Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
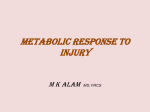
Case Challenge A 13-Year-Old Girl with Recurrent Inguinal Lymphadenopathy Francesca Del Bufalo, MD; Irene Salfa, MD; Valerio Pardi, MD; Giovanna Stefania Colafati, MD; Maria Antonietta De Ioris, MD, PhD; Rita De Vito, MD; and Andrea Finocchi, MD, PhD Francesca Del Bufalo, MD, is a Resident Physician, Department of Pediatric Hematology/Oncology, Bambino Gesù Children’s Hospital, IRCCS, and Pediatric Department, Tor Vergata University of Rome. Irene Salfa, MD, is a Resident Physician, Unit of Immunology and Infectious Disease, University Hospital Pediatric Department, Bambino Gesù Children’s Hospital, IRCCS, and Pediatric Department, Tor Vergata University of Rome. Valerio Pardi, MD, is a Pediatric Surgeon, Department of Surgery and Transplantation, Division of General Surgery, Bambino Gesù Children’s Hospital, IRCCS. Giovanna Stefania Colafati, MD, is a Pediatric Radiologist, Department of Neuroradiology, Bambino Gesù Children’s Hospital, IRCCS. Maria Antonietta De Ioris, MD, PhD, is a Pediatric Oncologist, Department of Pediatric Hematology/Oncology, Bambino Gesù Children’s Hospital, IRCCS. Rita De Vito, MD, is a Pediatric Pathologist, Department of Pathology, Bambino Gesù Children’s Hospital, IRCCS. Andrea Finocchi, MD, PhD, is Assistant Professor of Pediatrics, Unit of Immunology and Infectious Disease, University Hospital Pediatric Department, Bambino Gesù Children’s Hospital, IRCCS, and Pediatric Department, Tor Vergata University of Rome. Address correspondence to: Andrea Finocchi, MD, PhD, Unit of Immunology and Infectious Disease, University Hospital Department of Pediatrics, Children’s Hospital Bambino Gesù, and University of Rome Tor Vergata, Piazza Sant’Onofrio, 4 - 00165 Rome, Italy; email: andrea.finocchi@ uniroma2.it. Disclosure: The authors have no relevant financial relationships to disclose. doi: 10.3928/00904481-20140325-04 136 | Healio.com/Pediatrics A 13-year-old girl was referred to our hospital for diagnostic evaluation of recurrent inguinal lymphadenopathy. Eleven months before, she had been admitted to another institution with non-specific right inguinal lymphadenopathy associated with bi-monthly intermittent mild fever and hypochromic microcytic anemia, elevation of C-reactive protein (CRP), and hypergammaglobulinemia at blood screen. After excluding infectious causes by blood exams, diagnostic lymph nodal excisional biopsy was performed to exclude malignant etiologies. Histological examination showed nonspecific lymphoid hyperplasia, and the girl was discharged with the diagnosis of non-specific lymphadenopathy and irondeficiency anemia, with prescription of iron supplements. During the following months, follow-up blood exams showed persistence of anemia. At admission to our institution, the physical examination was unremarkable except for the presence of a mass in the inner upper aspect of the right thigh. An accurate history revealed that the mass had reappeared soon after the biopsy; the lesion was below the biopsy area and had enlarged slowly during the course of 10 months. It did not show any inflammatory signs (calor, dolor, rubor, or loss of function); had a solid, woody consistency; and was not movable. During the hospital stay, initial diagnostic workup confirmed persistence of microcytic anemia — interpreted as anemia of chronic disease — elevation of CRP and erythrocyte sedimentation rate (ESR) and hypergammaglobulinemia (Table 1). Considering the elevated inflammatory markers, antibiotic therapy was started. Nevertheless, all of the extensive microbiological tests performed both on blood and on bone marrow were negative. Indeed, an underlying infectious disease was excluded (Table 1). Auto-inflammatory causes and autoimmune diseases responsible for recurrent lymphadenopathy were also excluded because serum auto-antibodies screening results were negative (Table 1). An inguinal ultrasound scan revealed the presence of a 4 × 3 × 4 cm oval lesion in the internal upper side of the right thigh. The edges of the mass appeared to be well-defined, and it was predominantly For diagnosis, see page 137 Editor’s note: Each month, this department features a discussion of an unusual diagnosis in areas including genetics, radiology, or dermatology. A description and images are presented, followed by the diagnosis and an explanation of how the diagnosis was determined. As always, your comments are welcome via email at [email protected]. PEDIATRIC ANNALS 43:4 | APRIL 2014 Case Challenge solid, with vascular areas containing semi-solid material (Figure 1A). An ultrasound scan also showed lymph nodes with reactive aspect. A malignant disease or Castleman disease was suspected. A larger biopsy including both the mass and a closer lymph node was performed, revealing a moderate infiltration of the mass into deep tissues. Both specimens were sent for histopathologic examination,which showed a polymorphous proliferation of spindlecells with voluminous mononucleated cells, lympho-histiocytic elements, and a moderate inflammatory infiltrate; an abundant myxoid stroma was also described. Immunohistochemistry revealed mild cytoplasmic staining for anaplastic lymphoma kinase and actin, as well as mild proliferation index with MIB-1. Histopathologic examination showed a reactive lymph adenitis, as well, probably related to the mass. Diagnosis: Inflammatory Myofibroblastic Tumor DISCUSSION The evaluation of the child with inguinal lymphadenopathy (LA) is a common scenario for the pediatrician. Most cases result from benign and self-limiting diseases and resolve without any consequences. However, sometimes it can be a result of the manifestation of a serious systemic disease; in these cases, prompt identification and diagnosis is mandatory.1 The patient was admitted for a recurrent inguinal LA diagnosis with a 1-year history. The clinical history suggested an indolent but progressive disease. A careful history and physical examination indicated that the mass appeared shortly after a lymph node biopsy, just below the area of the biospy. Physical examination led us to the suspicion that the mass did not represent a relapse of the inguinal LA, PEDIATRIC ANNALS 43:4 | APRIL 2014 TABLE 1. Summary of Diagnostic Work-Up Admission 1st Follow-Up After Resection Normal Reference Range 4.34 106/mm3 5.59 > 106/mm3 3.90 - 4.90 106/mm3 Hemoglobin (HB) 7.9 g/dL 13.1 g/dL 12-16 g/dL Hematocrit (HT) 27.9% 42.5% 36%-49% Test Red blood cell (RBC) Mean corpuscular volume (MCV) 64.3 fL 76.1 fL 75-98 fL Platlet (PLT) 562 103/mm3 326 103/mm3 150-450 103/mm3 C-reactive protein (CRP) 12.19 mg/dL 0.09 mg/dL 0-0.50 mg/dL 68 mm N.A 0-15 mm Serum iron 7 mcg/dL N.A. 50-170 mcg/dL Ferritin 99 ng/mL N.A. 9-290 ng/mL Erythrocyte sedimentation rate (ESR) Transferrin 164 mg/dL N.A. 200-360 mg/dL Immunoglobulin G (IgG) 2,910 mg/dL N.A. 700-1,600 mg/dL Immunoglobulin A (IgA) 356 mg/dL N.A. 70-400 mg/dL Immunoglobulin M (IgM) 215 mg/dL N.A. 40-230 mg/dL Cytomegalovirus (CMV) serology Negative N.A. Epstein-Barr virus (EBV) PCR Negative N.A. Leishmania PCR and serology Negative N.A. Toxoplasma gondii serology Negative N.A. HIV serology Negative N.A. Parvovirus B19 PCR Negative N.A. Mycobacterium tubercolosis interferon-gamma release assay Negative (3 samples) N.A. Bartonella serology Negative N.A. Antinuclear antibody (ANA) Negative N.A. Anti-neutrophil cytoplasmatic antibody (ANCA) Negative N.A. N.A. = not applicable; PCR = polymerase chain reaction. but rather a neoformation ex novo, which was subsequently confirmed by histological examination. Inflammatory myofibroblastic tumor (IMT) is an uncommon, mesenchymal, low-malignancy potential neoplasm characterized by proliferating myofibroblasts that typically present as a mass in children and young adults. The most commonly involved visceral site is the lung, although many extrapulmonary sites are also recognized; soft tissue localization is exceptionally rare.2 IMT clinical manifestation and symptoms range from abdominal pain, intestinal obstruction, urinary symptoms, and a pal- pable mass for abdominal IMT, to mild to severe respiratory symptoms for intrapulmonary lesions.3,4 Soft-tissue lesions usually manifest with a mass with locally aggressive features that make differential diagnosis with malignant neoplasms difficult; little attention has been paid in literature to IMTs of the extremities.5 The important inflammatory component leads to confounding systemic symptoms such as unexplained fever, weight loss, weakness, pallor, as well as to laboratory findings including microcytic anaemia refractory to iron therapy, thrombocytosis, hypergammaglobulinemia, and Healio.com/Pediatrics | 137 Case Challenge Image courtesy of Andrea Finocchi, MD, PhD. Distant metastases have been reported to occur occasionally, mostly in patients with abdominal tumors. Histological predictors of aggressive behavior in IMTs have been largely investigated without much success.10 Figure 1. The sonographic scan (a) shows a mass at the level of internal upper side of the right thigh with inhomogeneous structure, solid and fluid. Magnetic resonance axial (MRA) T2-weighted turbo spin echo (TSE) image (b) shows inhomogeneous mass in the soft tissues (black arrow) with close relationship with blood vessels. MRA TSE T1-weighted images (d) on the same plane show an intermediate-high signal intensity of the mass, consistent with hemorrhagic infarction. Moreover, coronal T1-weighted image with fat-suppression after gadolinium administration (c) depicts longitudinal extension and shows enhancement of the solid component of the lesion (white arrow); notice the presence of enlarged ipsilateral inguinal lymph nodes. increased inflammatory markers, mimicking other systemic or neoplastic processes.6 The clinical presentation of our patient was made more confusing by the previous lymphadenopathy and lymph node excisional biopsy, which revealed a non-specific lymphoid hyperplasia. We believe that this finding represented a reactive process to the relevant inflammatory component of the tumor that was developing but not macroscopically visible yet. To our knowledge, recurrent and preceding lymphadenopathy has never been described as presenting sign of IMT. Although the etiology of IMTs is unknown, association with minor trauma, surgery, infections, and/or other diseases of the immune system, as reported from Alaggio and colleagues,4 suggests an inflammatory origin of the disease. The treatment of choice for IMTs is surgical excision. In the present case, after estimating the extension and infiltration of the mass by MRI (Figures 1B138 | Healio.com/Pediatrics 1D), in accordance with the surgeons and the oncologists, radical surgical resection was successfully carried out. Treatment with chemotherapy or radiotherapy is controversial because of the variable response reported.7 Occasionally, treatment with steroids or non-steroidal anti-inflammatory therapy have been reported.8 The prognosis of IMTs remains unpredictable, and as such, these tumors have been categorized as tumors of intermediate biological potential by the most recent World Health Organization classification.9 Most IMTs follow a nonrecurring clinical course after complete surgical excision, but clinical behavior of IMTs can be locally aggressive with local recurrence in case of partial resection. Currently, the girl is in good clinical condition. The anemia rapidly resolved after surgical resection without further iron supplements, and CRP and gammaglobulin count also normalized (Table 1). CONCLUSIONS In consideration of the intermediate malignant potential and of the multiform clinical presentation of IMTs, we believe that pediatricians should be aware of this entity and should consider it in the differential diagnosis of a soft-tissue lesion associated with recurrent local lymphadenopathy and/ or inflammatory symptoms. REFERENCES 1. Knight PJ, Mulne AF, Vassy LE. When is lymph node biopsy indicated in children with enlarged peripheral nodes? Pediatrics. 1982;69:391-396. 2.Kovach SJ, Fischer AC, Katzman PJ, Salloum RM, Ettinghausen SE, Madeb R, Koniaris LG. Inflammatory myofibroblastic tumors. J Surg Oncol. 2006;94:385-391. 3.Stinger MD, Ramani P, Yeung CK, et al. Abdominal inflammatory myofibroblastic tumors in children. Br J Surg. 1992;79:1357-1360. 4.Alaggio R, Cecchetto G, Bisogno G, et al. Inflammatory myofibroblastic tumors in childhood: a report from the Italian Cooperative Group studies. Cancer. 2010;116:216-226. 5. Masciocchi C, Lanni G, Conti L, et al. Soft-tissue inflammatory myofibroblastic tumors (IMTs) of the limbs: potential and limits of diagnostic imaging. Skeletal Radiol. 2012;41:643-649. 6.Patnana M, Sevrukov AB, Elsayes KM, et al. Inflammatory pseudotumor: the great mimicker. Am J Roentgenol. 2012;198:W217-227. 7.Chun YS, Wang L, Nascimento AG, Moir CR, Rodeberg DA. Inflammatory myofibroblastic tumor: anaplastic lymphoma kinase (ALK) expression and prognosis. Pediatr Blood Cancer. 2005;45:796-801. 8.Su W, Ko A, O’Connell T, Applebaum H. Treatment of pseudotumors with nonsteroidal antiinflammatory drugs. J Pediatr Surg. 2000;35:1635-1637. 9.Coffin CM, Fletcher JA. Inflammatory myofibroblastic tumor. In: Fletcher CDM, Unni KK, Mertens F, eds. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon: IARC Press; 2002:91-93 10.Gleason BC, Hornick JL. Inflammatory myofibroblastic tumours: where are we now? J Clin Pathol. 2008;61:428-437. PEDIATRIC ANNALS 43:4 | APRIL 2014