unable to control HBV infection. J. Clin. Invest. 118, 1835–1845 Grayson, J. M., Weant, A. E., Holbrook, B. C. and Hildeman, D. (2006) Role of Bim in regulating CD8 + T-cell responses during chronic viral infection. J. Virol. 80, 8627–8638 Holz, L. E., Benseler, V., Bowen, D. G., Bouillet, P., Strasser, A., O’Reilly, L., d’Avigdor, W. M., Bishop, A. G., McCaughan, G. W. and Bertolino, P. (2008) Intrahepatic murine CD8 T-cell activation associates with a distinct phenotype leading to Bim-dependent death. Gastroenterology 135, 989–997 Bowen, D. G., Zen, M., Holz, L., Davis, T., McCaughan, G. W. and Bertolino, P. (2004) The site of primary T cell activation is a determinant of the balance between intrahepatic tolerance and immunity. J. Clin. Invest. 114, 701–712 Fisicaro, P., Valdatta, C., Massari, M., Loggi, E., Biasini, E., Sacchelli, L., Cavallo, M. C., Silini, E. M., Andreone, P., Missale, G. and Ferrari, C. (2010) Antiviral intrahepatic T-cell responses can be restored by blocking programmed death-1 pathway in chronic hepatitis B. Gastroenterology 138, 682–693, 693 e1–e4 C The Authors Journal compilation C 2013 Biochemical Society 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 Diehl, L., Schurich, A., Grochtmann, R., Hegenbarth, S., Chen, L. and Knolle, P. A. (2008) Tolerogenic maturation of liver sinusoidal endothelial cells promotes B7-homolog 1-dependent CD8 + T cell tolerance. Hepatology 47, 296–305 Isogawa, M., Furuichi, Y. and Chisari, F. V. (2005) Oscillating CD8 + T cell effector functions after antigen recognition in the liver. Immunity 23, 53–63 Dong, H., Zhu, G., Tamada, K., Flies, D. B., van Deursen, J. M. and Chen, L. (2004) B7-H1 determines accumulation and deletion of intrahepatic CD8 + T lymphocytes. Immunity 20, 327–336 Kassel, R., Cruise, M. W., Iezzoni, J. C., Taylor, N. A., Pruett, T. L. and Hahn, Y. S. (2009) Chronically inflamed livers up-regulate expression of inhibitory B7 family members. Hepatology 50, 1625–1637 Barber, D. L., Wherry, E. J., Masopust, D., Zhu, B., Allison, J. P., Sharpe, A. H., Freeman, G. J. and Ahmed, R. (2006) Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 439, 682–687 Maier, H., Isogawa, M., Freeman, G. J. and Chisari, F. V. (2007) PD-1:PD-L1 interactions contribute to the functional suppression of virus-specific CD8 + T lymphocytes in the liver. J. Immunol. 178, 2714–2720 Brahmer, J. R., Drake, C. G., Wollner, I., Powderly, J. D., Picus, J., Sharfman, W. H., Stankevich, E., Pons, A., Salay, T. M., McMiller, T. L. et al. (2010) Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 28, 3167–3175 Schurich, A., Khanna, P., Lopes, A. R., Han, K. J., Peppa, D., Micco, L., Nebbia, G., Kennedy, P. T., Geretti, A. M., Dusheiko, G. and Maini, M. K. (2011) Role of the coinhibitory receptor cytotoxic T lymphocyte antigen-4 on apoptosis-prone CD8 T cells in persistent hepatitis B virus infection. Hepatology 53, 1494–1503 Raziorrouh, B., Schraut, W., Gerlach, T., Nowack, D., Gruner, N. H., Ulsenheimer, A., Zachoval, R., Wachtler, M., Spannagl, M., Haas, J. et al. (2010) The immunoregulatory role of CD244 in chronic hepatitis B infection and its inhibitory potential on virus-specific CD8 + T-cell function. Hepatology 52, 1934–1947 Schlaphoff, V., Lunemann, S., Suneetha, P. V., Jaroszewicz, J., Grabowski, J., Dietz, J., Helfritz, F., Bektas, H., Sarrazin, C., Manns, M. P. et al. (2011) Dual function of the NK cell receptor 2B4 (CD244) in the regulation of HCV-specific CD8 + T cells. PLoS Pathog. 7, e1002045 Purkayastha, S., Fernando, S. S., Diallo, S., Cohen, L., Ranasinghe, B., Levano, K. and Banerjee, P. (2009) Regulation of protein kinase C isozymes during early postnatal hippocampal development. Brain Res. 1288, 29–41 Das, A., Hoare, M., Davies, N., Lopes, A. R., Dunn, C., Kennedy, P. T., Alexander, G., Finney, H., Lawson, A., Plunkett, F. J. et al. (2008) Functional skewing of the global CD8 T cell population in chronic hepatitis B virus infection. J. Exp. Med. 205, 2111–2124 Chisari, F. V. (1978) Regulation of human lymphocyte function by a soluble extract from normal human liver. J. Immunol. 121, 1279–1286 Blattman, J. N., Grayson, J. M., Wherry, E. J., Kaech, S. M., Smith, K. A. and Ahmed, R. (2003) Therapeutic use of IL-2 to enhance antiviral T-cell responses in vivo. Nat. Med. 9, 540–547 Shevach, E. M. (2010) TGF-β to the rescue. Immunity 32, 585–587 Swarowsky, A., Rodrigues, L., Biasibetti, R., Leite, M. C., de Oliveira, L. F., de Almeida, L. M., Gottfried, C., Quillfeldt, J. A., Achaval, M. and Goncalves, C. A. (2008) Glial alterations in the hippocampus of rats submitted to ibotenic-induced lesion of the nucleus basalis magnocellularis. Behav. Brain Res. 190, 206–211 Tinoco, R., Alcalde, V., Yang, Y., Sauer, K. and Zuniga, E. I. (2009) Cell-intrinsic transforming growth factor-β signaling mediates virus-specific CD8 + T cell deletion and viral persistence in vivo. Immunity 31, 145–157 Hepatitis B virus: from immunobiology to immunotherapy 89 90 91 Publicover, J., Goodsell, A., Nishimura, S., Vilarinho, S., Wang, Z. E., Avanesyan, L., Spolski, R., Leonard, W. J., Cooper, S. and Baron, J. L. (2011) IL-21 is pivotal in determining age-dependent effectiveness of immune responses in a mouse model of human hepatitis B. J. Clin. Invest. 121, 1154–1162 Michel, M. L., Deng, Q. and Mancini-Bourgine, M. (2011) Therapeutic vaccines and immune-based therapies for the treatment of chronic hepatitis B: perspectives and challenges. J. Hepatol. 54, 1286–1296 Gehring, A. J., Xue, S. A., Ho, Z. Z., Teoh, D., Ruedl, C., Chia, A., Koh, S., Lim, S. G., Maini, M. K., Stauss, H. et al. (2011) Engineering virus-specific T cells that target HBV infected hepatocytes and hepatocellular carcinoma cell lines. J. Hepatol. 55, 103–110 92 93 94 Deng, Q., Mancini-Bourgine, M., Zhang, X., Cumont, M. C., Zhu, R., Lone, Y. C. and Michel, M. L. (2009) Hepatitis B virus as a gene delivery vector activating foreign antigenic T cell response that abrogates viral expression in mouse models. Hepatology 50, 1380–1391 Caselitz, M., Link, H., Hein, R., Maschek, H., Boker, K., Poliwoda, H. and Manns, M. P. (1997) Hepatitis B associated liver failure following bone marrow transplantation. J. Hepatol. 27, 572–527 Lok, A. S., Liang, R. H., Chiu, E. K., Wong, K. L., Chan, T. K. and Todd, D. (1991) Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Report of a prospective study. Gastroenterology 100, 182–188 Received 3 April 2012/20 June 2012; accepted 5 July 2012 Published on the Internet 12 September 2012, doi: 10.1042/CS20120169 www.clinsci.org 85