Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
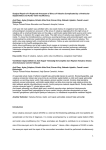
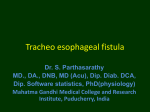
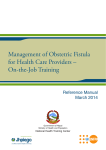
IMAGES IN MEDICINE Heart, Lung and Vessels. In press Aortic to right atrial fistula secondary to chronic ruptured sinus of Valsalva aneurysm Nisal K. Perera1, Sean D. Galvin1, Omar Farouque2, George Matalanis1 Departments of Cardiac Surgery1 and Cardiology2, Austin Health, Heidelberg, Victoria, Australia Keywords: adult cardiac surgery, aortic surgery, heart failure. A sinus of Valsalva aneurysm (SOVA) is an uncommon cardiac anomaly occurring in less than 1% of patients undergoing open cardiac surgical procedures (1). Approximately 65-85% of SOVAs originate from the right sinus of Valsalva, while SOVAs originating from noncoronary (10-30%) and left sinuses (<5%) are less common (2). It may be congenital or acquired in origin and may rupture into any of the cardiac chambers to form an aorto-cardiac fistula. When intra-cardiac rupture occurs, early surgical intervention is indicated as rupture may lead to serious hemodynamic instability, acute heart failure and, if left untreated, has a mean survival period of 1–2 years (3). Although there have been suc- Figure 1 - Short Axis view of TEE confirmed a ruptured non-coronary SOVA with torrential aortic to right atrial shunt. AV = Aortic Valve; FT = Fistula Tract; RA = Right Atrium. Corresponding author: Dr Nisal Kalhara Perera Department of Cardiac Surgery Austin Hospital PO Box 5555, Heidelberg, Victoria, 3084 Australia E-mail: [email protected] Heart, Lung and Vessels. 2014, Vol. 6 1 Perera NK, Galvin SD, Farouque O, Matalanis G 2 cessful reports of transcatheter closure (4, 5), no dedicated closure devices exist and open surgical repair remains the mainstay of treatment. We present a case of a chronic ruptured non-coronary SOVA illustrating the classical “windsock” appearance of the aorta to right atrial fistula tract and correlate the non-invasive imaging appearances with those seen at the time of open surgical repair. A 50-year-old female presented with a 2-week history of sudden onset shortness of breath, impaired exercise tolerance and orthopnoea. Past medical history included rheumatoid arthritis. Her vital signs were: heart rate 102 beats per minute, respiratory rate 28 breaths per minute, blood pressure 112/52mmHg, oxygen saturation 98% on room air and NYHA class III. On cardiovascular examination she was noted to have clinical signs of biventricular heart failure with a sinus tachycardia, elevated jugular venous pulse, a continuous murmur, bilateral pulmonary crepitations and pitting Figure 2 - Left heart catheterization study showing a large aortic to right atrial shunt. Asc = Ascending Aorta; FT = Fistula Tract; RA = Right Atrium. Figure 3 - Intra operative image of the fistula tract protruding from the base of the non-coronary sinus with a “windsock” appearance. Fistula tract is identified by the forceps. edema in the lower limbs. Transesophageal echocardiogram (TEE) confirmed a ruptured non-coronary SOVA with a torrential aortic to right atrial shunt and right heart volume overload. The fistula tract was seen as a “windsock” originating in the non-coronary sinus and projecting into the right atrium (Figure 1). There were no other cardiac abnormalities identified on TEE. Right and left heart catheterization studies showed normal coronary anatomy, elevated right heart pressures [mean RA: 31 mmHg, RV: 62/24 mmHg, PA: 55/31 (mean = 43 mmHg] and a large left to right shunt (Qp:Qs 3.2:1) (Figure 2). The patient was operated on with urgent status (during current hospital stay) after a short intensive period of diuretic therapy. At operation there was a 2cm defect in the non coronary sinus with a fistula tract of thinned aortic wall protruding from the base of the non coronary sinus into the right atrium with the appearances of a “windsock” (Figure 3). The “windsock” was delivered back into the aorta from its right atrial position and its apex was seen to have multiple perforations resulting in the fistula. The tissue that made up the Heart, Lung and Vessels. 2014, Vol. 6 Chronic Ruptured SOVA “windsock” was excised and a bovine pericardial patch was used to repair the defect in the non-coronary sinus. After weaning from cardiopulmonary bypass, intra-operative TEE revealed a satisfactory repair with no residual fistula connection and normal aortic and tricuspid valve function. The patient had an unremarkable recovery and was discharged home on the 6th post operative day. At 6-week follow up she was symptom free and transthoracic echocardiogram revealed normal cardiac function with no detectable shunt. This case serves to highlight the importance of early identification and treatment of a ruptured SOVA as it can bring rapid and permanent symptomatic relief. Surgery can be performed with low morbidity and mortality with 10-year survival rates of 6393% (3, 6). In the presence of an otherwise normal aortic valve and root, the SOVA can be treated locally with either pericardial patch closure of the defect or replacement of the sinus with a Dacron patch with pres- ervation of the native aortic valve. When a diagnosis of ruptured SOVA is made, we advocate early surgical repair as if left untreated progressive heart failure and premature death may occur. REFERENCES 1. Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, et al. Sinus of Valsalva aneurysm or fistula: management and outcome. The Annals of thoracic surgery 1999; 68: 1573-7. 2. Meier JH, Seward JB, Miller FA Jr., Oh JK, Enriquez-Sarano M. Aneurysms in the left ventricular outflow tract: clinical presentation, causes, and echocardiographic features. J Am Soc Echocardiogr 1998; 11: 729-45. 3. Sarikaya S, Adademir T, Elibol A, Buyukbayrak F, Onk A, Kirali K. Surgery for ruptured sinus of Valsalva aneurysm: 25-year experience with 55 patients. Eur J Cardiothorac Surg 2013; 43: 591-6. 4. Chen F, Li SH, Qin YW, Li P, Liu SX, Dong J, et al. Transcatheter closure of giant ruptured sinus of valsalva aneurysm. Circulation 2013; 128: 1-3. 5. Kuriakose EM, Bhatla P, McElhinney DB. Comparison of Reported Outcomes With Percutaneous Versus Surgical Closure of Ruptured Sinus of Valsalva Aneurysm. Am J Cardiol. 2015; 115: 392-398. 6. Moustafa S, Mookadam F, Cooper L, Adam G, Zehr K, Stulak J, et al. Sinus of Valsalva aneurysms--47 years of a single center experience and systematic overview of published reports. The American journal of cardiology 2007; 99: 115964. Cite this article as: Perera NK, Galvin SD, Farouque O, Matalanis G. Aortic to right atrial fistula secondary to chronic ruptured sinus of Valsalva aneurysm. Heart, Lung and Vessels. 2015. In press. Source of Support: Nil. Disclosures: None declared. Heart, Lung and Vessels. 2014, Vol. 6 3