Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Echocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
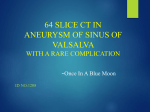
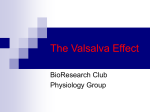
Unusual Ruptured Sinus of Valsalva Aneurysm Case Report Acta Cardiol Sin 2009;25:52-5 Rupture of Right Sinus of Valsalva Aneurysm with Alternating Shunting into Right Atrium and Right Ventricle Ming-Shyan Lin,1 Chia-Pin Lin,1 Jaw-Ji Chu,2 Yuan-Chang Liu3 and Pao-Hsien Chu1 Sinus of Valsalva aneurysm (SVA) is a rare cardiac anomaly that may be congenital or acquired. We report the case of a 29-year-old female who presented with a three-month history of exertional dyspnea. Cardiac auscultation revealed a grade III/VI continuous murmur along the right sternal border. Transthoracic echocardiography revealed alternating jet-flows into the right atrium (RA) and right ventricle (RV) during different phases of the cardiac cycle. The aortography revealed periodic movement of a jet of contrast medium, which was due to a long windsock SVA swimming between RA and RV. The aneurysm descended into the tricuspid orifice during diastole, and was possibly lifted by the leaflet of the tricuspid valve closure during systole. The patient underwent open-heart surgery to close the aneurysm ostium and directly suture the right atrial fistula. Key Words: Sinus of Valsalva aneurysm · SVA rupture · Right atrium · Right ventricle the left sinuses.2 The incidence of SVA in males is 2-3 times higher than in females. The most common associated cardiovascular lesions are ventricular septal defects (VSDs) and aortic valve insufficiencies.3 Structural defects are also one of the anomalies observed in association with congenital SVAs, including the bicuspid aortic valve, pulmonary stenosis, cocarctation, tetralogy of Fallot, patent ductus arteriosus and atrial septal defects (ASDs).4 SVA can be diagnosed by transthoracic echocardiography (TTE), but this technique has some limitations in terms of confirmation. We report an unusual and interesting case in which the presence of alternating jet flows initially revealed rupture of right SVA that was descending from the right atrium (RA) to the right ventricle (RV) along with a small ASD; this finding was finally confirmed at surgery. We focus on echocardiographic features and provide surgical findings to describe the condition. INTRODUCTION Congenital sinus of Valsalva aneurysm (SVA) is caused by dilation, usually of a single sinus of Valsalva due to deficiencies in tissue elasticity.1 Abnormal development of the bulbous cordis has been associated with SVA development. Acquired etiologies include trauma, infection, endocarditis, syphilis, Marfan syndrome, and senile dilation of sinus and left coronary sinus. A recent Mayo Clinic study and reviews have revealed that approximately 70% of SVAs originate from the right sinus of Valsalva, 26% from the non-coronary, AND 5% from Received: May 11, 2008 Accepted: July 29, 2008 1 Division of Cardiology, Department of Internal Medicine; 2Division of Thoracic and Cardiovascular Surgery, Chang Gung Memorial Hospital; 3Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Taipei, Taiwan. Address correspondence and reprint requests to: Dr. Pao-Hsien Chu, First Cardiovascular Division, Department of Internal Medicine, Chang Gung Memorial Hospital, 199 Tun-Hwa North Road, Taipei 105, Taiwan. Tel: 886-3-328-1200 ext. 8162; Fax: 886-3-327-1192; E-mail: [email protected] Acta Cardiol Sin 2009;25:52-5 CASE REPORT This is a report of a 29-year-old female who was 52 Unusual Ruptured Sinus of Valsalva Aneurysm ent directions; the jet flow going into the RV during diastole disappeared during systole, and an alternating blood flow into the RA appeared (Figures 1A and 1B). Ventricular septal defect (VSD) could not be ruled out completely due to the absence of obvious bulging of the sinus of Valsalva or vegetations. The patient refused to undergo transesophageal echocardiography (TEE) even after a comprehensive description of the procedure was provided. Computed tomography angiography (CTA) was performed, and it revealed a tubular structure from the anterior base of the right sinus of Valsalva, with a maximum diameter of 6 mm. The tract ran posteriorly and became an aneurysm-like structure (17 ´ 14.5 mm), located within the RA and attached to the tricuspid valve (TV) (Figures 1C and 1D). Cardiac catheterization revealed elevated pulmonary artery pressure (S/D 33/11, mean 23 mmHg) and oxygen saturation step-up at the RA and RV. [SVC: 56% (High), 59% (Low), IVC: 46% (Low), 59% (High), RA: 73% (High), 81% (Middle), healthy previously and presented refractory cough, progressive dyspnea and intermittent palpitations during the preceding 3 months. Murmur over the right parasternal border was also noted at a local clinic, and the patient was then transferred to our hospital for further examination. Physical examination revealed an engorged jugular vein (9 cm above the Lewis angle) and mild leg edema. A continuous heart murmur was heard over the right upper and lower sternal borders, and crackles were also heard over the bilateral basal lung fields. A hemogram revealed normocytic anemia (hemoglobin 12.6 g/dL), and biochemical profile revealed normal renal functions (creatinine 0.9 mg/dL) and negative cardiac enzymes creatine kinase-MB (CK-MB) 6 ng/mL and troponin-I, 0.13 ng/mL. At admittance, the patient’s vital signs were 37.3 °C, 105 bpm, 17 breaths/min and 108/60 mmHg. Chest X-rays revealed mild pulmonary congestion without cardiomegaly. TTE revealed two jet flows of differ- Figure 1. Color flow Doppler images in short-axis view demonstrating alternating bidirectional turbulent flow to the right atrium during systole (A), and ventricle during diastole. (B) Computed tomographic angiography images reveal a tubular structure from the anterior base of the right sinus of Valsalva, with a maximum diameter of 6 mm. (C) The tract ran posterior and became an aneurysm-like structure, sized 17 × 14.5 mm; it was located within the RA and attached to the tricuspid valve. (D) The aortogram demonstrated mild aortic regurgitation and sinus of Valsalva aneurysm presence, with jets into the right ventricle during diastole (arrowheads). (E) The left ventricle angiography revealed absent existence of ventricular septal defect but showed contrast leaking into the right atrium during systole (arrowheads). (F) (AV = aortic valve; LA = left atrium; RA = right atrium; RV = right ventricle; TV = tricuspid valve; RC = right coronary cuspid; SVA=sinus of Valsalva aneurysm). 53 Acta Cardiol Sin 2009;25:52-5 Ming-Shyan Lin et al. signs.6 These murmurs are loud, stentorian and continuous; they vary in intensity during systole and diastole, and are best heard at the base of the heart. The murmurs start in the systole and continue to the diastole, peaking near S2. The intensity of the murmurs may be diminished at around the second heart sound, only to increase again during diastole, creating a ‘to-and-fro’ cadence. Possible differential diagnoses include patent ductus arteriosus, ruptured SVA, cervical venous hum, mammary soufflé of pregnancy, coronary arteries, great vessel, or hemodialysis AV fistulas. Echocardiography remains the best non-invasive diagnostic tool, and it can detect the wall of the aneurysm and the disturbed flow within the aneurysm or at the site of perforation.7,8 TEE may provide more precise and optimal information than TTE if performed prior to surgery. If the aneurysm is ruptured, color flow Doppler mapping can show a continuous turbulent jet within the aneurysm that would drain into the receiving chamber. If the aneurysm has ruptured into the RA or RV, the flow would be continuous during both systole and diastole according to pressure gradient. If an aneurysm is not observed with TTE, further study with TEE, MRI, CT, or aortography should be performed to obtain complementary data for the SVA diagnosis. In our case, SVA could not be identified easily due to the location, we could visualize one jet flow into the RV during the early to mid-diastole, and another jet flow into the RA cavity was noted during systole. Interestingly, we found that two jet flows originated from the same location but had different directions that differed with the phase of the cardiac cycles. Since the major jet flow was into the RV and occurred during diastole, the possibility of a VSD (systolic phase) could be excluded. Sequential cardiac catheterization confirmed the diagnosis of an SVA running from the RA to RV without a VSD. By using LV angiography and aortography, we could describe the dynamic movement of the alternating jet flows from a long windsock SVA from the RA to RV through the TV, and the aneurysm descended into the tricuspid orifice during diastole, and was lifted by the leaflet of the TV during systole. From a surgical viewpoint, our case is unique because SVA was suspected on the basis of an interesting echocardiographic feature; an SVA that communicated with both cardiac chambers, namely, RA and RV, or an 74% (Low), RV: 88% (In), 89% (Body), and 83% (Out)]. Furthermore, transcardiac shunting was suspected, and the shunt ratio (Qp/Qs) was 3.2. Aortography revealed an aortocardiac shunt between the RA and RV, suggesting a ruptured SVA (Figures 1E and 1F). During surgery, a right SVA that ruptured into the junction of TV and RA was noted and an incidental small ASD was also found (Figure 2). The SVA was closed with a Gore-Tex patch on the aortic side and direct closure using 4-O prolene running sutures along the right atrial side. After successful surgery, the patient’s symptoms improved, and regular outpatient department follow-ups were conducted. DISCUSSION A recent review concerning the frequency of sinus and cardiac chamber involvement in aneurysm rupture has been published. According to a Mayo Clinic study and previous reviews (11 studies), aneurysms usually rupture into the RV (50-77%) or RA (37%), leading to aortocardiac fistulas, while the right coronary sinus aneurysms mostly (73%) ruptured into the RV.2 The Oriental population has a higher incidences of SVA orientation from the right coronary cuspid that ruptures into RV than western population. 5 These rare aneurysms are eventually diagnosed once they rupture, typically fistulazing into another cavity (pericardium, atrium, RV, or right outflow tract) and manifesting symptoms and Figure 2. Exposure of the ruptured windsock aneurysm, protruding into the right atrium (arrow), located at the lower right atrium (RA) just above the level of the tricuspid valve. Acta Cardiol Sin 2009;25:52-5 54 Ming-Shyan Lin et al. TV involvement if TEE is unavailable. SVA in RA along with a VSD were suspected. However, one long and large wind-sock SVA located at the atrial side near the TV junction, descending into the RV during the cardiac cycle, was finally confirmed. Tricuspid regurgitation is a serious consideration if there is TV involvement, and may increase the risk of endocarditis and the difficulty of surgical repair. CTA provides early diagnosis of SVA and precise location of the SVA before surgical evaluation. For example, in this study, CTA revealed that the SVA was located along the atrium near the junction of the TV without destruction or involvement of the TV. In time, CTA will be a perfect pre-operative tool for evaluating TV involvement and identifying the location of the rupture hole; however, if SVA is suspected, images of better quality focus around the TV can be obtained. To the best of our knowledge, there were only six cases of SVA presented with suspected jet flows into both chambers, due to bilateral rupture in three cases9-11 or alternating jet flows in others,12-14 from 1987 to 2008. Of the six cases, only two were acquired due to endocarditis; the others were congenital.9,11 In acquired aneurysms, secondary degeneration of the elastic connective tissue occurs as a result of atherosclerosis or infection. There are many interesting clinical features for cases with direct or indirect involvement of both chambers. SVA with echocardiographic features of dual jet flows into both chambers will be classified to two major types; one is direct dissection or rupture of the SVA into both chambers, the other is a long and large sac within one chamber, and protruding into the other. SVA is a rare congenital anomaly that requires early surgical correction following its diagnosis and recognition of typical heart failure signs after physical examination. The repair procedure for an unruptured SVA is individualized, and it has a high success rate and low mortality.15 In conclusion, this is an unusual case of SVA with interesting echocardiographic features since this SVA was a wind sac that swam between both chambers and was combined with an ASD that was undetected prior to surgery. CTA, or more recently, magnetic resonance imaging could provide sufficient additional information about aneurysm location, communicating chambers, and REFERENCES 1. Sakakibara S, Konno S. Congenital aneurysm of the sinus of Valsalva: anatomy and classification. Am Heart J 1962;63:40524. 2. Moustafa S, Mookadam F, Cooper L, et al. Sinus of Valsalva aneurysms: 47 years of a single center experience and systematic overview of published reports. Am J Cardiol 2007;99:1159-64. 3. Wang ZJ, Fan QX, Zou CW, et al. Clinical analysis for 70 sinus of Valsalva aneurysm. Zhonghua Wai Ke Za Zhi 2004;42:808-11. 4. Sundeen JT, Bloom S. Sinus of Valsalva aneurysm associated with multiple conotruncal congenital malformations. Hum Pathol 1987;18:96-9. 5. Chu SH, Hung CR, How SS, et al. Ruptured aneurysms of the sinus of Valsalva in Oriental patients. J Thorac Cardiovasc Surg 1990;99:288-98. 6. Feldman DN, Roman MJ. Aneurysms of the sinuses of Valsalva. Cardiology 2006;106:73-81. 7. Smith RL, Irimpen A, Helmcke FR, et al. Ruptured congenital sinus of Valsalva aneurysm. Echocardiography 2005;22:625-8. 8. Pasteuning WH, Roukema JA, van Straten AH, et al. Rapid hemodynamic deterioration because of acute rupture of an aneurysm of the sinus of Valsalva: the importance of echocardiography in early diagnosis. J Am Soc Echocardiogr 2002;15:1108. 9. Vereckei A, Vándor L, Halász J, et al. Infective endocarditis resulting in rupture of sinus of Valsalva with a rupture site communicating with both the right atrium and right ventricle. J Am Soc Echocardiogr 2004;17:995-7. 10. Przybojewski JZ, Blake RS, de Wet Lubbe JJ, et al. Rupture of sinus of Valsalva aneurysm into both right atrium and right ventricle. S Afr Med J 1983;63:616-25. 11. Feldman L, Friedlander J, Dillon R, et al. Aneurysm of right sinus of Valsalva with rupture into right atrium and into the right ventricle. Am Heart J 1956;51:314-24. 12. Kallis P, de Belder M, Smith EE. Rupture of a sinus of Valsalva aneurysm through the tricuspid septal leaflet. Ann Thorac Surg 1993;55:1247-8. 13. Anzai N, Yamada M, Tuchida K, et al. Rupture of an aneurysm of the aortic sinus of Valsalva into the right ventricle: a case presenting an unusual hemodynamic manifestation. Cardiology 1987; 74:147-50. 14. Lim ST, Lau KW, Ding ZP. An unusual case of ruptured aneurysm of sinus of Valsalva. Singapore Med J 1996;37:115-6. 15. Dong C, Wu QY, Tang Y. Ruptured sinus of Valsalva aneurysm: A Beijing experience. Ann Thorac Surg 2002;74:1621-4. 55 Acta Cardiol Sin 2009;25:52-5