Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
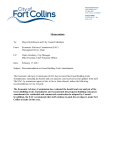
Successful TCR-Based Immunotherapy for Autoimmune Myocarditis with DNA Vaccines After Rapid Identification of Pathogenic TCR This information is current as of August 12, 2017. Subscription Permissions Email Alerts J Immunol 2000; 164:2248-2254; ; doi: 10.4049/jimmunol.164.4.2248 http://www.jimmunol.org/content/164/4/2248 This article cites 19 articles, 11 of which you can access for free at: http://www.jimmunol.org/content/164/4/2248.full#ref-list-1 Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2000 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 References Yoh Matsumoto, Youngheun Jee and Mayumi Sugisaki Successful TCR-Based Immunotherapy for Autoimmune Myocarditis with DNA Vaccines After Rapid Identification of Pathogenic TCR1 Yoh Matsumoto, Youngheun Jee, and Mayumi Sugisaki E xperimental organ-specific autoimmune diseases can be induced in animals by immunization with organ-specific autoantigens and serves as a model for human autoimmune diseases. Recent analysis mainly using experimental autoimmune encephalomyelitis (EAE)3 indicates that autoimmune disease-inducing T cells bear CD4 molecules and use a limited number of ␣- and -chains of the TCR (1, 2). Furthermore, the complementarity-determining region 3 (CDR3) of TCR of in vitroestablished encephalitogenic T cell clones is rather short, and some amino acid residues are conservatively preserved (3, 4). We have recently demonstrated by CDR3 spectratyping that only V8.2 spectratype shows oligoclonal expansion in the spinal cord throughout the course of EAE induced in Lewis rats, whereas irrelevant TCRs become more diverse at later stages of the disease (5, 6). Importantly, the CDR3 sequence of the majority of clones derived from EAE-specific spectratype is the same as that of encephalitogenic T cell clones. These findings imply that although the phenotype of T cells in the target organ diversifies as the autoimmune disease progresses, disease-associated TCR spectratype(s) are preserved throughout the course of the disease. Thus, CDR3 spectratyping is a powerful tool for the screening of autoimmune disease-inducing T cells whose pathomechanism is poorly known. Department of Molecular Neuropathology, Tokyo Metropolitan Institute for Neuroscience, Fuchu, Tokyo, Japan Received for publication October 4, 1999. Accepted for publication December 9, 1999. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 This study was supported in part by grants-in-aid (10357005, 09480216, and 09670682) from the Ministry of Education, Japan. Y.J. was supported by the research subsidy of Japan Foundation for Neuroscience and Mental Health. 2 Address correspondence and reprint requests to Dr. Yoh Matsumoto, Department of Molecular Neuropathology, Tokyo Metropolitan Institute for Neuroscience, Musashidai 2-6 Fuchu, Tokyo 183-8526, Japan. E-mail address: [email protected] 3 Abbreviations used in this paper: EAE, experimental autoimmune encephalitis; EAC, experimental autoimmune carditis; CDR, complementarity-determining region; CNBr, cyanogen bromide; PI, postimmunization. Copyright © 2000 by The American Association of Immunologists In some types of organ-specific autoimmune diseases such as experimental autoimmune myocarditis (EAC), it is difficult to establish autoantigen-reactive disease-inducing T cell lines and clones. Like EAE, EAC is inducible in Lewis rats by immunization with cardiac myosin (7, 8) or adoptive transfer of sensitized T cells activated in vitro with Con A (9). Therefore, EAC is judged to be a T cell-mediated autoimmune disease. However, so far, attempts to establish cardiac myosin-reactive carditogenic T cells using cyanogen bromide (CNBr)-treated soluble myosin have been unsuccessful (our unpublished observation). These findings suggest that carditogenic epitope(s) resides in the cleavage site of CNBr. In such a case, it is impossible to identify disease-inducing TCR by determining the TCR phenotype of in vitro-established carditogenic T cell clones. In the present study, we have extended our strategy to identify EAC-inducing TCRs on the basis of the findings obtained with the EAE system by direct analysis of heart-infiltrating T cells. For this purpose, candidate TCR -chain genes were screened by CDR3 spectratyping and the sequence of their CDR3 region was determined after cloning. Then immunotherapy with V-specific mAbs was performed to see whether this treatment suppresses the development of EAC. Consequently, we found that combined immunotherapy with anti-V8.2 plus V10 mAbs, but not with either alone, significantly reduced the histological severity of EAC and completely suppressed the inflammation in some animals. More important, essentially the same results were obtained using DNA vaccines encoding V8.2 and V10. Collectively, the determination of candidate TCR genes by CDR3 spectratyping and subsequent immunotherapy serves not only to elucidate the pathomechanism, but also to provide a systematic therapeutic strategy for T cell-mediated autoimmune diseases. Materials and Methods Rats and reagents Lewis rats were obtained from Seiwa (Fukuoka, Japan). All of the rats were used at the age of 8 –12 wk. The mAbs used in this study were R73 (antiTCR ␣) (10), R78 (anti-V8.2), B73 (anti-V8.5), G101 (anti-V10) (11), and HIS42 (anti-V16). R78, B73, and G101 were kindly provided 0022-1767/00/$02.00 Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 The identification of TCRs of autoimmune disease-inducing T cells within a short period of time is a key factor for designing TCR-based immunotherapy during the course of the disease. In this study, we show that experimental autoimmune carditisassociated TCRs, V8.2 and V10, were determined by complementarity-determining region 3 (CDR3)-spectratyping analysis and subsequent sequencing of the CDR3 region of spectratype-derived TCR clones. Immunotherapy targeting both V8.2 and V10 TCRs using mAbs and DNA vaccines significantly reduced the histological severity of experimental autoimmune carditis and completely suppressed the inflammation in some animals. Since depletion or suppression of one of two types of effector cells does not improve the severity of the disease significantly, combined TCR-based immunotherapy should be considered as a primary therapy for T cell-mediated autoimmune diseases. TCR-based immunotherapy after rapid identification of autoimmune diseaseassociated TCRs by CDR3 spectratyping can be applicable, not only to animal, but also to human autoimmune diseases whose pathomechanism is poorly understood. The Journal of Immunology, 2000, 164: 2248 –2254. The Journal of Immunology by Dr. T. Hünig (Würzburg, Germany). R73 and HIS42 were obtained from Serotec (Oxford, U.K.). Cardiac myosin preparation Cardiac myosin was partially purified according to the method of Perry (12) with a few modifications. Human heart kept at ⫺80°C was thawed, minced, and weighed. A total of 300 ml of chilled 0.3 M KCl-0.15 M sodium phosphate buffer (pH 6.5) was added to 100 g of minced heart tissue and kept on ice for 20 min. This homogenate was centrifuged at 5000 rpm for 20 min at 4°C, and the supernatant was collected by filtration through Toyo No. 2 filter paper (Toyo Roshi, Tokyo, Japan). The filtrate was then diluted with 15 volumes of chilled Mili-Q-filtered (Millipore Japan, Tokyo, Japan) purified water to aggregate myosin. Aggregated myosin was collected by centrifugation at 5000 rpm, dissolved in 0.5 M KCl, and stored at ⫺20°C with the same volume of glycerin. EAC induction and histological evaluation Flow cytometric analysis Under ether anesthesia, blood was aspirated via cardiac puncture and the heart and the popliteal lymph node were removed. Then PBL and heartinfiltrating T cells were isolated by the proteolytic enzyme treatment and density gradient method as described previously (14). Cells were incubated with one of the V-specific mAbs followed by PE-conjugated anti-mouse IgG (Biomeda, Foster City, CA). To saturate free binding sites of the secondary Ab, cells were incubated with normal mouse serum. Then FITCR73 (Serotec) was applied in the second step. Ten thousand cells were analyzed in each sample by FACScan (Becton Dickinson, Mountain View, CA) flow cytometry. In preliminary studies, it was shown that the profile of staining using irrelevant mAbs plus the secondary Ab or the secondary Ab alone was essentially the same as that of unstained controls. Therefore, Ab controls were omitted in subsequent analysis. cDNA synthesis and PCR amplification RNA was extracted from isolated heart-infiltrating T cells using RNazol B (Biotecx Laboratories, Houston, TX). cDNA was then synthesized by reverse transcription using a SuperScript Preamplification System (Life Technologies, Gaithersburg, MD) and amplified in a thermal cycler (Perkin-Elmer/Cetus, Norwalk, CT) using primer pairs for TCR. Primers for V1–20 were the same as those used previously (15). Two types of C primers, C outer (5⬘-TGTTTGTCTGCGATCTCTGC-3⬘) and C inner (5⬘-TCTGCTTCTGATGGCTCA-3⬘), were used in this study. They were labeled with Cy5 or rhodamine or remained unlabeled. CDR3 spectratyping and sequencing of spectratype-derived DNA CDR3 spectratyping was performed as described previously (16) with a few modifications. cDNA was amplified with V-specific and rhodaminelabeled C outer primers, and undiluted or diluted PCR products were added to an equal volume of formamide/dye loading buffer and heated at 94°C for 2 min. A total of 2 l of the samples was applied to a 6% acrylamide-sequencing gel. Gels were run at 30 W for 3 h and 30 min at 50°C. Then the fluorescence-labeled DNA profile on the gel was directly recorded using a FMBIO fluorescence image analyzer (Hitachi, Yokohama, Japan). cDNA extracted from spectratypes of interest on the acrylamide gel was reamplified with V and unlabeled C inner primers. Then PCR products were ligated into pT-Adv vector and cloned using the AdvanTAge PCR Cloning kit (Clontech Laboratories, Palo Alto, CA) according to the manufacturer’s instructions. The plasmid DNA was then sequenced using a Cy5-labeled C inner primer and Thermo Sequenase Fluorescent-labeled Primer Cycle sequencing kit on an ALFexpress DNA sequencer (Pharmacia Biotech, Tokyo, Japan). CDR3 length is defined as the region starting from the amino acid residue after the CASS sequence of most V segments and ending before the GXG box in the J region as described previously (17). In vivo administration of mAbs Protein G-purified R78, G101, or both mAbs at a dose of 100 g was injected i.p. once a day for 21 consecutive days from day ⫺7 to ⫹14 postimmunization except on the day of challenge. DNA vaccination DNA vaccine therapy was performed as reported previously with modifications (18). Total RNA was extracted from normal rat PBL and reverse transcribed into cDNA. This cDNA was then amplified using Amplitaq Gold (Perkin-Elmer/Cetus) with one of primers specific for V8.2 (5⬘CAAAACACATGGAAGCTGCAG-3⬘), V10 (5⬘-TTATGAGCTATAG GCTCCTAAGCTGTGTGG-3⬘) or V12 (5⬘-AAATGGGCATCCAGA CCCTCTGTTGTATGA-3⬘) and C inner primer. All of the forward primers were designed to include an ATG in-frame. PCR products were cloned into pTargeT plasmid (Promega, Madison, WI) according to the manufacturer’s instructions. Colonies grown in competent cells were picked and recombinant plasmid DNA was isolated using Mini prep (Promega). By restriction enzyme digestion with PstI, colonies with an insert with right direction and length were screened, and the nucleotide sequence of each clone was determined to confirm that inserts had the right sequence with ATG in-frame. Large-scale preparation of plasmid DNA was done using Mega prep (Promega). For DNA vaccination, animals were pretreated with 0.75% bupivacaine (1 l/g body weight; Sigma) by injecting it into tibialis anterior muscle 1 wk before vaccination. Then 100 g of DNA was injected into the same site according to the indicated protocol. Two weeks after the last vaccination, rats were challenged with human cardiac myosin emulsified in CFA. To verify the expression of RNA and protein, the muscle tissue was removed from the injected site after extensive perfusion with PBS, and RNA and protein extracts were prepared. Using a forward primer specific for the plasmid sequence upstream to the insert and C inner primer, we identified that transcripts corresponding to the plasmid sequence plus insert existed in the muscle. We also verified the presence of the TCR protein by Western blot analysis (data not shown). Results Histological and flow cytometric analysis of EAC Lewis rats were immunized with human cardiac myosin in CFA along with an i.p. injection of pertussis toxin. At various time points, the heart was removed under ether anesthesia and processed for histological examination. At the early stage of EAC, mononuclear cells which mainly consisted of TCR␣⫹ T cells and macrophages infiltrated the outer one-third of the muscle. In severe cases, there was extensive necrosis of muscle fibers (Fig. 1A). Multinucleated giant cells were occasionally seen in the lesion (arrows in Fig. 1A) as reported previously (8). Using hematoxylin and eosin-stained sections, the histological severity of the disease during the course was scored (Fig. 1B). Inflammatory lesions appeared at around day 7 postimmunization (PI), increased in severity gradually, and reached a maximal level on day 12 PI. The severity of inflammation remained unchanged during the examination period until day 20 PI (Fig. 1B). We next examined the TCR V phenotype of infiltrating T cells by flow cytometry with currently available anti-V mAbs (Fig. 1C ). The percentages of V8.2, V8.5, V10, and V16 in lymph Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 EAC was induced in Lewis rats as described previously (7) with modifications. Each rat was immunized in the hind footpads on both sides with an emulsion containing 1.5 mg of cardiac myosin in CFA (Mycobacterium tuberculosis H37Ra, 5 mg/ml) along with an i.p. injection of 2 g pertussis toxin (Sigma, St. Louis, MO). Immunized rats were weighed and observed daily. EAC lesions were evaluated using hematoxylin and eosin-stained sections according to the following criteria: grade 1, focal inflammatory lesions mainly located in the outer layer of the cardiac muscle; grade 2, diffuse inflammation involving the outer layer of the muscle; grade 3, grade 2 plus focal transmural inflammation; and grade 4, diffuse inflammation with partial necrosis. A single immunoperoxidase staining was performed using mAbs against TCR ␣ (R73), V8.2 (R78), V8.5 (B73), and V10 (G101) (11) as described previously (13). Briefly, frozen sections of the heart were air dried and fixed in ether for 10 min. After incubation with normal horse serum, sections were allowed to react with mAb, biotinylated horse antimouse IgG (Vector Laboratories, Burlingame, CA), and HRP-labeled Vectstain Elite ABC kit (Vector Laboratories). HRP binding sites were detected in 0.005% diaminobenzidine and 0.01% hydrogen peroxide. 2249 DNA VACCINE THERAPY FOR AUTOIMMUNE MYOCARDITIS 2250 Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 The Journal of Immunology 2251 nodes, PBL, pericardial effusion, and heart were determined and proportions to total T cells were calculated (numbers in parentheses). The percentages of Vs in lymph nodes and PBL were essentially the same as those in normal controls which were reported previously (15). Moreover, there was no preferential infiltration of T cells bearing a particular type of V in the target organ. CDR3-spectratyping analysis of heart-infiltrating T cells Nucleotide sequence of the CDR3 region of oligoclonally expanded spectratypes Based on findings obtained by CDR3 spectratyping, bands representing candidate spectratypes were cut out from the gel and extracted cDNA was reamplified by nested PCR. PCR products were then cloned and the nucleotide sequences of the clones were determined. The results are listed in Tables 1 and 2. With regard to V8.2, DSSYEQYF, which is a predominant sequence in EAE, was also recognized in 50% of clones on day 8 PI (Table I). However, CDR3 sequences of the clones from V8.2 spectratype became diverse at a later stage (Table I). V12 spectratype showed diverse CDR3 sequences (data not shown). In sharp contrast, sequencing analysis of V10 revealed a very striking finding. As shown in Table II, all of the clones isolated from V10 on day 8 PI possessed the sequence ERTDERLFF (Table II), and 85.7% of V10 on day 14 PI showed this sequence (Table II). These findings suggest that V8.2 and V10, rather than V12, are more likely effector TCRs because they have unique sequences in their CDR3 region. Immunotherapy of autoimmune carditis with mAbs and DNA vaccines We finally tested whether TCR-based immunotherapy with mAbs and DNA vaccines is effective for suppression of EAC. Purified mAbs against candidate TCRs, R78 (anti-V8.2) or G101 (antiV10) or both, were administered to rats by i.p. injections for 21 FIGURE 2. CDR3 spectratyping of heart-infiltrating T cells on days 8 (A) and 14 (B). On day 8, oligoclonal expansion of spectratypes with a short CDR3 was noted in V8.2 and V10 (indicated by arrow and arrowhead in A, respectively). However, on day 14, there was additional expansion in V10 and V12 (open arrow and double arrowhead in B, respectively). consecutive days starting from day ⫺7, i.e., 7 days before the immunization. On day 0, rats were immunized with human cardiac myosin, and heart pathology was examined on day 14 PI. The results are summarized in Table III. R78 treatment alone did not alter the severity of EAC (Table III, group A). G101 suppressed FIGURE 1. Histological and flow cytometric analysis of inflammatory lesions in the heart during EAC. Upon immunization with cardiac myosin, rats developed severe inflammatory lesions mainly comprising mononuclear cells with focal necrosis. In severe cases, there was extensive necrosis of muscle fibers (A). Residual muscle fibers and multinucleated giant cells are indicated by arrowheads and arrows, respectively. Histological grading of the lesions at various time points revealed that inflammatory lesions developed around day 6 PI, reached a plateau phase on day 12 PI, and persisted throughout the examination period (B). Standard errors are within 10% of the mean values at each time point. Flow cytometric analysis of inflammatory cells isolated from the heart during EAC revealed that no predominant V usage was detected using currently available anti-V-specific mAbs (anti-V8.2, V8.5, V10, and V16) (C). Numbers in parentheses indicate percentages of particular V-positive cells in the total TCR ␣-positive cells. Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 To identify oligoclonal expansion of TCRs with a particular CDR3 size, CDR3-spectratyping analysis was performed using heart-infiltrating T cells isolated at different times during EAC. In previous studies, we have shown that EAE-specific spectratype has several characteristics (5). First, clonal expansion of EAE-specific spectratype is observed throughout the course of the disease, whereas expansion of irreverent spectratypes is detectable only over a short period. Second, EAE-specific spectratype has a short CDR3. Finally, a predominant CDR3 sequence is found in EAE-specific spectratype throughout the disease course. On the basis of these criteria, we searched for EAC-specific spectratypes and representative results are shown in Fig. 2. At the early stage of EAC (day 8 PI), oligoclonal expansion was noted in V8.2 (arrow in Fig. 2A) and V10 (arrowhead in Fig. 2A) spectratypes. Expansion of V8.2 and V10 was also detectable at a later stage (day 14 PI) (arrow and arrowhead in Fig. 2B) when the histological severity was maximal (Fig. 1B). In addition, V12 was oligoclonally expanded at this stage (double arrowhead in Fig. 2B). Thus, CDR3spectratyping analysis suggests that three spectratypes, V8.2, V10, and V12, are candidates for EAC-inducing TCR. 2252 DNA VACCINE THERAPY FOR AUTOIMMUNE MYOCARDITIS Table I. Amino acid and nucleotide sequences of the CDR3 region of TCR clones extracted from V8.2 spectratype showing oligoclonal expansion in EACa V 2190H: EAC day 8, V8.2 CASS CASG CASS 2196H: EAC day 14, V8.2 CASS CASS CASS CASS CASG Frequency D gac G ggt N aat S agc S tct S tct S tcc G gga G gga Y tat N aat N aat E gag V gtg V gtg Q cag L ctc L ctc Y tat Y tat Y tat F ttc F ttt F ttt N aat D gac A ggc S tct L ctt D gac S tct S tcg S agc S tct S tct S agc G gga G ggg S tcc G gga G gga S tcc N aat G ggt Y tat N aat N aat Y tat V gtg E gag E gag V gtg V gtg E gat L ctc Q cag Q cag L ctc L ctc Q cag Y tat Y tat Y tat Y tat Y tat Y tat F ttt F ttc F ttc F ttt F ttt F ttc GPG 3/6 (50.0%) GEG 2/6 (33.3%) GEG 1/6 (16.7%) GEG 2/7 (28.6%) GPG 1/7 (14.3%) GPG 1/7 (14.3%) GEG 1/7 (14.3%) GEG 1/7 (14.3%) GAG 1/7 (14.3%) a CDR3 spectratyping was performed using PCR products amplified with TCR V1-20-specific primers. cDNA was extracted from bands showing oligoclonal expansion and reamplified by nested PCR, cloned, and sequenced. inflammation in the heart to some extent but the difference between test and control groups (groups B and D) was statistically insignificant. Combination therapy with R78 and G101 significantly reduced the severity of EAC and completely suppressed inflammation in two of four rats examined (Table III, group C). We also examined the effects of DNA vaccination on the development of EAC (Table IV). Plasmid DNA encoding V8.2, V10, or V8.2 plus V10 was injected i.m. twice and challenged for EAC. V8.2 DNA vaccination was ineffective (Table IV, group A). V10 DNA reduced the histological severity slightly compared with that of the control (group D, empty vector) but the difference was not significantly different. In contrast, combination therapy using V8.2 and V10 DNA significantly reduced the incidence and histological severity (group C). These findings indicate that both V8.2 and V10 screened by CDR3-spectratyping analysis are pathogenic TCRs and that TCR-based immunotherapy, especially using DNA vaccines, is effective for the treatment of T cell-mediated autoimmune diseases. Discussion In the present study, we analyzed EAC to verify EAC-inducing TCRs and to establish TCR-based immunotherapy. EAC is inducible in Lewis rats by immunization with human cardiac myosin as reported previously (7, 8). Since injection of activated T cells that had been taken from immunized animals and then stimulated in vitro with Con A induced severe carditis in naive rats (9), EAC is judged to be a T cell-mediated autoimmune disease. However, attempts so far have been unsuccessful in establishing cardiac myosin-reactive carditogenic T cells using CNBr-treated soluble myosin (our unpublished observation). These findings imply that carditogenic epitope(s) resides in the cleavage site of CNBr. As such, it would be difficult to identify disease-inducing TCRs by establishing disease-inducing T cell clones and subsequently determining their TCRs. Alternatively, we tried to identify EACspecific TCRs using heart-infiltrating T cells by CDR3 spectratyping and subsequent sequencing of the CDR3 region of oligoclonally expanded spectratypes. As reported previously (5), it was revealed in EAE that TCRs of T cells in the spinal cord show oligoclonal expansion of V8.2 spectratype throughout the course of the disease and that the majority of clones (⬃70% regardless of the stage examined) possess an identical sequence which is the same as that of the encephalitogenic T cell clone. On the basis of these criteria, we screened the spectratype pattern of TCRs isolated from heart-infiltrating T cells and found that V8.2, V10, and V12 spectratypes showed oligoclonal expansion (Fig. 2). To our surprise, virtually all of the clones (100% at the early stage and Table II. Amino acid and nucleotide sequences of the CDR3 region of TCR clones extracted from V10 spectratype showing oligoclonal expansion in EAC V 2190H: EAC day 8, V10 CASS 2196H: EAC day 14, V10 CASS CASS (N)D(N) Frequency E gag R agg T acg D gat E gaa R aga L ttg F ttt F ttc GHG 9/9 (100%) E gag V gtc R agg G gga T acg P ccg D gat R cgg E gaa D gac R aga T acc L ttg L ttg F ttt F ttc F ttc F ttc GHG 6/7 (85.7%) GAG 1/7 (14.3%) Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 CASS (N)D(N) The Journal of Immunology 2253 Table III. Immunotherapy of EAC with mAbsa mAb Specificity Incidenceb Heart weight (g) Histological Grade R78 G101 R78 ⫹ G101 Saline Anti-V8.2 Anti-V10 3/3 4/4 2/4 3/3 1.3 ⫾ 0.2 1.2 ⫾ 0.3 0.8 ⫾ 0.1c 1.4 ⫾ 0.3 3.7 ⫾ 0.2 2.6 ⫾ 0.9 0.8 ⫾ 0.8d 3.2 ⫾ 0.2 Group A B C D a Purified mAbs at a dose of 100 g or saline were administered i.p. once a day for 21 consecutive days starting from day ⫺7 of immunization. On day 0, rats were immunized with human cardiac myosin in CFA in bilateral footpads along with an i.p. injection of pertussis toxin. b No. of rats with cardiac inflammation/no. of rats examined. c Significantly different from groups A ( p ⫽ 0.006), B ( p ⫽ 0.045), and D ( p ⫽ 0.012) by Student’s t test. d Significantly different from groups A ( p ⫽ 0.002), B ( p ⫽ 0.024), and D ( p ⫽ 0.004) by Student’s t test. Table IV. Immunotherapy of EAC with DNA vaccinesa Group A B C D DNA V8.2 V10 V8.2 ⫹ V10 Empty vector Incidence Heart weight (g) Histological Grade 4/4 3/4 2/4 4/4 1.1 ⫾ 0.2 1.1 ⫾ 0.2 0.9 ⫾ 0.3 1.3 ⫾ 0.3 3.0 ⫾ 0.7 2.3 ⫾ 1.3 0.9 ⫾ 0.9b 3.0 ⫾ 1.1 a Lewis rats were pretreated by injection of 0.75% bupivacaine (1 l/g body weight) in the tibialis anterior muscle and 100 g in 50 l of DNA was injected twice at 2-wk intervals and challenged for EAC. On day 14 PI, hearts were removed and processed for hematoxylin and eosin staining. Histological severity was evaluated according to the criteria described in Materials and Methods. b Significantly different from groups A ( p ⫽ 0.01) and D ( p ⫽ 0.03) by unpaired Student’s t test. treatment with mAbs for 21 consecutive days. More important, potential side effects of xenoantibody administration can be avoided by this method. Treatment experiments using mAbs and DNA vaccines clearly indicate that both T cells bearing either V8.2 or V10 are EAC-inducing T cells. Since depletion or suppression of one of two types of effector cells does not improve the severity of the disease significantly, combined TCR-based immunotherapy should be considered as a primary therapy for T cellmediated autoimmune diseases. In the present study, we have shown that rapid identification of pathogenic TCRs by CDR3 spectratyping and CDR3 sequencing gives useful information for designing TCR-based immunotherapy without the culture procedures. The strategy employed in the present study provides insights into the pathomechanism of, but also provides a systematic therapeutic strategy for, human autoimmune diseases. Acknowledgments We thank Dr. Hünig (Würzberg) for kindly providing us with mAbs. We also thank Y. Kawazoe, K. Kohyama, and K. Nomura for technical assistance. References 1. Burns, J., A. Rosenzweig, B. Zweiman, A. Moskovitz, and R. Lisak. 1984. Recovery of myelin basic protein reactive T cells from spinal cords of Lewis rats with autoimmune encephalomyelitis. J. Immunol. 132:2690. 2. Acha-Orbea, H., D. J. Mitchell, L. Timmermann, D. C. Wraith, G. S. Tausch, M. K. Waldor, S. S. Zamvil, H. O. McDevitt, and L. Steinman. 1988. Limited heterogeneity of T cell receptors from lymphocytes mediating autoimmune encephalomyelitis allows specific immune intervention. Cell 54:263. 3. Gold, D. P., H. Offner, D. Sun, S. Wiley, A. A. Vandenbark, and D. B. Wilson. 1991. Analysis of T cell receptor  chains in Lewis rats with experimental allergic encephalomyelitis: conserved complementarity determining region 3. J. Exp. Med. 174:1467. 4. Zhang, X., and E. Heber-Katz. 1992. T cell receptor sequences from encephalitogenic T cells in adult Lewis rats suggest an early ontogenic origin. J. Immunol. 148:746. 5. Kim, G., N. Tanuma, T. Kojima, K. Kohyama, Y. Suzuki, Y. Kawazoe, and Y. Matsumoto. 1998. CDR3 size spectratyping and sequencing of spectratypederived T cell receptor of spinal cord T cells in autoimmune encephalomyelitis. J. Immunol. 160:509. 6. Kim, G., K. Kohyama, N. Tanuma, H. Arimoto, and Y. Matsumoto. 1998. Persistent expression of autoimmune encephalomyelitis (EAE)-specific V8.2 TCR spectratype in the central nervous system of rats with chronic relapsing EAE. J. Immunol. 161:6993. 7. Kodama, M., Y. Matsumoto, M. Fujiwara, F. Masani, T. Izumi, and A. Shibata. 1990. A novel experimental model of giant cell myocarditis induced in rats by immunization with cardiac myosin fraction. Clin. Immunol. Immunopathol. 57: 250. 8. Kodama, M., Y. Matsumoto, M. Fujiwara, S. Zhang, H. Hanawa, E. Itoh, T. Tsuda, T. Izumi, and A. Shibata. 1991. Characteristics of giant cells and factors related to the formation of giant cells in myocarditis. Circ. Res. 69:1042. 9. Kodama, M., Y. Matsumoto, and M. Fujiwara. 1992. In vivo lymphocyte-mediated myocardial injuries demonstrated by adoptive transfer of experimental autoimmune myocarditis. Circulation 85:1918. Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017 85.7% at the plateau stage of EAC) derived from V10 spectratype possessed an identical CDR3 region, i.e., ERTDERLFF (Table II), whereas V12 spectratypes were heterogeneous. V8.2 showed oligoclonal expansion only at the early stage (Table I). These findings strongly suggest that V10 and possibly V8.2 are carditogenic TCR V phenotypes. Since identification of EAC-associated TCRs by single-strand conformation polymorphism analysis was unsuccessful (19), CDR3 spectratyping is more suitable for the screening of autoimmune disease-associated TCR than singlestrand conformation polymorphism. Flow cytometric analysis of TCRs of T cells isolated from the peripheral blood and target organ is not always useful for the screening of autoimmune disease-associated T cells. Although the predominance of T cells bearing encephalitogenic TCR (V8.2) is observed in the spinal cord by this approach (15), that of V8.2 and V10 in the heart was not detectable in the present, as well as the previous (19), study. This discrepancy may be attributable to the difference in histopathology between EAC and EAE. Compared with EAE, T cells in the heart lesion are much fewer and the predominant population of inflammatory cells is macrophages. Therefore, it may be difficult to obtain a sufficient number of T cells from the lesion to show the predominance of a particular type of TCR. Finally, we performed treatment experiments with mAbs and DNA vaccines based on the data obtained by CDR3 spectratyping. Rats were treated with either anti-V8.2 or anti-V10 mAbs or both before and after the challenge for EAC. As nicely demonstrated in Table III, combined therapy with anti-V8.2 and antiV10 mAbs, but not with either alone, significantly suppressed autoimmune inflammation in the heart. Furthermore, essentially the same results were obtained using DNA vaccines (Table IV). Compared with mAb administration, DNA vaccination is an effective and easy therapeutic approach for the treatment of autoimmune diseases because remarkable suppressive effect was obtained by vaccination twice. This effect was almost the same as that after 2254 DNA VACCINE THERAPY FOR AUTOIMMUNE MYOCARDITIS 10. Hünig, T., H.-J. Wallny, J. K. Hartley, A. Lawetzky, and G. Tiefenthaler. 1989. A monoclonal antibody to a constant determinant of the rat T cell antigen receptor that induces T cell activation: differential reactivity with subsets of immature and mature T lymphocytes. J. Exp. Med. 169:73. 11. Torres-Nagel, N. E., D. P. Gold, and T. Hünig. 1993. Identification of rat TcrbV8.2, 8.5, and 10 gene products by monoclonal antibodies. Immunogenetics 37: 305. 12. Perry, S. V. 1955. Myosin adenosintriphosphatase. Methods Enzymol. 2:582. 13. Ohmori, K., Y. Hong, M. Fujiwara, and Y. Matsumoto. 1992. In situ demonstration of proliferating cells in the rat central nervous system during experimental autoimmune encephalomyelitis: evidence suggesting that most infiltrating T cells do not proliferate in the target organ. Lab. Invest. 66:54. 14. Tanuma, N., T. Kojima, T. Shin, Y. Aikawa, T. Kohji, Y. Ishihara, and Y. Matsumoto. 1997. Competitive PCR quantification of pro- and antiinflammatory cytokine mRNA in the central nervous system during autoimmune encephalomyelitis. J. Neuroimmunol. 73:197. 15. Tsuchida, M., Y. Matsumoto, H. Hirahara, H. Hanawa, K. Tomiyama, and T. Abo. 1993. Preferential distribution of V8.2-positive cells in the central nervous system of rats with myelin basic protein-induced autoimmune encephalomyelitis. Eur. J. Immunol. 23:2399. 16. Gorski, J., M. Yassai, X. Zhu, B. Kissella, C. Keever, and N. Flomenberg. 1994. Circulating T cell repertoire complexity in normal individuals and bone marrow recipients analyzed by CDR3 size spectratyping. J. Immunol. 152:5109. 17. Rock, E. P., P. R. Sibbald, M. M. Davis, and Y.-H. Chien. 1994. CDR3 length in antigen-specific immune receptors. J. Exp. Med. 179:323. 18. Waisman, A., P. Ruiz, D. L. Hirschberg, A. Gelman, J. R. Oksenberg, S. Brocke, F. Mor, I. R. Cohen, and L. Steinman. 1996. Suppressive vaccination with DNA encoding a variable region gene of the T-cell receptor prevents autoimmune encephalomyelitis and activates Th2 immunity. Nat. Med. 2:899. 19. Hanawa, H., T. Inomata, H. Sekikawa, T. Abo, M. Kodama, T. Izumi, and A. Shibata. 1996. Analysis of heart-infiltrating T-cell clonotypes in experimental autoimmune myocarditis. Circ. Res. 78:118. Downloaded from http://www.jimmunol.org/ by guest on August 12, 2017