Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Adaptive immune system wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Sjögren syndrome wikipedia , lookup
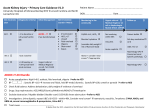
2120 Human Acute Kidney Injury (AKI) is Associated with a Pro-inflammatory Phenotype M Varrier, N Gauge, D Boardman, M Hernandez-Fuentes, M Ostermann Guy’s and St Thomas’ Hospital and King’s College London Introduction: Patients with AKI have markedly worse outcomes than otherwise matched controls. There is increasing evidence from animal models that leukocytes play a central role in the pathophysiology of AKI resulting in an inflammatory response (1, 2). We conducted a pilot study aiming to describe the immune phenotype in human AKI using flow cytometry. Methods: We enrolled three groups of patients: 1) AKI stage II/III (defined by KDIGO criteria) and systemic inflammatory response syndrome (SIRS) without sepsis; 2) SIRS without AKI; and 3) AKI stage II/III without SIRS. A healthy control population was used for baseline comparison. Serial blood samples were taken on day 0, 2 and 7. Cells were separated from whole blood using percoll gradients and stained using panels of antibodies specific for lymphocyte, monocyte or neutrophil markers. Cells were acquired by flow cytometry using BD LSR Fortessa and analysed using FlowJo (Tree Star, USA). We compared the median values on day 0 between all groups. Results: Results from 24 day 0 samples identified statistically significant differences in the proportion of cytotoxic CD8+ T Cells, CD45-CD25+++ regulatory T cells and CD45-CD25++ cytokine secreting non T regulatory cells between SIRS, AKI, AKI + SIRS and healthy controls (Table 1). The percentage of CD69 positive neutrophils was significantly increased across all 3 groups relative to controls, with little variation between AKI, SIRS and AKI+SIRS patients. Table 1- Group column values are percentages Cell type day 0 CD8+ Cytotoxic T cells Fr. II CD45-CD25+++ T cell regs Fr. III CD45-CD25+ Cytokine Secreting non T regs CD69+ Neutrophils 23.3 4.1 AKI alone 16.7 2.7 SIRS alone 11.6 1.6 11.5 21.2 83.9 69.7 AKI+SIRS Controls p value 31.1 1.2 0.039 0.002 13.9 8.0 0.008 65.5 7.35 0.023 Conclusions: Our results indicate that AKI is associated with an inflammatory phenotype similar to patients meeting SIRS criteria. The combination of AKI and SIRS is associated with increased CD8+ cytotoxic T cells. In addition cytokine secreting non-regulatory T cells (Fr. III) appear particularly elevated in patients with AKI alone. We aim to complete recruitment of 20 patients in each group, analyse day 2 and 7 results and perform cytokine profiling on saved serum samples to conclude this study. More research is needed to fully characterise the inflammatory response in human AKI and any resultant systemic effects in order to develop targeted treatment to improve clinical outcomes. References 1. 2. Kinsey GR, Okusa MD. Role of leukocytes in the pathogenesis of acute kidney injury. Crit Care. 2012;16(2):214. Kinsey GR, Okusa MD. Expanding role of T cells in acute kidney injury. Curr Opin Nephrol Hypertens. 2014;23(1):9-16.