Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
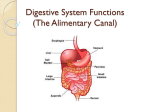
كلية الطب المحاضرةالسابعة (GIT) physiology المرحلة الثانية Enterohepatic Circulation of Bile Salts. The bile micelles still in the chyme, where they function again and again to help absorb still more monoglycerides and fatty acids .About 94 % of the bile salts are reabsorbed into the blood from the small intestine, about one half of this by diffusion through the mucosa in the early portions of the small intestine and the remainder by secondary active transport process through the intestinal mucosa in the distal ileumThey then enter the portal blood and pass back to the liver, passage through the venous sinusoids ,then back into the hepatic cells and then are resecreted into the bile. Bile salts make the entire circuit some 17 times before being carried out in the feces. The small quantities of bile salts lost into the feces are replaced by new amounts formed continually by the liver cells. This recirculation of the bile salts is called the enterohepatic circulation of bile salts. . Vitamins : A vitamin is an organic compound needed in small quantities for normal metabolism that cannot be manufactured in the cells of the body. Lack of vitamins in the diet can cause important metabolic deficits. These requirements, depending on such factors as body size, rate of growth, amount of exercise, and pregnancy. Vitamin Absorption Vitamins are absorbed mainly in the jejunum and ileum sections of the small intestine. A, D, E, and K are the fat soluble vitamins and they must be absorbed in combination with fat. The B’s and C, vitamins are water soluble vitamins. BI Thiamine, B2 Riboflavin, B6 Pyridoxine, B12 cobalamin compounds, as well as biotin, folic acid, nicotinic acid and pantothenic acid. In most cases, absorption of them occur via an Na-dependent cotransport mechanism in the small intestine, except of vitamin B 12 which requires intrinsic factor ( a glycoprotein secreted by gastric parietal cells). They start breaking down in the stomach and then throughout the small intestine. Minerals Absorption : Intestinal absorption of minerals increases or decreases depend on lacking of the particular nutrient from the body. Calcium:Are actively absorbed into the blood especially from the duodenum, controlled by parathyroid hormone which activated vitamin D. and then vitamin D greatly enhances calcium absorption . In children, inadequate Ca⁺⁺ absorption causes rickets and in adult causes osteomalacia. Iron:It is absorbed in the intestine as a free iron or as heme iron, in the cells heme is digested by lysosomal enzymes, releasing free iron. Free iron binds to apoferritin and transported across the basolateral membrane into the blood. In circulation iron is bound to transferrin β-globulin) which transports it to storage site in the liver then to bone marrow.Deficiency of iron cause anemia. Intestinal fluid and electrolyte transport GIT absorbs large quantities of fluid and electrolytes. The small and large intestine absorb 9 L of fluid daily (liquid in diet 2 litters and salivary, gastric,pancreatic, biliary and intestinal secretion 7 litters). The small remaining volume (100-200 ml) is excreted in feces. The small intestine and colon absorb large quantities of electrolytes (Na⁺, CI⁻, HCO3], and K⁺), large volume of water. The colon secretes K⁺by a mechanism similar to that in renal distal tubule. The mechanism for fluid and electrolyte absorption and secretion in the intestine involve cellular and paracellular routes. Intestinal epithelial cells lining villi absorb large amount of water and solute. The absorption is always isotonic, which is similar to that in the renal proximal tubule. The solute absorptive mechanism vary among the jejunum, ileum and colon. Jejunum; It is major site for Na⁺ absorption in small intestine. The apical membrane contains Nadependent coupled transports; Na-monosaccahride cotransporters (Na-glucose and Nagalactose),Na-amino acid cotransporters and Na⁺-H⁺ exchange, after Na⁺ enter cell, it is extracted across the basolateral membrane via the Na⁺-K⁺ ATPase. Ileum; The ileum contains same transport mechanism as jejunum plus CI-HCO3 exchange mechanism in the apical membrane and CI⁻ transporter instead HCO3⁻ transporter in the basolateral membrane, for secreting bicarbonate ions in exchange for absorption of chloride ions . This is important because it provides alkaline bicarbonate ions that neutralize acid products formed by bacteria in the large intestine. the Absorption ileum Colon Apical membrane contains Na⁺ and K⁺ channels which responsible for Na⁺ absorption and K⁺secretion, induced by aldosterone which lead to increase Na⁺ absorption and K⁺ secretion electrolyte transport in the colon Large intestine The large intestine frames the small intestines and extends from the ileocecal valve to the anus. Its diameter, is greater than that of the small intestine and it is 1.5m long. The principal functions of the colon are (1) absorption of water and electrolytes from the chyme to form solid feces . (2) storage of fecal matter until it can be expelled. The proximal half of the colon, is concerned with absorption, and the distal half with storage. The large intestine is divided into the cecum, appendix, colon, rectum and the anal canal. Indigestible food residues travels from the cecum, to ascending colon, turns at the right colic (hepatic) flexure, to the transverse colon, turns at the left colic (splenic) flexure, to the descending colon, sigmoid colon, rectum, and finally the anal canal. in colon there are no circular folds and a reduced number of villi. The mucosa is thicker, with a larger number of globet cells. Large intestinal motility: Segmentation contractions(mixing movements) occur as in the small intestine, to mix the contents, in large intestine associated with characteristic sac like segment called haustrations . Mass movement :occur to move the contents of large intestine over long distances, occur 1-3 times per day. Water absorption occur in distal colon, making the fecal contents semisolid. Mass movement propels the fecal contents into rectum where they are stored until defecation occurs. Defecation:Done by two reflexes: 1-Rectosphincteric reflex. As the rectum fills with feces, the smooth muscle wall of rectum contracts to create pressure and the internal anal sphincter relaxes, the feces are forced out through anal canal. 2- Gastrocolic reflex: Distension of the stomach by food increases the motility of the colon and increases the frequency of mass movement in large intestine, this reflex has afferent limb in the stomach which is mediated by parasympathetic nervous system and the efferent limb which increased motility of colon and mediated by CCK (cholecystokinin) and gastrin hormones . As well as the afferent signals entering the spinal cord initiate other effects ,such as taking a deep breath, closure of the glottis ,and contraction of the abdominal muscles to force the fecal contents of the colon downward ,at the same time causing the pelvic floor to extend downward to pull out ward on the anus to evaginate the feces. Secretion of the large intestine: Mucous which is regulated by direct tactile and by local nervous reflexes to mucous cells. Stimulation of pelvic nerve which carry parasyrspathetic to distal two third of large intestine increase secretion of mucous and motility (every 30 minutes). Mucous protect the intestinal wall against excoriation, from the great amount of bacterial activity and provide the adherent medium for holding fecal matter together Absorption in large intestine: The colon ( proximal half) absorbs 2-3 L of water, Na⁺ and Cl⁻ ions per day, and secretes K⁺ ions, and bicarbonate ions to neutralize the acidic end products of bacterial action in colon . In colon the hormone control regulate Na⁺ and K⁺ absorption is aldosterone. Bacterial action in the colon: numerous bacteria such as colon bacilli are present in the absorbing colon Intestinal bacterial flora is harmless unless it enter the blood. The antibodies which are produced by lymphocyte cells (proliferate and differentiate by intestinal antigens) coat the mucous and prevent bacteria from penetrating intestinal wall. The function of bacteria are: 1-Utilize vitamin C, B 12, synthesis vitamin K and B plex. 2- Brown color of stool due to metabolism of bile pigment. The brown color of feces is caused by sterobilin and urobilin which are derivatives of bilirubin 3- Acidity of stool due to formation of organic acid from carbohydrate by bacteria 4- Formation of toxic substances (histamine and tyramine). 5- Formation of indole, in addition to sulfide gives the odder of stool. The oddor is caused by products of bacterial action bile pigment, sloughed epithelial cells and undigested roughage of food.. 6- Formation of ammonia,and various gases that contribute to flatus in colon especially carbon dioxide, hydrogen gas, N2 and methane. The gases produced due to breakdown of undigested nutrients that reach the colon