Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Protein domain wikipedia , lookup
List of types of proteins wikipedia , lookup
Rosetta@home wikipedia , lookup
Homology modeling wikipedia , lookup
Protein design wikipedia , lookup
Protein folding wikipedia , lookup
Protein structure prediction wikipedia , lookup
Bimolecular fluorescence complementation wikipedia , lookup
Western blot wikipedia , lookup
Protein purification wikipedia , lookup
Nuclear magnetic resonance spectroscopy of proteins wikipedia , lookup
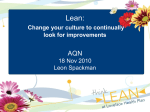
Metabolic Abnormalities in the Burn Patient Part 1 Objectives • To understand normal body composition and importance of lean body mass •To understand the metabolic changes which occur in the burn patient with activation of the “stress response” •To recognize the morbidity associated with the “stress response” and loss of lean mass Table of Contents I. Introduction II. Normal Body Composition III. Body Compositional Changes IV. Normal Metabolism V. Metabolic Response to Starvation VI. The “stress response” to burn injury VII. Controlling the stress response VIII. References I. INTRODUCTION A severe catabolic state is initiated by the major burn Smaller burns also initiate the “stress response” I. INTRODUCTION Major changes in body metabolism occur as the result of the stress of a burn injury. Every burn patient develops metabolic changes, the degree depending on the degree of the burn insult. This response leads to potentially deleterious changes in body composition, namely loss of body protein as well as a hypermetabolic catabolic state. To understand these alterations it is first necessary to define normal body composition and normal metabolic activity. A comparison can then be made with the response to starvation and “the stress response to a burn. Understanding that the marked changes in metabolism with “stress” are due to an altered hormonal environment and the response to inflammation, will provide the information needed for clinical judgment. Treatment modalities will be much more logical and be based on concept recognition rather than simply reacting to problems as they develop. II. NORMAL BODY COMPOSITION The body can be divided into two compartments. Lean body mass (LBM) makes up about 75% of body weight and contains three quarters water and all the protein and mineral in the body. The fat mass makes up about 25% of body weight and contains all the fat (water free). Fig 1 Legend: The contents of the lean body mass and fat mass compartments are shown Lean Body Mass The lean body mass contains all of the protein in the body. The LBM is highly metabolically active and essential for survival. Protein makes up all the muscle (50-60% of the LBM). The critical cell structure in all organs and connective tissue, in addition to enzymes, growth factors and antibodies (Figure 1). Any significant loss of protein is deleterious. The LBM is maintained by an intense genetic drive for preservation and action of the anabolic hormones, growth hormone, testosterone and insulin. Resistance exercise also maintains the anabolic activity (protein synthesis) needed to maintain LBM. Adequate protein intake is of course required for sufficient substrate needed by the protein synthesis pathway. Lean Body Mass Compartment •Contains all the protein in the body •High metabolic activity •Essential for survival •Any significant protein loss is deleterious •Normal adaptation is to preserve and not use for fuel What Maintains Lean Mass? •Intense genetic drive to maintain body proteins •Anabolic hormones which stimulate protein synthesis •Adequate protein intake to meet demands •Resistance exercise Muscle is a very dynamic tissue, with about 50-100 grams of muscle continually broken down and re-synthesized each day. In healthy man, the rate of loss and synthesis is equal, with a net zero nitrogen (N) balance. With increased anabolism, (increased protein synthesis) muscle gain, is increased with a nitrogen gain. With burn injury, there is a net loss. Muscle is 75% water or (1 gram of muscle N=25-30 grams muscle). Multiplying protein by 4 is a good estimate of muscle (gms). N (grams) x 6.25 = protein (gms) x 4 = muscle (gms). Intake of adequate calories, protein, vitamins and trace elements, are required to maintain normal body composition. Fat Mass Fat mass contains mostly fat stored as an energy reserve. Some fats essential for survival are also present. The fat mass typically has over 100,000 potential calories assuming the metabolic environment is in the fat burning mode as seen with pure starvation. Fat Mass Compartment •Not metabolically active •Mainly a fuel depot •Fat loss not necessarily deleterious •Normal adaptation is to use fat for fuel instead of protein III. BODY COMPOSITIONAL CHANGES The body composition changes in the burn patient are involuntary. There is a major difference between involuntary weight loss and voluntary weight loss. The former is dangerous if not well controlled as the problem of weight loss in the surgical patient is that of lean mass loss. Loss of lean mass instead of fat is sure to lead to significant complications. The complications from lost lean mass, caused by the metabolic changes of stress. Complications correlate with the percent of total lean mass lost assuming normal body composition prior to the loss. Pre-existing losses are added to the loss from a body insult in order to recognize the potential complications expected. The relationship between the loss of lean mass and the degree of morbidity and mortality is shown. A 40% loss of total lean mass is fatal. Complications Relative to Loss of Lean Body Mass Complications of Lean Mass Loss •Loss of muscle strength and the ability to function physically •Thinning of skin leading to pressure sores •Poor healing leading to chronic wounds •Decreased weight bearing leading to loss of calcium from bone Complications of Lean Mass Loss (cont’d) •Increased infections •Poor quality of life •Malnutrition •Progression of complications The effect of lost body protein on wound healing relates to the fact that there is competition of protein substrate between the wound and restoration of LBM. The impairment of cutaneous wound healing is also proportional to the amount of lost lean mass. The wound still has priority for protein substrate for healing, with a LBM loss of up to 10% of total. With progressive losses, the lean mass compartment increasingly competes with available protein substrate to restore itself. This self preservation process is aimed at avoiding further morbidity with lost lean mass, which become a higher risk than the wound itself. As the skin protein decreases throughout the body, new wounds will develop as well as the reopening of old wounds. Fig. 2 Legend 2: With a loss of lean mass less than 10%, the wound takes priority over available protein substrate. As lean mass continues to decrease more consumed protein is used to restore LBM with O less being available to the wound. Wound healing rate decreases until lean mass is restored. With a loss of lean mass exceeding 20% of total, spontaneous wounds can develop due to the thinning of skin from lost collagen. Causes of Lean Mass Loss There are several routes to involuntary weight loss and lean mass loss. The first is via the acute injury, surgery, or infection induced process where increased nutrient requirements and wasting of body protein are characteristics. The presence of other stressors, such as pain and anxiety, can lead to the same endpoint. Then PEM occurs rapidly, due to the lack of any adaptive or protective responses. Often the insult or “stress” resolves, but the weight loss and PEM are never corrected in the recovery phase leading to a chronic protein deficit and its resulting complications. With the presence of any catabolic insult the degree of lean mass loss (% of total) exceeds the degree of weight loss, as lean mass is not protected and fat mass is not preferentially used for fuel. Increased nutrient losses due to gastrointestinal disease, can lead to the same endpoint. The second route is due to inadequate nutrient intake, both quality and quantity. This process is very common in the elderly, those with disability, lack of appetite from chronic illness, mental illness, and poverty. The onset of severe weight loss precedes the PEM as some adaptation will occur and lean mass is initially spared, but eventually protein-energy malnutrition will occur.9 The third route is through the disuse atrophy of post-injury bed rest, inactivity and the resulting disability. Whatever the route, the most common cause of weight loss and protein energy malnutrition is the triad of increased nutrient demands, decreased intake, and inactivity. Causes of Lean Moss Loss •The stress response to injury •Other stressors: Pain, Anxiety, Hypo/Hyperthermia •Disuse atrophy from bed rest, inactivity, disability •Nutrient deprivation with protein energy malnutrition •Combination IV. NORMAL METABOLISM Metabolism is defined as the sum total of all the chemical reactions required for all function. To better understand the metabolic changes in the surgical patient, it is best to compare normal metabolism, that due to starvation and that due to stress in the surgical patient. The terminology used in describing metabolism, is presented. Definitions Energy: The capacity to do work Energy Production: defined in terms of standard Energy units produced per time, or Oxygen Consumed per time, as oxygen is required for Energy production. Energy Consumptions: Energy used/time (e.g. Kcal/hr or ml O2 /min.) Kilocalorie – standard measure of the quantity of Energy obtained from nutrients (often referred to as a Calorie) (e.g. One gram Carbohydrate produces 3.3 Kcal) Calorie: term used interchangeably with Kcal. Energy Production: term used to quantify the amount of energy generated over time. Since 95% of the oxygen used is for energy production, oxygen consumed can also be used as a measure of energy as can the Kilocalorie (Calorie). Energy Consumed: quantifies the energy used. Energy consumed, in the form of oxygen used or Calories burned is used to determine the patients nutrient requirements. Metabolism: Sum (body) total of all chemical reactions required for cell function – an energy requiring process. Hypermetabolism: increase in metabolic rate above normal for a specific activity level. Anabolism: Constructive Metabolism: protein synthesis and new tissue formation. Catabolism: Destructive Metabolism: protein breakdown producing tissue degradation. Protein-Energy Malnutrition (PEM) is defined by inadequate intake of energy and protein is the most common form of malnutrition in the acutely injured, chronically ill or incapacitated respiratory dysfunction populations. The initial symptoms of fatigue (cell energy crisis) is followed by progressive weight loss including fat but predominantly lean mass. Unintentional Weight Loss6-10 Loss of 10% of actual body weight over a 6 month period or greater than 5% over 30 days is usually considered to be the definition for weight loss producing a significant health risk. Because unintentional weight loss is often an associated factor in malnutrition, as well as injured or ill patients, and is easy to monitor. The degree of weight loss is used as a marker of the degree of malnutrition. Weight loss itself is used as a medical quality assurance marker for adequacy of nutrition in patient populations at risk. The degree of morbidity including poor wound healing and development of ongoing respiratory disease increases as the degree of weight loss increases. B. Hormonal Regulation Hormones regulate the metabolic pathways. These chemical messengers control nutrient processing and control the rate of anabolism and catabolism. • • • • • Hormones Chemical messengers from endocrine system Control nutrient processing Maintain energy balance Control rate of protein synthesis (anabolism) and protein breakdown (catabolism) Key Hormones Regulating Metabolism Insulin Controls glucose to energy Converts excess glucose to fat Converts amino acid to protein (anabolic) • Catecholamines Increases metabolic rate Anti-insulin: increases blood glucose • Cortisol Stimulates gluconeogenesis Causes protein breakdown (catabolic) • Growth Hormones Stimulate protein synthesis (anabolic) Anticatabolic Increases blood glucose • Glucagon Stimulates glucose production Catabolic • Testosterone Increases protein synthesis (anabolic) Normal metabolic activity is shown. Normal energy expenditure is about 25 cal/kg/day. Carbohydrates provide most of the fuel (60%) for energy followed by fat. (25-30%) Very little protein is used for fuel, most being used for protein synthesis. Figure 3 Legend: Normal metabolic activity is controlled by hormonal balance. The energy compartment is fueled mainly by carbohydrates and fat while the lean mass or protein compartment is maintained by ingested protein. Therefore the normal partitioning of macronutrients is carbohydrate and fat to energy and protein, to the protein synthesis. Anabolic hormones maintain this balance. Fig. 4 Legend: The hormonal environment maintains the activity in these compartments of energy production and protein synthesis. Anabolic activity maintains the protein synthesis pathway.