Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Molecular mimicry wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
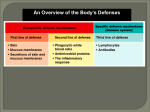
INNATE HOST DEFENSES CHAPTER 16 Patient suffering from advanced Leprosy Copyright © 2012 John Wiley & Sons, Inc. All rights reserved. If you have an infection you essentially always have a disease se 50% Fa l 50% Tr ue A. True B. False E.coli kills two girls in U.S. Pacific Northwest, boy hospitalized SEATTLE (Reuters) - Two young girls have died and a boy was hospitalized in critical condition in the Pacific Northwest on Wednesday after becoming infected with E.coli in two separate incidents, health officials said. Investigations have been launched into the source and strain of the bacteria that killed a 3-yearold girl in Lynden, Washington, and a 4-year-old girl, Serena Profitt, in Otis, Oregon. A third child, Bradley Sutton, 5, has also tested positive for E.coli and was being treated at Mary Bridge Children's Hospital in Tacoma, Washington, a hospital spokeswoman said. Possible sources of the E. coli infection include high-risk foods such as undercooked meat, unpasteurized milk or juices, restaurants at which cases have eaten, exposure to live animals and recreational water. Most of the multiple strains of E. coli are harmless or cause relatively brief illness but a few, including O157:H7, can cause severe illness and can lead to HUS, the Mayo Clinic said. H-7 O157 protein on cell wall The Trials of Stem Cell Therapy Edgar Irastorza was just 31 when his heart stopped beating in October 2008. He survived the heart attack, but the scar tissue that resulted cut his heart’s pumping ability by a third. He couldn’t pick up his children. He couldn’t dance. He fell asleep every night wondering if he would wake up in the morning. Desperation motivated Mr. Irastorza to volunteer for a highly unusual medical research trial: getting stem cells injected directly into his heart. Edgar Irastorza, who had stem cells injected into his heart after a major heart attack, was break-dancing again a few years after the procedure. As many as 4,500 clinical trials involving stem cells are underway in the United States to treat patients with heart disease, blindness, Parkinson’s, H.I.V., diabetes, blood cancers and spinal cord injuries, among other conditions. Initial studies suggest that stem cell therapy can be delivered safely, said Dr. Ellen Feigal, senior vice president of research and development at the California Institute of Regenerative Medicine, the state stem cell agency, which has awarded more than $2 billion toward stem cell research since 2006 and is enrolling patients in 10 clinical trials this year. Stem cells harvested from an embryo can turn into any of the body’s 200 cell types and, theoretically, live as long as the body does, unlike most cells. The basic idea of therapies using stem cells is simple: Inject them, for example, into a brain whose cells are dying, and replacement cells could presumably grow. The same would hold true for muscles, blood, organs and bone. In theory, stem cells can make repairs, lead to new growth and replace missing pieces. CHAPTER 16 INNATE HOST DEFENSES Innate host defenses- act against any type of invading organisms (as compared to specific host defenses which act against specific agents (antigens). Typically, nonspecific host defenses perform their function before specific body defense mechanisms are activated and include the following: 1. Physical barriers, such as skin and mucous membrane and the chemicals that they secrete 2. Chemical barriers, including antimicrobial substances in body fluids such as saliva, mucus, gastric juices and iron limiting mechanisms 3. Cellular defenses, consisting of certain cells that engulf (phagocytize) invading microorganisms 4. Inflammation, the reddening, swelling, and temperature increases in tissues at sites of infection 5. Fever, the elevation of body temperature to kill invading agents and/or inactivate their toxic products. 6. Molecular defenses, such as interferon and complement, that destroy or impede invading microbes. Adaptive host defenses will be covered in Chapter 17- specific host defenses Physical barriers- The skin and mucous membranes protect your body and internal organs from injury and infectious agents. Chemical Barriers Sweat glands High salt content of sweat Sweat and sebum produced by sebaceous gland produce secretions with a low pH Acid pH of the stomach Lysozyme in tears, saliva and mucus Transferrin- a protein in the blood plasma, binds free iron that is present in the blood. Bacteria require iron as a cofactor for some enzymes. The binding of iron by transferrin inhibits the growth of bacteria in the bloodstream. Defensins in mucus are a group of molecules that can kill pathogens by forming pores in their membranes or inhibit growth by other mechanisms Defensins are small proteins found in both vertebrates and invertebrates. They are active against bacteria, fungi and enveloped viruses. Cells of the immune system contain these peptides to assist in killing phagocytosed bacteria, for example in neutral granulocytes and almost all epithelial cells. Most defensins function by penetrating the cell membrane by way of electrical attraction, and once embedded, forming a pore in the membrane which allows efflux. Cellular DefensesDefensive Cells- Blood consists of about 60 percent liquid called plasma and 40 percent formed elements (cells and cell fragments- (i.e., platelets). Boxed in area includes cell types involved in innate host defense mechanisms Lymphoid system mostly associated with specific defense mechanisms-in the next chapter Blood consists of about 60% liquid called plasma and 40 percent formed elements (cells and cell fragments) Fig. 16.1 Formed (cellular) elements of the blood Phagocytes- Phagocytes engulf foreign materials. Neutrophils- represent 50-70 percent of total leukocyts (also known as polymorphonuclear leukocytes or PMNL's) are released from the bone marrow continuously to maintain a stable circulating population. They last 1 to 3 days after activation. Contain oxidative chemicals to kill internalized microbes and are phagocytic. Eosinophils- 1-5% of the total leukocytes. Release defensive chemicals to damage parasites (worms): phagocytic. They contain granules which in turn contain chemical mediators of inflammation (e.g., histamine, major basic protein, lipases, Rnase, Dnases, peroxidase) which are toxic to both parasites and host tissues. Eosinophils are thought to be a major player in asthma. Basophils – 0.1% of total leukocytes. Release histamine and other chemicals (heparin, proteolytic enzymes, lipid mediators, e.g., leukotrienes and several cytokines, during – inflammation: responsible for allergic symptoms. Histamine and proteoglycans are pre-stored in the cell’s granules and are important source of the cytokine, interleukin-4, considered one of the critical cytokines in the development of allergies and the production of IgE (will discuss IgE in detail in the next chapter). Monocytes (macrophages)- 2-10% of white blood cells -migrate from the bone marrow into the blood. When these cells move from blood into tissues, they go through a series of cellular changes, maturing into macrophages. Macrophages are “big eater: that destroy not only microorganisms but also larger particles, such as debris left from neutrophils that have died after ingesting bacteria. Although macrophages take longer than neutrophils to reach an infection site, they arise in larger numbers than neutrophils. Macrophages are either fixed or wandering. Fixed macrophages remain stationary in tissues , e.g., lung, liver, bone, spleen and connective tissue and are given different names, depending on the tissue in which they reside. Wandering macrophages circulate in the blood. The process of phagocytosis. The phagocyte must i) find, ii) adhere to, iii) ingest and iv) digest the microorganism. Chemotaxis phagocytes first must find the invading microorganisms. Both the infectious agent and the damaged tissues release specific chemical substances to which phagocytes are attracted. In addition, basophils and mast cells release histamine, and phagocytes already at the infection site release chemicals called cytokines which among other things attract additional phagocytic cells. What you need to know about the chemotactic process is that the specific chemical agent (damaged tissue “stuff” for example) activate the polymerization of cytoskeletal actin fibers to move the macrophage (or PMN) in a concentrationdependent manner to the site of attack or injury. Neutrophil chemotaxis http://www.youtube.com/watch?v=EpC6G_DGqkI Adherence and ingestion-The ability of the phagocyte cell membrane to bind to specific molecules on the surface of the microbe is called adherence. A very important virulence factor is the capsule or surface anti-phagocytic proteins (M protein of S. pyogenes). In a previous chapter we described adherens which are important proteins in the adherence process. Digestion (following slide). Monocytes are part of the family of white blood cells called granulocytes se 50% Fa l 50% Tr ue A. True B. False Biogen Reports Its Alzheimer’s Drug Sharply Slowed Cognitive Decline An experimental drug for Alzheimer’s disease sharply slowed the decline in mental function in a small clinical trial, researchers reported Friday, reviving hopes for an approach to therapy that until now has experienced repeated failures. The drug, called aducanumab, met and in some cases greatly exceeded Wall Street expectations in terms of how much the highest dose slowed cognitive decline. However, there was a high incidence of a particular side effect that might make it difficult to use the highest dose. Aducanumab, which until now has been called BIIB037, is designed to get rid of amyloid plaque in the brain, which is widely believed to be a cause of the dementia in Alzheimer’s disease. However, other drugs designed to prevent or eliminate plaque have failed in large clinical trials, raising questions about what role the plaque really plays. Johnson & Johnson and Pfizer abandoned a drug they were jointly developing after it showed virtually no effect in large trials. Eli Lilly and Roche are continuing to test their respective drugs despite initial failures. Experts say there is some suggestion the drugs might work if used early enough, when the disease is still mild Results announced from Phase 1 single ascending dose study of PRX002, a monoclonal antibody for the potential treatment of Parkinson's disease Prothena Corporation plc, a latestage clinical biotechnology company focused on the discovery, development and commercialization of novel protein immunotherapy programs, has announced positive results from a Phase 1 single ascending dose study of PRX002, a monoclonal antibody for the potential treatment of Parkinson's disease and other related synucleinopathies. PRX002 is the focus of a worldwide collaboration between Prothena and Roche. PRX002 was safe and well-tolerated, meeting the primary objective of the study. Further, results from this study showed that administration of PRX002 leads to mean reduction of free serum alpha-synuclein levels of up to 96%. These overall results were highly statistically significant (p<0.00001). Reduction of free serum alpha-synuclein, a protein potentially involved in the onset and progression of Parkinson's disease and the target of PRX002, was shown to be robust, rapid and dosedependent after just a single dose. There is genetic and pathological evidence that supports a causal role of alpha-synuclein in Parkinson's disease," said Todd Sherer, PhD, CEO of the Michael J. Fox Foundation for Parkinson's Research. "The Phase 1 double-blind, placebocontrolled, single ascending dose study enrolled 40 healthy volunteers. All volunteers enrolled were randomized 3:1 into five escalating dose cohorts (0.3 mg/kg, 1 mg/kg, 3 mg/kg, 10 mg/kg or 30 mg/kg) to receive either PRX002 or placebo. No hypersensitivity reactions or drug-related serious adverse events were reported. PRX002 demonstrated favorable pharmacokinetic properties, supporting the current dosing frequency in the on-going Phase 1 multiple ascending dose study in patients with Parkinson's disease. There were no treatment emergent adverse events (TEAEs) in greater than 10% of subjects. The only TEAEs in greater than 5% of subjects were vessel puncture site pain, headache and viral infection. All PRX002related adverse events were mild and no dose limiting toxicities were observed. Fig. 16.3 Phagocytosis of two bacterial cells by a neutrophil Digestion: Phagocytic cells have several mechanisms for digesting and destroying ingested microbes. 1. Lysosomes found in the phagocytes cytoplasm. These organelles, which contain digestive enzymes and small proteins called defensins (Defensins promote fusion and lysis of negatively charged membranes), fuse with the phagosome forming phagolysosomes. 2. Macrophages can also use other metabolic products to kill ingested microbes. These phagocytic cells use oxygen to form hydrogen peroxide (H2O2), nitric oxide free-radical (ONOO-), superoxide ions (O2-) and hypocholorite ions (ClO-)(ingredient of household bleach). The products, indicated above, produced by macrophages to kill ingested microbes are likely important players in most inflammatory responses which can be harmful to the host. Some microbes have developed mechanisms to prevent their destruction within a phagolysosome. 1. Some bacteria (S. pneumoniae, Y. pestis) produce capsules which either prevent them from being engulfed or from being destroyed if engulfed. 2. Some bacteria- leprosy or tuberculosis organisms can resist digestion by phagocytes. 3. Some bacteria- produce toxins that kill phagocytes by causing the release of the phagocytes own lysosomal enzymes into its cytoplasm, e.g., leukocidin (both staph and strept), and streptolysin released by streptococci. As indicated in the recent article about MRSA- leukocidin is an important player in pneumonial death: Severity (of MRSA) is often due to leukocidan termed Panton-Valentine leukocidin. Extracellular killing- The leukocytes responsible for killing intracellular viruses are natural killer (NK) cells. Natural killer cells (or NK cells) are a type of cytotoxic lymphocyte that constitute a major component of the innate immune system. NK cells play a major role in the rejection of tumors and cells infected by viruses. They kill cells by releasing small cytoplasmic granules of proteins called perforin and granzyme that cause the target cell to die by apoptosis (programmed cell death). The Lymphatic System The lymphatic system which is closely associated with cardiovascular system, consists of a network of vessels, nodes and other lymphatic tissues, and the fluid lymph. It has three major functions: 1) collect excess fluid from the spaces between body cells, 2) transport digested fats to the cardiovascular system and 3) provide many of the nonspecific and specific defense mechanisms against infection and disease. Inflammation- is a body’s defense response to tissue damage from microbial infection. It is also a response to mechanical injury (cuts and abrasions), burns, sunburn, chemicals (e.g., phenol), and allergies. Cardinal signs or symptoms of inflammation: 1) increase in temperature 2) redness 3) swelling and 4) pain in the infected or injured site. Fig. 16.6 Steps in the process of inflammation and subsequent healing Molecular defenses- involve the actions of interferon and complement Chronic inflammation- When an inflammation is not destroyed, host defenses attempt to limit or confine the agent so that it cannot spread to surrounding tissue. For example, granulomatous inflammation results in granulomas. A granuloma is a pocket of tissue that surrounds and wall off the inflammatory agent (gummas of syphilis, lepromas of Hansens bacillus, and tubercles of tuberculosis) Fever- a rise in temperature in infected or injured tissue is one sign of a local inflammatory reaction. Fever, a systemic increase in body temperature, often accompanies inflammation. Body temperature is maintained by the hypothalamus and is most often increased by pyrogens. Fever can 1) increase body temperature above the optimum of the infecting agent or its toxins, 2) increase the level of immune responses by increasing the rate of chemical reactions in the body. IFNs belong to the large class of glycoproteins known as cytokines. Interferons are named after their ability to "interfere" with viral replication within host cells. IFNs have other functions: they activate immune cells, such as natural killer cells and macrophages; they increase recognition of infection or tumor cells by up-regulating antigen presentation to T lymphocytes; and they increase the ability of uninfected host cells to resist new infection by virus. Certain host symptoms, such as aching muscles and fever, are related to the production of IFNs during infection. Both beta-interferon and gamma interferon can also function to modulate the immune system by stimulating the production of cytokines (proteins involved in host defense among other functions). Interferon alpha and beta activate antiviral proteins in neighboring cells- they do not enter the cell they are going to protect- instead they bind to a surface receptor and trigger a G-protein activated cascade which in turn activates antiviral proteins. Fig. 16.7 The mechanism by which interferons a and b act. The binding of IFN to its receptor results in the transcription of a group of genes that code for antiviral proteins involved in preventing viral replication in that cell. As a consequence the cell will be protected from infection with a virus until the antiviral proteins are degraded, a process which takes several days. The antiviral state in IFN-treated cells results from the synthesis of two enzymes that result in the inhibition of protein synthesis. One protein indirectly affects protein synthesis by breaking down viral mRNA the other directly affects protein synthesis by inhibiting elongation Complement- refers to a set or more than 20 large regulatory proteins that play a key role in host defense. They are produced by the liver and circulate in plasma in an inactive form. These proteins account for about 10 percent of all plasma proteins. General function: 1) enhance phagocytosis by phagocytes, 2) lyse microorganisms, bacteria and enveloped viruses directly and 3) generate peptide fragments that regulate inflammation and immune responses. inflammation and phagocyte chemotaxis. Opsonization- the complement system can counteract the capsule/M-protein type defenses of the organism by binding to opsonins (antibodies) which are in turn used to uptake bacteria into phagocytic cells. This process is called opsonization or immune adherence Membrane attack complexes Fig. 16.8 The complement system Holes in a red blood cell caused by the complement attack complex Membrane attack complexes Side view of a membrane attack complex Fig. 16.9 Complement lesions in cell membrane physical barriers phagocytosis extracellular killing-NK cells Inflammatory response fever interferons complement Fig. 16.10 A summary Of the body’s nonSpecific defenses