Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Toxicodynamics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacology 301.6
Module 6
Lesson 2
Lipids/Obesity
Lipid cycling
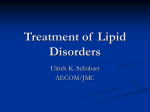
Goodman and Gilman’s Pharmacological Basis of Therapeutics, 10th ed. 2001
Chylomicron
metabolism
HL = hepatic
lipase
LPL =
lipoprotein
lipase
FFA = free
fatty acids
ApoE mediated
Lipoprotein classes
protein
choles.
triglycerides
• Chylomicrons
B48
85%
•VLDL
B100/E
20%
55%
• IDL
B100/E
35%
25%
• LDL
B100
60%
5%
•HDL
AI/II/E
20%
5%
LDL is not measured but calculated:
LDL-C = total cholesterol - (HDL-C + TG/5)
(Triglycerides must be <4.5 mmol/L or < 400 mg/dL)
Hyperlipidemia
• Major CV risk factor - 25% of population
• LDL, Total Choles., Total Choles./HDL, and
1/HDL all predict CVD
• Reducing LDL with diet (10%) or drugs (2060%), prevents CVD, saves lives and money
• Generally safe, expensive (use in high risk
pts.)
• Statins, fibrates, niacin, bile acid binding
resins
Statins
Most effective and best-tolerated agents for
treating dyslipidemia
Effective except when LDL receptor
dysfunctional
Inhibit 3-hydroxy-3-methylglutaryl
coenzyme A (HMG-CoA) reductase –
catalyzes cholesterol biosynthesis
Reduce cholesterol and VLDL synthesis in
the liver
Lovastatin MEVACOR
Statins How do they work?
LDL receptors in liver, plasma LDLC clearance ( by 20-55%)
Higher doses of atorvastatin and
simvastatin triglyceride levels (LDL
receptor - Apo-E in VLDL)
Some statins may HDL-C levels
Statins –
other potential cardioprotective effects:
On endothelial cell function – increase
NO synthesis
On plaque stability – reduce degradation
of matrix by metalloproteinases
On inflammation – antiinflammatory?
On lipoprotein oxidation – reduce
oxidation of LDL and uptake by
macrophages
On blood coagulation – reduce platelet
aggregation and alter fibrinogen levels
Statins - kinetics
Extensive first pass metabolism for all
Atorvastatin longer half-life (30 h) than
other statins (1-4 h) – more efficacious?
Given at bedtime – cholesterol synthesis –
midnight to 2 a.m., not with bile-acid seq.
Do not use during pregnancy or while
breast feeding as its safety in these
situations has not been established.
Statins
Better in combination with bile-acid binding
resins (cholestyramine & colestipol), niacin
or fibrates
Side effects are rare:
hepatotoxicity (ALT determinations)
myopathy (can progress to myoglobinuria
and renal failure), esp. when other drugs
metablized by CYP3A4 are given together –
erythromycin, azole antifungals,
cyclosporine, antidepressants, nefazodone,
protease inhibitors
Cerivastatin was withdrawn from the US
market in 2001
Gemfibrozil LOPID Fibrates Bezafibrate BENZALIP SR
Drugs of choice for hypertriglyceridemia
(>1000 mg/dl) to prevent pancreatitis
Gene transcription through - peroxisomal
proliferation activated receptor (PPAR-α)
Liver and adipose tissue, less in kidney, heart
and skeletal muscle
Stimulates fatty acid oxidation
LPL activity, plasma triglycerides & VLDL
hepatic apoC-III –
VLDL clearance
apoA-I and apoA-II – HDL-C
Clofibrate ATROMID-S
Fenofibrate LIPIDIL MICRO
Fibrates
Better absorbed with meals
Side effects are uncommon - GI distress
Drug-Drug Interactions:
Fibrates plus statins myopathy
Fibrates – renal failure and hepatic
dysfunction - relative contraindications
Not used in children, during pregnancy
and breast-feeding
Nicotinic Acid (Niacin)
Water soluble B-complex vitamin
Multiple actions
Reduces plasma LDL by 20 to 30% (4.5-6
g/d)
Best agent to increase HDL-C (30-40%)
Reduces triglycerides by 35-45% (2-6
g/d)
Side effects limit use
Niacin – How does it work?
1. Inhibits lipolysis of triglycerides in adipose
tissue
2. In liver -
triglyceride synthesis & hepatic
VLDL production
3. Lowers LDL (comes from VLDL)
4.
LPL activity,
clearance of chylomicrons
and VLDL triglycerides
5.
HDL-C levels, clearance in the liver
Niacin tabs – 50 to 500 mg OTC
Niacin – Adverse reactions
Common and reduce patient compliance:
Flushing (with drop in blood pressure syncope in some patients) (give aspirin)
Dyspepsia (take after meals)
Pruritis, skin rashes.
Hepatotoxicity (the most serious side
effect)
Avoid in peptic ulcer patients & gout
Worsens diabetes
Avoid in pregnancy – birth defects
Niacin + statins – watch out for myopathy
Cholestyramine NOVO CHOLAMINE
Bile-acid sequestrants (Resins)
Oldest lipid-lowering drug – second line
drugs to add to statins.
Positively-charged anion-exchange
resins
binding negatively charged bile acids
(95% of which are normally reabsorbed)
Liver has to synthesize new bile acid and
uses cholesterol – LDL receptors
increase
Colestipol COLESTID
Colesevelam WELCHOL
Cholestyramine QUESTRAN
Resins
• Max. doses of cholestyramine and colestipol
LDL-C by upto 25% (unacceptable GI side
effects)
• Colesevelam LDL-C by 18% at its max. dose
Advantage: Probably the safest - not
absorbed
Only hypocholesterolemic drugs currently
recommended for children 11-20 y of age
Not used in patients with
hypertriglyceridemia (increase triglyceride
synthesis)
Colestipol COLESTID
Resins
Side Effects:
Interfere with absorption of fat soluble
vitamins (ADEK), folic and ascorbic acids,
other fat-soluble drugs (e.g., griseofulvin
for tinea), thiazides, furosemide,
propranolol, l-thyroxine, coumarin
anticoagulants, cardiac glycosides, statins.
GI: bulk of resin causes discomfort –
bloating & dyspepsia (suspend in liquid
several h before ingestion)
Colesevelam better? – newer anhydrous
gel-tablet form
Obesity
Body mass index (BMI) = weight (Kg) 2
{height (m)}
BMI 20-25 normal
BMI 25-27 borderline
BMI 27-30 overweight
BMI >30
Waist
male > 100 cm (40”)
female > 90 cm (36”)
obese
Increased risk of diabetes
Prevalence in Canada
of BMI 27
60%
male
51%
48%
45%
female
40% 40%
40%
36%
32%
26%
26%
20%
16% 16%
18%
0%
18-24
25-34
35-44
age
45-54
55-64
65-74
What we have now:
Glazer G Arch. Intern Med 2001; 161: 1814-24
Overview of studies lasting 36-52 weeks
Drug
Plbo corr weight loss
(all published studies)
phentermine
sibutramine
orlistat
diethylpropion
7.9 kg
4.3 kg
3.4 kg
1.5 kg
Orlistat (XENICAL®)
Davidson MH et al JAMA 1999; 281: 235-42)
• inhibits pancreatic and intestinal lipases
• not absorbed (<1%) (no worry about systemic
adverse effects)
• reduces fat uptake of fatty acids by 30%
• adverse effects: bloating
40%
oily spotting
33%
fecal urgency
30%
• 7/657 (1%) patients withdrew from study
• lower serum vit A,D,E,K. corrected with suppl
• drug interactions: cyclosporine absorption
Sibutramine (MERIDIA®)
Anon. Med Letter 1998; 40; 32
• inhibits reuptake of NE, 5HT, and DA ( conc in brain)
• absorbed, metabolized by CYP3A4
• adverse effects: dry mouth, headache, constipation
increased HR and BP (dose related)
• drug interactions:SSRI’s, triptins, lithium, opiates
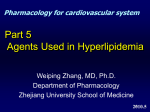
Leptin
Reproductive function
Gn-RH
LH
FSH
Leptin receptors
Hypothalamus
Body wt.
Endothelial cells
T-lymphocytes
Neuropeptide Y
Hunger
Food intake
Adipocytes
stomach
placenta
leptin
insulin
energy
intake
energy
expend
Most obese humans are leptin resistant
Summary
• Hyperlipidemia is a major cardiovascular
risk factor
• Statins have been shown to save lives and
money
• Fibrates likely do too
• Obesity is a national epidemic
• We have a few drugs that are useful for
obesity