Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
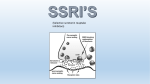
Depression in Primary Care Chirag V Desai MD Chirag V Desai MD, LLC 8823 San Jose Blvd, Suite 303 Jacksonville, FL 32217 Learning Objectives: • Upon completion of this activity, participants should be able to: 1. Define and describe the different forms of depressive disorders. 2. Choose proper assessment methods and identify current FDA approved medication interventions to treat depressive disorders Depression in Primary Care • Depression is the most common psychiatric disorder in the general population • Most common mental health condition in patients seen in primary care • Two-thirds of primary care patients with depression present with somatic symptoms (ie, headache, back problems, or chronic pain), making detection of depression more difficult DSM-V Criteria • A major depressive syndrome or episode manifests with five or more of the following symptoms, present most of the day nearly every day for a minimum of two consecutive weeks. At least one symptom is either depressed mood or loss of interest or pleasure. • Depressed mood • Loss of interest or pleasure in most or all activities • Insomnia or hypersomnia • Change in appetite or weight • Psychomotor retardation or agitation • Low energy • Poor concentration • Thoughts of worthlessness or guilt • Recurrent thoughts about death or suicide, or a suicide attempt Biological Basis of Depression: Monoamine Hypothesis Norepinephrine Serotonin Dopamine Brain-Derived Neurotrophic Factor (BDNF) Neurogenesis, synaptogenesis, neuronal resilience Under stress, the BDNF gene is repressed Sustains viability of neurons Epidemiology: Depression Prevalence 14% lifetime prevalence (unipolar depression)1 Impact 2nd leading cause of disability in the US2, suicide, impairment Gender ratio 2x female Risk Factors Family hx Depression (G x E) Substance use Comorbidity Anxiety, ADHD, Substance Use Disorders Future Recurrent depression 30-70% relapse in 1-2yrs 1 – Kessler et al, 2011; 2 – US Burden of Disease Collaborators, 2013. Flavors of 1 Depression • Polarity: Unipolar vs. bipolar • Symptom-based specifiers: Melancholic (25-30%) severe Atypical (<40%) Main Symptom lack of mood reactivity OR anhedonia + Mood reactivity Additional features 3: ↓app/wt, ↓ Sleep, worse AM mood, despair 2: ↑ app/wt, ↑ Sleep, Leaden paralysis, IP rejection sensitivity Other Treatment-resistance Women, SA, young; Use of MAOIs 1 – Thase ME, 2013. “Flavors” Continued Anxious (up to 40%) Psychotic (15-20% of severe) Symptoms 2: restlessness, tension, poor C (worry), fears: losing control, something bad will happen Delusions, hallucinations Features Poorer outcomes with pharmacotherapy high recurrence, hospitalizations, longer episodes, impairment Treatment Adjunctive pharmacotherapy, CBT Treatment w/ antipsychotics, ECT Onset-based subgroups • Seasonal affective Disorder • Associated w/ inc. latitude, women • Different treatment: buproprion1, bright light therapy • Peripartum onset • • • • Non psychotic depression : 13% of women who deliver Recurrence rates up to 50% in subsequent preganancies2 Includes pregnancy and post-partum period Treatment: Antidepressants (FDA Class C), CBT 1 – Westrin A, Lam RW. 2007; 2- O’Hara 1996. Screening Instruments: • PHQ-9: scored 0 to 27, with scores ≥10 indicating a possible depressive disorder. It has a sensitivity of 88 percent and specificity of 88 percent. • PHQ-2: Comprised of the 1st two questions of PHQ-9: • During the last month, have you often been bothered by feeling down, depressed, or hopeless? • During the last month, have you often been bothered by having little interest or pleasure in doing things? Screening Instruments: • Beck Depression Inventory for Primary Care: • 7 item modified inventory adapted from the 21 item full BDI-II • 4 point cutoff for identifying MDD • 97 percent sensitivity and 99 percent specificity for identifying major depression • Unfortunately, only available by license requiring a fee which limits broader use Medical Factors to Consider: Other conditions can exhibit similar behaviors as major depression such as: Hypothyroidism Cushing disease Substance Abuse Medication : OCP, Steroids, Interferon, Beta blockers (Propanolol). SSRI’s and Effect on CYP450 • SSRIs inhibit P450 (CYP1A2, CYP3A4, CYP 2D6) • Can increase levels of anti-arrhythmics, β-blockers, antihistamines, and Ca2+ channel blockers • e.g. CYP2D6 inhibition by fluoxetine, paroxetine, sertraline (weak) may cause metoprolol and carvedilol accumulation and bradycardia • e.g. CYP2C19 inhibition by fluoxetine inhibits clopidogrel’s effect by inhibiting conversion to active metabolite • Escitalopram and citalopram (1A2,2D6,2C19) weak inhibitors Tricyclic Antidepressants • Relatively safe in short term use for stable ischemic heart disease, prior MI or CHF • Orthostatic hypotension is very common • Nortriptyline is thought to be safest in CHF due to minimal effect on orthostasis and ejection fraction • All TCA’s have quinidine like anti-arrhythmic properties that delay cardiac conduction, increase HR and prolong QTc Descriptors of Medication Effect: Response – 50% reduction in symptoms Remission – all symptoms removed Recovery – 6 to 12 months of remission Relapse – worsens before remission Recurrence – worsens months after recovery Mechanism of Action • Currently still do not have a complete and adequate explanation of how antidepressants work • Some block monoamine reuptake • Others block alpha-2 receptors • Still others block monoamine oxidase • Direct vs indirect effects on neurotransmitters Antidepressant Types: Selective Serotonin Reuptake Inhibitor (SSRI) Monoamine Oxidase Inhibitor (MAOI) Tricyclic Antidepressant (TCA) Serotonin/Norepinephrine Uptake Inhibitor (SNRI) Norepinephrine/Dopamine Uptake Inhibitor (NDRI) Noradrenergic/Specific Serotonergic AD (NaSSA) Serotonin Antagonist Reuptake Inhibitor (SARI) Receptor Subtypes: 5HT1A – Anxiolytic & Antidepressant 5HT2A – Anxiety, Insomnia, OCD, Libido 5HT2C – Anxiety & Weight loss 5HT3 – GI problems & Nausea 5HT1D – blockade of 5HT release Selective Serotonin Reuptake Inhibitors fluoxetine (Prozac) paroxetine (Paxil) sertraline (Zoloft) citalopram (Celexa) escitalopram (Lexapro) Chemical Structure First-line treatments for: Major depressive disorder (MDD) Panic disorder (PD) Obsessive-compulsive disorder (OCD) Social anxiety Posttraumatic stress disorder (PTSD) Bulimia Generalized anxiety disorder (GAD) Premenstrual dysphoric disorder (PMDD) FDA Indications: MDD (approved for all except fluvoxamine) PD (approved for fluoxetine, paroxetine, and sertraline) OCD (approved for all except citalopram and escitalopram) Social Anxiety (approved for sertraline and paroxetine) FDA Indications Cont’d PTSD (approved for sertraline and paroxetine) Bulimia (approved for fluoxetine) GAD (approved for paroxetine and escitalopram) PMDD (approved for fluoxetine [Sarafem only], paroxetine [controlled release only], and sertraline) Adverse Effects: Most common side effects Nausea, diarrhea, headache Decreased libido Delayed/Inability for orgasm “Serotonin Syndrome” Hyperpyrexia, myoclonus, mental status changes, seizures, arrhythmias, delirium Drug Interactions: Increase TCA levels (paroxetine, fluoxetine) Increase carbamazepine, phenytoin (paroxetine) Increase haloperidol, olanzapine, risperidone (paroxetine) MAOI (contraindicated): serotonin syndrome Smoking decreases many psychotropic levels Serotonin/Norepinephrine Reuptake Inhibitors venlafaxine (Effexor) duloxetine (Cymbalta) desvenlafaxine (Pristiq) Chemical Structure Venlafaxine (Effexor) Blocks reuptake of serotonin, norepinephine, (and to a lesser extent, dopamine) First-line monotherapy for MDD Activating at high doses Can elevate blood pressure at higher doses Some efficacy for PTSD that failed SSRI Treatment of chronic pain conditions Duloxetine (Cymbalta) Blocks serotonin and norepinephine More potent norepinephrine reuptake inhibitor (NRI) compared to venlafaxine First-line monotherapy for MDD Approved for Peripheral Neuropathy May treat stress urinary incontinence Desmethylvenlafaxine (Pristiq) Major metabolite of venlafaxine More potent reuptake inhibitor of norepinephrine Only approved for MDD Appears to be effective to treat vasomotor symptoms from menopause 50mg initiation/final dose Not metabolized by P-450 and thought to have less drug-drug interaction Indications: MDD (Effexor XR, duloxetine, desvenlafaxine) GAD (approved for Effexor XR and duloxetine) Social anxiety disorder (approved for Effexor XR) Neuropathic pain (approved for duloxetine) Fibromyalgia (approved for duloxetine) Safety Fatal overdoses with venlafaxine are exceedingly rare No reported fatal overdoses of duloxetine 10 g or more resulted in seizures and serotonin syndrome Desvenlafaxine overdoses associated with arrhythmias, serotonin syndrome, rhabdomyolysis (often in combination with other drugs) NORADRENERGIC-DOPAMINERGIC ANTIDEPRESSANT • Bupropion (Wellbutrin) Chemical Structure Indications: First-line monotherapy or augmentation for mild to moderate depression Smoking cessation (Zyban) Treatment of seasonal affective disorder Appears to be effective in the treatment of ADHD Not effective in the treatment of anxiety disorders Factors to Consider: Relatively safe in overdose Completed suicides due to underlying seizure disorder Counteract sexual dysfunction EtOH abuse/Eating Disorders Lower doses for liver and kidney problems Factors to Consider: Serious drug interactions are uncommon Drugs that lowers the seizure threshold such as clozapine and clomipramine should be used cautiously or avoided MAOI and bupropion is contraindicated as greater risk of hypertensive crisis Avoid if dependent on alcohol or benzodiazepines Tricyclic Antidepressants: imipramine (Tofranil) amitriptyline (Elavil) clomipramine (Anafranil) desipramine (Norpramin) nortripyline (Pamelor) Chemical Structure Indications: Second- or third-line agents for MDD Panic disorder OCD (FDA approved for clomipramine) Pain syndromes Migraine prophylaxis Enuresis (FDA approved for imipramine) Mechanism of Action: Block Serotonin reuptake Block Norepinephrine reuptake Block alpha1 adrenergic receptors Block H1 histamine receptors Block muscarinic cholinergic receptors Adverse Effects: Dry mouth, urinary retention, constipation, confusion, blurred vision, tachycardia Weight gain Sedation Sexual dysfunction Orthostasis Cardiac conduction abnormalities by blocking sodium channels (cardiac arrest and seizures) Factors to Consider: Amitriptyline has a very poor side-effect profile secondary to its anticholinergic and antihistaminic side effects Desipramine and nortriptyline have the most favorable side-effect profiles Desipramine more stimulating Amitriptyline more sedating Drug Interactions: Anticoagulants: ↑ warfarin levels Antipsychotics: ↑ TCA and antipsychotic levels Cimetidine: ↑ TCA levels Stimulants: ↑ TCA levels Oral contraceptives: ↑ TCA levels SSRIs: ↑ TCA levels Monoamine Oxidase Inhibitors: Nonselective MAO Inhibitors phenelzine (Nardil) tranylcypromine (Parnate) isocarboxazid (Marplan) Selective Inhibitor MAO B for treatment of Parkinson’s Disease Selegiline (Eldepryl) transdermal (Emsam) Chemical Structure Indications: Third-line agents for MDD (FDA approved for resistant depression) Social anxiety Panic disorder Parkinson's disease (selegiline has FDA approval) Mechanism of Action: Irreversible inhibitor of monoamine oxidase A (MAO-A) Exert effects on norepinephrine and 5-HT Selective irreversible MAO-B inhibitor Exert effects on phenylethylamine and dopamine Adverse Effects: Weight gain Orthostasis Sexual dysfunction Dry mouth Insomnia/somnolence Headache Factors to Consider: Potentially lethal in overdose Hypertensive crisis Stroke Myocardial infarction Requires 2-3 week wash-out period before switching to another antidepressant Dietary Considerations: Foods to be avoided (tyramine content): Beer, red wine Aged cheeses (cottage and cream cheese allowed) Dry sausage Fava or Italian green beans Brewer's yeast Smoked fish Liver (beef or chicken) Drug Interactions: ß-Blockers: hypotension, bradycardia Bupropion (contraindicated): hypertensive crisis, seizure Carbamazepine (contraindicated): hypertensive crisis Meperidine (contraindicated): serotonin syndrome Nefazodone: possible serotonin syndrome Sympathomimetics: hypertensive crisis SSRIs (contraindicated): serotonin syndrome TCAs: clomipramine contraindicated Mirtazapine (contraindicated): hypertensive crisis SNRIs (contraindicated): serotonin syndrome Vilazodone HCl (Viibryd) • • • • • • • • SSRI with dual mechanism of action Blocks serotonin reuptake through the serotonin transporter Partial agonism of the 5-HT1A presynaptic receptor FDA indicated for MDD Thought to decrease the therapeutic lag of traditional SSRI’s Felt to have less sexual side effects compared to the other SSRI’s Common adverse effects include diarrhea, nausea, vomiting and headache should be taken with food because it has 72% bioavailability after a meal Levomilnacipran (Fetzima) • Serotonin–norepinephrine reuptake inhibitor (SNRI) • Levomilnacipran is the enantiomer of milnacipran, approved in Europe for depression but only for fibromyalgia pain and peripheral neuropathy in the US • In theory, levomilnacipran should improve cognitive functions linked to norepinephrine: concentration and motivation, and in turn, improve social function • Potential adverse effects include: increases in heart rate and blood pressure, and dose-dependent urinary hesitancy and erectile dysfunction • levomilnacipran is affected by renal function but no dose adjustment needed in mild renal impairment Vortioxetine (Trintillex) • SSRI as well as a 5-HT1A full agonist and 5-HT3 receptor antagonist • Inhibitory effect on 5-HT7 and 5-HT1D receptors and partial agonism of 5-HT1B receptors • Ultimate effect of the multimodal action is an increase in dopamine, norepinephrine, and acetylcholine activity in the prefrontal cortex • In theory, this should lead to improvement in cognitive deficits associated with depression • Specifically studied for use in the geriatric population References American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington, VA: American Psychiatric Association; 2013. American Psychiatric Publishing Textbook of Psychopharmacology, 4th edition. Schatzberg AF, Nemeroff CB (eds); American Psychiatric Publishing, Inc. Washington, D.C. (2009). Deardorff WJ, Grossberg GT. A review of the clinical efficacy, safety and tolerability of the antidepressants vilazodone, levomilnacipran and vortioxetine. Expert Opin Pharmacother. 2014;15(17):2525-2542 Kessler RC, Ormel J, et al. Development of lifetime comorbidity in the World Health Organization world mental health surveys. Arch Gen Psychiatry 2011;68:90. O’Hara MW. Swain AM. Rates and risk of postpartum depression: a meta-analysis. Int Rev Psychiatry. 1996;8: 37-54 Prescriber’s guide to using 3 new antidepressants: Vilazodone, levomilnacipran, vortioxetine Current Psychiatry. 2015 February;14(2):28-29, 32-26 Thase ME. The multifactorial presentation of depression in acute care. J Clin Psychiatry 2013; 74 (suppl 2): 3 – 8. US Burden of Disease Collaborators. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors. JAMA 2013; 310:591. Up To Date: Screening for Depression Westrim A, Lam RW. Long-term and preventative treatment for seasonal affective disorder. CNS Drugs. 2007; 21:901-999.