Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Atherosclerosis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Molecular mimicry wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Innate immune system wikipedia , lookup
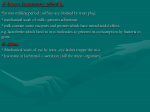
ATVB in Focus Macrophage Diversity in Health and Disease Series Editor: Ann Marie Schmidt Macrophage Polarization at the Crossroad Between HIV-1 Infection and Cancer Development Massimo Alfano, Francesca Graziano, Luca Genovese, Guido Poli Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 Abstract—Mononuclear phagocytes play a fundamental role in the tissue homeostasis and innate defenses against viruses and other microbial pathogens. In addition, they are likely involved in several steps of cancer development. Circulating monocytes and tissue macrophages are target cells of viral infections, including human cytomegalovirus, human herpes virus 8, and the HIV, and alterations of their functional and phenotypic properties are likely involved in many tissue-degenerative diseases, including atherosclerosis and cancer. Different tissue microenvironments as well as their pathological alterations can profoundly affect the polarization state of macrophages toward the extreme phenotypes conventionally termed M1 and M2. Thus, targeting disease-associated macrophages is considered a potential approach particularly in the context of cancer-associated tumor-associated macrophages, supporting malignant cell growth and progression toward a metastatic phenotype. Of note is the fact that tumor-associated macrophages isolated from established tumors display phenotypic and functional features similar to those of in vitro–derived M2-polarized cells. Concerning HIV-1 infection, viral eradication strategies in the context of combination antiretroviral therapy should also consider the possibility to deplete, at least transiently, certain mononuclear phagocytes subsets, although the possibility of distinguishing those that are either infected or pathogenically altered remains a goal of future research. In the present review, we will focus on the recent literature concerning the role of human macrophage polarization in viral infections and cancer. (Arterioscler Thromb Vasc Biol. 2013;33:1145-1152.) Key Words: cancer ◼ HIV ◼ human cytomegalovirus ◼ human herpes virus 8 ◼ M1 ◼ M2 ◼ macrophage ◼ polarization Functional Polarization of Mononuclear Phagocytes (IFN-γ), and are potent effector cells enabled to kill cells infected by intracellular pathogens, including viruses, and tumor cells; they are also sources of proinflammatory cytokines, such as interleukin (IL)-1β, IL-12, IL-15, IL-18, and tumor necrosis factor-α, thus participating to the induction and maintenance of CD4+ T helper cells 1 responses.6,8,9 In addition, M1-cells secrete factors of the Complement cascade and express high levels of major histocompatibility complex class I and class II antigens, thereby enhancing the adaptive immune response to pathogens or tumors.6 In contrast, IL-4, IL-13, glucocorticoid hormones, IL-10, and antigen-antibody (Ab) complexes, in combination with cell stimulation via toll-like receptor, induce M2 functional polarization of tissue macrophages. This activation state is characterized by poor production of nitric oxide (NO), reduced to absent secretion of proinflammatory cytokines coupled with the enhanced ability to scavenge cellular debris, promotion of neoangiogenesis, tissue remodeling, and repair. M2-polarized macrophages have also shown an increased capacity to eliminate extracellular pathogens, including parasites, and participate in the switch of the adaptive immune response toward CD4+ Th2 Mononuclear phagocyte (MP) encompass bone marrow precursor cells and peripheral blood monocytes that, after a very short time (1–2 days), migrate into the different organs and tissues. Under the influence of the different microenvironments, recently migrated monocytes give rise to a variety of MP subtypes, including mucosal macrophages, dendritic cells, and tissue-associated Langherans cells of skin, perivascular macrophages, Kupffer cells of liver, and brain microglial cells.1–5 In addition to their peculiar differentiation phenotypes, tissue macrophages may be activated along 2 main functional pathways.6,7 Proinflammatory stimuli result in classically activated macrophages or M1-cells, which participate to the clearance of either infected or transformed cells, however simultaneously contributing to tissue destruction. Conversely, anti-inflammatory signals induce alternatively activated or M2-macrophages that will activate cellular programs, promoting tissue regeneration and wound healing. M1-macrophages are typically induced by microbial products and proinflammatory cytokines, particularly interferon-γ Received on: January 4, 2013; final version accepted on: March 14, 2013. From the AIDS Immunopathogenesis Unit, Division of Immunology, Transplantation and Infectious Diseases, San Raffaele Scientific Institute, Milan, Italy (M.A., F.G., L.G., G.P.); and Università Vita-Salute San Raffaele, School of Medicine, Milan, Italy (F.G., L.G., G.P.). Correspondence to Guido Poli, P2/P3 Laboratories, DIBIT-1, Via Olgettina n. 58, 20132, Milano, Italy. E-mail [email protected] © 2013 American Heart Association, Inc. Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org 1145 DOI: 10.1161/ATVBAHA.112.300171 1146 Arterioscler Thromb Vasc Biol June 2013 pathways.6 Dominance of M2-polarized macrophages has been also associated with the suppression of antitumor activities.6 M2-macrophages secrete anti-inflammatory molecules, such as the IL-1 receptor antagonist (IL-1ra), IL-10, and transforming growth factor-β, thereby inhibiting the inflammatory burst and the production of proinflammatory cytokines.10 Depending on the activation stimuli, M2-macrophages can be subdivided in 3 partially distinct phenotypes: M2a (resulting from IL-4/13 stimulation), M2b (induced by immune complexes stimulation in the presence of toll-like receptor ligands), and M2c (on exposure of macrophages to anti-inflammatory stimuli, such as glucocorticoid hormones, IL-10, or transforming growth factor-β).11 Thus, macrophage polarization is an important component of both the innate and adaptive immune responses to pathogens and tumor cells, balancing the proinflammatory and antiinflammatory states to fine-tune the most appropriate type and intensity of immune response to a microbial or neoplastic threat. Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 Of Mice and Men…in Macrophage Polarization Mice and humans share ≈80% of orthologous genes, whereas the frequency of mouse genes without any human homolog is <1%.12 Nonetheless, significant differences between mice and humans exist in the development of the immune system as well as in the activation of both the innate and adaptive immune responses. Concerning macrophage polarization, both similarities and differences have been reported between man and mouse, as summarized in the Table. In particular, one of the best surface markers used for determining the distribution and function of mouse macrophages is Ly-71 (F4/80),13,30 which is believed to play an immunoregulatory role through the interaction with an unidentified cellular ligand expressed by other immune effectors cells.31,32 F4/80 expression by tumor-associated macrophages (TAM) has been documented in many types of tumors, either naturally occurring or experimentally induced. To date, no human homolog of F4/80 has been reported, but the closely related molecule epidermal growth factor-like module-containing mucin-like hormone receptor-like 2 provides a sensitive marker for identification of TAM as well as of macrophages in healthy human tissue. CD97 is, conversely, a human macrophage marker also expressed in the mouse and highly similar to epidermal growth factor-like module-containing mucin-like hormone receptor-like 2. Of note, all these antigens belong to the family of G-protein–coupled receptors (R).33,34 M1- and M2-Phenotypic Markers Surprisingly, there are only a few cell surface markers that have been clearly associated with mouse M1-polarization (Table). In contrast, selective and restricted expression of markers typical of alternative macrophage polarization has been described in both human and mouse studies. Murinerestricted macrophage markers of M2-polarization lacking homologs in human include the chitinase-like proteins YM1 and YM2,35,36 members of the glycosyl-hydrolase family 18, for which it has been hypothesized a function either as lectinbinding proteins or cytokines.20 Another murine-restricted macrophage marker of M2-polarization is FIZZ1 (found in inflammatory zone 1),36 for which no human homolog has been described. The M2- and Th2-polarizing cytokine IL-4 upregulates the expression of chemokine ligands (CCLs), such as CCL13, CCL14, CCL17, CCL18, CCL22, and CCL24, from human macrophages. Three of these upregulated chemokines lack murine orthologs, such as CCL14 (only human), CCL18 (for which a pseudogene has been described in the mouse), and CCL23 (showing a low degree of homology with murine CCL6), whereas CCL17 and CCL24, which do have murine orthologs, are exclusively upregulated in humans.20 Finally, some confusion has also been generated by inappropriate use of nomenclature. CCL2 has been described as marker of M2-polarization in murine macrophages, whereas CCL13 is a marker of human M2-phenotype in humans. The situation is complicated by the fact that, in humans, CCL2 is different from CCL13 (homolog of murine CCL2), and it is a marker of M1-polarization. Macrophage Polarization and Viral Infections Pathogens have evolved ingenious strategies to circumvent host immune responses as part of the constant evolutionary process occurring in all living organisms. In this scenario, macrophages are endowed with strategies to neutralize pathogenic challenges, while preserving host integrity. In steady-state conditions, macrophages perform multiple housekeeping functions governed by their differentiation state, tissue distribution, and signals from the microenvironment. As discussed below, an excessive polarization may be associated with comorbidities and be detrimental to the host. Viral pathogens causing chronic diseases, such as human cytomegalovirus (HCMV), human herpes virus 8, and the HIV-1, have evolved strategies to take advantages from macrophage polarization to favor their own survival in the host in a latent state. Macrophage Polarization and HCMV Infection HCMV, also known as human herpes virus 5, is a member of the family of Herpesviridae (Betaherpesvirinae subfamily) and infects 60% to 90% of the adult population, leading to a life-long infection of the host (“herpes is forever…”).37 Infection by HCMV leads to morbidity and mortality in immunocompromized individuals, such as AIDS patients, organ transplant recipients, congenitally infected neonates, and cancer patients undergoing chemotherapy.38 After the initial primary infection of host epithelial cells by contact with HCMV-contaminated body fluids, HCMV replicates and spreads via peripheral blood to disseminate in multiple organs.39 HCMV infection causes a wide range of overt organ diseases, including retinitis, gastro-intestinal symptoms, hepatitis, and interstitial pneumonia attributable to the broad in vivo cellular tropism of the virus.39 Human monocytes are responsible for the systemic spreading of HCMV,38–40 representing primary target in vivo and sites of viral latency and persistence; moreover, tissue macrophages are the most prominent infiltrating cell type found in HCMV-infected organs.41,42 Their aberrant function after HCMV infection has been also implicated in the pathogenesis of atherosclerosis.43,44 Alfano et al Macrophage Polarization, HIV and Cancer 1147 HCMV-activated monocytes exhibit increased secretion of cytokines and chemokines, adhesion to endothelial cells and transendothelial migration, suggesting their predominant M1-polarization,45–47 as confirmed by transcriptional profiling studies of HCMV-infected macrophages.48 The secretion of M1-associated cytokines and chemokines, such as IL-1β, IL-6, and tumor necrosis factor-α, in addition to further shaping macrophages toward an M1-phenotype, enhances virus replication and dissemination.45,46 Macrophage Polarization and Human Herpes Virus 8 Infection in HIV-1+ Individuals Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 Kaposi (angio)sarcoma (KS) is one of the most common tumors in therapy-naïve HIV-1+ males, in whom it may acquire features of tissue damage and spreading not observed in its endemic variant.49,50 The pathogenesis of both endemic and HIV–associated KS has been unequivocally linked to the infection by human herpes virus 8, also termed Kaposi sarcoma–associated herpes virus.24 The role of macrophages in the pathogenesis of AIDS–related KS has been well described, because CD169+ macrophages were found associated to the typical KS lesions.49 The establishment of M1-/T helper cells 1-biased immune responses involving CD8+ T cell activation and leading to the production of T helper cells 1 cytokines that promote the progression of KS is supported by studies showing that administration of IFN-γ or tumor necrosis factor-α to patients with HIV-1+ leads to KS development and disease progression.50,51 Because IFN-γ and other proinflammatory cytokines are produced during HIV-1 infection, together with the progressive state of immunodeficiency, they may contribute to determine the faster progression of KS compared with the disease observed in HIV-negative individuals.51 Macrophage Polarization and HIV-1 Infection HIV-1 is a pathogenic human retrovirus of the lentivirinae subfamily that profoundly dysregulates the human immune system by causing a state of chronic immune activation ultimately leading to a progressive severe immunologic deficiency with depletion of CD4+ helper T cells known as AIDS. During HIV-1 infection, monocytes and macrophages play a fundamental role as viral reservoirs throughout all the stages of disease, promoting both immune dysregulation and virus dissemination and representing, together with CD4+ T cells, one of the major barriers to HIV-1 eradication in the setting of highly controlled virus replication by means of combination antiretroviral therapy.52 In particular, tissue macrophages contribute to the establishment of viral reservoirs as consequence of their ubiquitous distribution, long half-life, relative insensitivity to the cytopathic effects of virus replication (unlike CD4+ T cells) and, finally, to their peculiar capacity of producing and storing mature HIV virions in intracellular compartments of debated origin.53 Indeed, HIV-infected macrophages in tissues are credited to represent a crucial cell population, contributing to the viral spreading particularly during the AIDS phase characterized by a severe CD4+ T cell depletion.54–56 A standing issue is whether different, precommitted monocytes exist.57 In particular, CD16+ monocytes are expanded in blood and tissues during pathological conditions characterized by chronic inflammation, including inflammatory bowel disease, cancer, and AIDS.57 Indeed, CD14+CD16+ monocytes are the predominant subset of monocytes, in which HIV infection is hosted,58 and represent a main vehicle by which the virus passed across the blood–brain barrier to colonize the central nervous system.59 Several authors have investigated the role of cytokines, chemokines, and bacterial products on either the susceptibility of human monocyte–derived macrophages (MDM) to HIV-1 infection or on the functional polarization of these cells. In vitro, HIV-1 infection has been reported to drive human MDM toward an M1-like phenotype,60,61 although unlike that observed after stimulation with lipopolysaccharide, HIV-1–driven polarization does not involve a toll-like receptor–dependent pathway and does not result in the production of proinflammatory cytokines, such as IL-1-β or IL-6 (Figure).60 However, HIV-primed MDM are hyperresponsive to different stimuli, including lipopolysaccharide, CL097 (toll-like receptor 7/8 agonist), and polyinosinic:polycytidylic acid.60 Moreover, HIV-1 infection of human MDM causes an increased secretion of M1-associated chemokines, including CCL3, CCL4, and CCL5 (ligands of the CC-chemokine receptor 5 [CCR5], the main HIV-1 entry coreceptor), and downregulation of M2-associated markers, such as CD163, the mannose receptor CD206, CCL18, and IL-10.60,61 These findings support the hypothesis that HIV-1 infection of macrophages induces or primes their polarization toward a proinflammatory, M1-phenotype likely contributing, among other effects, to the establishment and maintenance of state of chronic activation that is nowadays credited to represent a major determinant of HIV-1 disease progression.62–64 Experimental polarization of human macrophages has been obtained by our group by exposing 5- to 7-day-old MDM to either IFN-γ plus tumor necrosis factor-α (M1) or IL-4 (M2a) for 18 h before HIV-1 infection after removal of the cytokines.14 In these experimental conditions, both M1- and M2a-MDM have shown a decreased capacity to support productive CCR5dependent (R5) HIV-1 replication in comparison with unpolarized MDM (whereas CXC chemokine receptor 4-dependent infection was never observed to be productive in either polarized or unpolarized cells),14 however with important differences between M1 and M2a cells. In fact, a potent restriction of HIV-1 replication occurring at a preintegration level of the viral life cycle was shown in the case of M1−, but not of M2aMDM, and was associated with a downregulation of primary CD4 receptor and with the secretion of CCR5-binding chemokines (CCL3, CCL4, and CCL5) ultimately resulting in decreased levels of HIV-1 DNA synthesis.14 Independently, some microRNA (miR) credited with anti– HIV-1 effects, including miR-28, miR-150, miR-223, and miR-382, have been described as upregulated in MDM stimulated with type-I IFN.40 In this regard, a contribution of miR155 to poly (I:C)-induced anti-HIV-1 effects observed during primary macrophage infection has been recently reported.62–64 In addition, IFN-γ stimulation of human MDM has been shown to increase several natural restriction factors for HIV-1 infection, including tripartite motif5α, cyclophilin A, apolipoprotein B mRNA editing enzyme, catalytic polypeptidelike3G, 3 prime repair exonuclease 1, tripartite motif 22, and Bst-2/theterin.40 1148 Arterioscler Thromb Vasc Biol June 2013 M1-MDM R5 HIV-1 replication HIV-1 attachment and entry receptors Cytokine and chemokine secretion Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 HIV-1 life cycle interference HIV-1 restriction factor expression IFN- γ + TNF- α IL-4, IL-13 Unpolarized MDM M2a-MDM +/- ++++ ++ DC-SIGN (-) CD4 (+/-) CCR5 (++) DC-SIGN (+) CD4 (+++) CCR5 (++) DC-SIGN (+++) CD4 (+) CCR5 (++) IL-6, IL-12, TNF-α, CCL2, CCL3, CCL4, CCL5 CXCL8, CXCL9, CXCL10, CXCL11 low to undetectable IL-1ra, IL-10, CCL13, CCL14, CCL20, CCL22, CCL23 Entry, pre-integration (post-integration) n.a. Post-integration APOBEC3A (APOBEC3G, SAMHD1, TRIM22) APOBEC3G, TRIM22 Undefined Figure. Human monocyte–derived macrophage (MDM) polarization and HIV-1 infection in vitro. The figure summarizes published and unpublished results from our as well as other laboratories.14,15,21,96 DC-SIGN indicates dendritic cell–specific intercellular adhesion molecule-3–grabbing nonintegrin; IFN, interferon; IL, interleukin; n.a., not applicable; TNF, tumor necrosis factor; and TRIM, tripartite motif. In our experience, M2a-polarization of human MDM is characterized by less potent, but more durable inhibition of HIV-1 replication, with no detectable impairment of HIV-1 DNA synthesis,14 therefore implying the induction of an interference mechanism acting at a postintegration level.14,15,40 Recently, we have reported that expression of dendritic cell–specific intercellular adhesion molecule-3grabbing nonintegrin is present and enhanced in unpolarized and M2a-MDM, respectively, whereas it downregulates M1-cells,21 therefore representing a potentially useful marker to distinguish between M1- and M2-macrophages in vivo. Dendritic cell–specific intercellular adhesion molecule3–grabbing nonintegrin expression by M2a-MDM, on the one hand, may compensate for the decreased levels of CD4 on the surface of these cells, but, on the other hand, facilitate virion transmission to CD4+ T cells, in analogy to its already demonstrated role in dendritic cell.65 Therefore, M2apolarization likely induces both restrictive and permissive factors of HIV spreading, unlike M1-cell polarization. In this regard, a distinctive feature between M1- and M2-MDM is their ability to internalize HIV-1 virions, in that it has been reported to be significantly increased in M1-MDM versus M2or unpolarized MDM.66 Such a different endocytic capacity may ultimately affect the different susceptibility of MDM to HIV-1 infection in addition to impact on both their antigenpresenting function and their ability to transfer virions to other target cells.66 Based on the differential profiles of monocyte activation observed in patients at different stages of disease, in 2010 Herbein and Varin have proposed a model, whereby the macrophage activation or polarization state changes during the course of disease, with an M1-phenotype dominating during the early phase of the disease and an M2a-profile emerging during the chronic phase of disease, leading to macrophage deactivation (M2c) in its later stage.67 The introduction of combination antiretroviral therapy has significantly ameliorated the quality of life of infected individuals and prolonged their life expectancy. Such an increased life-span has been, however, associated with a significant change in HIV-1 infection comorbidities, including an increased incidence of solid cancers (discussed later) and of cardiovascular complications, including accelerated atherosclerosis and pulmonary hypertension.68,69 In this regard, the importance of macrophage polarization in the pathogenesis of atherosclerosis, and in particular the switch between the initial phase of atherosclerotic plaque formation, characterized by M2 predominance overturned by murine M1-macrophages with ensuing plaque growth has been discussed elsewhere.70,71 However, such a switch has not been observed in humans, in whom the presence of both M1- and M2-macrophages during human atherosclerotic plaque development has been reported.70,71 Polarized Macrophages and Tumor Pathogenesis TAM have been clearly involved in many events in tumor pathogenesis, although their role is still debated as a function of their intra- versus peritumoral localization and of the reciprocal interaction with malignant and stromal cells in the local microenvironment.72,73 Peritumoral TAM displaying a proinflammatory M1-like phenotype (ie, expressing cytokines, such as IFN-γ, IL-1β, and IL-6, and favoring antitumor immune Alfano et al Macrophage Polarization, HIV and Cancer 1149 Table. Expression of Cell Surface and Soluble Antigens Associated With Murine and Human Functional Macrophage (Mø) Polarization Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 Mø Mouse Human M1 Cell surface: CD16 (FcγRIII), CD86, MHC-II antigens Soluble: CXCL9, CXCL10, CXCL11, TNF-α Other: iNOS Cell surface: CD4 (downregulation), CCR7, IL-2Rα, IL-15Rα, CD80, CD86, MHX-II antigens, TLR2, TLR4 Soluble: CCL2, CCL3, CCL4, CCL5, CCL20, CXCL8, CXCL9, CXCL16, IL-1β, IL-7, IL-12, IL-18, IL-23, TNF-α, ROI Other: iNOS References M2 Cell surface: scavenger R, MRC1 Soluble: CCL2, CCL22, IL-10, YM1, YM2, FIZZ1 Other: Arginase1, HO-1 Cell surface: CD36, CD163, CXCR1, CXCR2, Dectin-1, DCL-1, SR-A, DCIR/ 9,15,16,20–23 LLIR, Scavenger R, MRC1, BIGH-H3, β2 integrins, DC-SIGN Soluble: CCL1, CCL13, CCL14, CCL17, CCL18, CCL20, CCL22, CCL23, CCL24, IL1ra, IL-10, IGF Other: Fibronectin, SPHK1, HO-1 TAM Cell surface: CD11b, CD14, CD36, CD45, CD68, CD97, CD163, CD200/ CD200R, CD204, CD206, CCR1, CCR2, CXCR1, IL-4/IL-13R, CSF1R, MHC-II antigens, VEGFR1, CR3, FcR, SR-A, MARCO, Mannose R, Dectin-1, Dectin-2, TLRs, F4/80 (Ly-71) antigen Soluble: CCL2, CCL5, CCL13, CCL22, CXCL9, CXCL10, CXCL16, IL-10 Other: HO-1 Cell surface: CD4 (downregulation), CD11b, CD14, CD23, CD36, CD45, CD68, CD97, CD163, CD200/CD200R, CD204, CD206, CCR1, CCR2, CXCR1, CXCR4, IL-4/13R, CSF1R, MHC-II antigens, VEGFR1, CR3, FcR, SR-A, MARCO, Mannose R, Dectin-1, Dectin-2, TLRs, MMP2, MMP9, B7H4, FRb, EMR2 Soluble: IL-6, IL-10, IL-12, TNF-α, CCL2, CCL5, CCL13, CCL18, CCL22, CXCL9, CXCL10, CXCL16 Other: STAT-3 9,13–19 3,22,24–29 Upregulated expression of M1 or M2 markers vs unpolarized cells was mainly obtained from in vitro studies. Markers of TAM were defined from ex vivo studies and compared in terms of expression with the levels observed in macrophages isolated from tumor-free tissue. In bold are indicated markers shared by murine and human MDM. CR3 indicates complement R3; CSF1R, colony stimulating factor 1 R; DCIR/LLIR, lectin-like immunoreceptor; DCL1, DEC-205-associated C-type lectin-1; EMR2, epidermal growth factor-like module-containing mucin-like hormone receptor-like 2; FRb, folate R b; HO-1, heme oxygenase-1; IGF, insulin growth factor; IL-1ra, IL-1 receptor antagonist; MDM, monocyte-derived macrophage; MHC, major histocompatibility complex; MMP, matrix metalloproteinase; MRC1, mannose R mannose R, C type 1; ROI, reactive oxygen intermediates; SPHK1, sphingosine kinase 1; SR-A, scavenger R class A; STAT-3, signal transducer and activator of transcription 3; TLR, toll-like receptor; and VEGFR1, vascular endothelial growth factor R1. response by T helper 1 cells)74 have been associated with prevention of tumor development and a good prognosis.75–78 The complexity of the role of M1-polarized macrophages in the context of cancer development is illustrated by the observation that, on the one hand, M1-polarized TAM promote expression of galectin-3 by colon tumor cell that further induce more macrophage infiltration leading to an amplification of immune responses against tumor cells,74 but, on the other hand, they contribute to the maintenance of chronic inflammation that leads to accumulation of DNA mutations favoring early steps of tumorigenesis. Conversely, intratumoral TAM cell count has been correlated with depth of invasion, lymph node metastasis, and staging of colorectal carcinoma, suggesting that intratumoral macrophages may promote a more aggressive behavior of cancer cells.79,80 Overall, most studies on different malignant cancers, including lymphomas, intestinal type gastric cancers, pancreatic cancers, nongynecologic leiomyosarcomas, and thyroid cancers, indicate that the presence of anti-inflammatory TAM in the tumor microenvironment is associated with a worse prognosis. In this regard, TAM are believed to orchestrate various aspects of cancer biology, such as tumor progression, angiogenesis, tumor growth, and actual metastasis in a context of immunosuppression.72,81,82 In particular, TAM represent variants of a general M2-polarization phenotype based on the expression of a series of markers, such as CD163, the R for Fc fragment of IgG, C-type lectin domain proteins, and heat shock proteins characteristically expressed by alternatively activated macrophages.83–85 In addition, the tumor microenvironment is characterized by the presence of several anti-inflammatory cytokines, such as IL-4, IL-10, IL-13, and transforming growth factor-β, that lead resident or recently migrated macrophages to adopt an M2-phenotype.86 In addition to growth factors, cytokines, and chemokines, TAM (M2) express molecules, which affect tumor cell proliferation, angiogenesis, and dissolution of connective tissues, such as matrix metallo-proteinases, thus contributing to matrix degradation needed for promoting angiogenesis and release of growth factors,87 plasmin, and urokinasetype plasminogen activator and its receptors urokinase-type plasminogen activator receptor.7,87 Translational Medicine: A Role for Macrophage Polarization in Cancer Therapy? This review focuses on the important roles of macrophages in viral infection and cancer, which qualifies them as potential druggable targets, aiming at decreasing macrophage accumulation, inducing their depletion, suppressing TAM-induced tumor angiogenesis, reprogramming macrophage polarization, and using these cells as functional vehicles. TAM are today considered putative targets for therapeutic intervention.81 In this regard, destruction of tissue macrophages with clodronate-loaded liposomes has also been shown to inhibit several tumorigenic steps, although this strategy has been investigated only in animal models, whereas the use of bisphosphonates in humans has been associated with severe adverse events.88 Furthermore, persistent depletion of macrophages could also potentially expose individuals to acquire 1150 Arterioscler Thromb Vasc Biol June 2013 Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 more easily mycobacterioses and other infectious diseases.88 As alternative approach, promotion of a switch of TAM polarization from M2 to M1 has also been investigated as strategy to reduce tumor growth and invasion.9 IFN-γ administration was observed to activate a tumoricidal activity of TAM in a large clinical study in patients with ovarian cancer by inducing a phenotypic switch.89 A recent study performed in a pancreatic ductal adenocarcinoma model has reported that anti-CD40 Abs promoted an antitumor effect and induced high expression of M1-associated markers (such as major histocompatibility complex class II antigens and CD86) in macrophages.90 Zolendronic acid has been shown to inhibit macrophage migration, proliferation, and secretion of tumor-promoting factors, such as matrix metallo-proteinases 9. Furthermore, both zoledronic acid, C phosphate G, antiIL10 and anti-IL10 receptor reversed the M2-polarization bias of TAM; in the case of Zolendronic acid, this was associated with an increased expression of inducible NO and with the downregulating of IL-10 and vascular endothelial growth factor secretion.91,92 In addition, the plasma protein histidine-rich glycoprotein, endowed with antiangiogenesis effect, induced TAM polarization toward an M1-like phenotype by inducing the downregulation of the placental growth factor, a member of the vascular endothelial growth factor family.93 In mice, histidine-rich glycoprotein promoted antitumor immune response and normalization of the vessel network.93 Other therapeutic strategies focused to affect macrophages polarization include trabectedin94 and statins.95 Conclusions The MP system is central to both the innate and adaptive immune responses to microbial invaders and cancer cells. Its well known plasticity can be transiently overcome by the possibility of polarizing its activation profile according to a range of variable functional aspects at the extreme poles, of which there are M1 and M2 opposite programs of macrophage activation. In the case of HIV-1 infection, although M1-polarization does not prevent the in vitro infection of these cells, it creates a hostile environment for retrovirus replication affecting multiple steps of its life cycle, both at pre- and (likely) postintegration levels, while, at the same time, the increased expression of major histocompatibility complex class II antigens and of secreted factors could potentially favor the clearance of infected cells by the adaptive arm of the immune system. Similar considerations could be made for the role of MP polarization in cancer cell biology and progression, converging to a general picture, in which MP tend to occupy a more prominent role than earlier suspected in the pathogenesis of these prominent diseases affecting mankind. Acknowledgments We thank Edana Cassol and Luca Cassetta, who have established the M1/M2-polarization model of HIV infection in our laboratory and Antonio Sica (Humanitas Clinical and Research Center, Milano) for his helpful suggestions. F. Graziano and L. Genovese performed this study as partial fulfillment of their PhD of the International PhD School in Molecular Medicine, Università Vita-Salute San Raffaele, Milano, Italy. Sources of Funding This article was supported in part by the grants to M. Alfano and G. Poli from the Italian Ministry of Health Grant Program of AIDS Research 2009 to 2010. Disclosures None. References 1. Collman RG, Perno CF, Crowe SM, Stevenson M, Montaner LJ. HIV and cells of macrophage/dendritic lineage and other non-T cell reservoirs: new answers yield new questions. J Leukoc Biol. 2003;74:631–634. 2. Gendelman HE, Orenstein JM, Baca LM, Weiser B, Burger H, Kalter DC, Meltzer MS. The macrophage in the persistence and pathogenesis of HIV infection. AIDS. 1989;3:475–495. 3.Gray F, Bélec L, Chrétien F, Dubreuil-Lemaire ML, Ricolfi F, Wingertsmann L, Poron F, Gherardi R. Acute, relapsing brain oedema with diffuse blood-brain barrier alteration and axonal damage in the acquired immunodeficiency syndrome. Neuropathol Appl Neurobiol. 1998;24:209–216. 4. Mann DL, Gartner S, Le Sane F, Buchow H, Popovic M. HIV-1 transmission and function of virus-infected monocytes/macrophages. J Immunol. 1990;144:2152–2158. 5. Stevenson M, Gendelman HE. Cellular and viral determinants that regulate HIV-1 infection in macrophages. J Leukoc Biol. 1994;56:278–288. 6. Mantovani A, Sica A, Sozzani S, Allavena P, Vecchi A, Locati M. The chemokine system in diverse forms of macrophage activation and polarization. Trends Immunol. 2004;25:677–686. 7. Mantovani A, Sozzani S, Locati M, Allavena P, Sica A. Macrophage polarization: tumor-associated macrophages as a paradigm for polarized M2 mononuclear phagocytes. Trends Immunol. 2002;23:549–555. 8. Goerdt S, Politz O, Schledzewski K, Birk R, Gratchev A, Guillot P, Hakiy N, Klemke CD, Dippel E, Kodelja V, Orfanos CE. Alternative versus classical activation of macrophages. Pathobiology. 1999;67:222–226. 9. Sica A, Mantovani A. Macrophage plasticity and polarization: in vivo veritas. J Clin Invest. 2012;122:787–795. 10. Abramson SL, Gallin JI. IL-4 inhibits superoxide production by human mononuclear phagocytes. J Immunol. 1990;144:625–630. 11. Martinez FO, Sica A, Mantovani A, Locati M. Macrophage activation and polarization. Front Biosci. 2008;13:453–461. 12. Guénet JL. The mouse genome. Genome Res. 2005;15:1729–1740. 13. Taylor PR, Martinez-Pomares L, Stacey M, Lin HH, Brown GD, Gordon S. Macrophage receptors and immune recognition. Annu Rev Immunol. 2005;23:901–944. 14. Cassol E, Cassetta L, Rizzi C, Alfano M, Poli G. M1 and M2a polarization of human monocyte-derived macrophages inhibits HIV-1 replication by distinct mechanisms. J Immunol. 2009;182:6237–6246. 15.Cassol E, Cassetta L, Alfano M, Poli G. Macrophage polarization and HIV-1 infection. J Leukoc Biol. 2010;87:599–608. 16. Ricardo SD, van Goor H, Eddy AA. Macrophage diversity in renal injury and repair. J Clin Invest. 2008;118:3522–3530. 17. Quiding-Järbrink M, Raghavan S, Sundquist M. Enhanced M1 macrophage polarization in human helicobacter pylori-associated atrophic gastritis and in vaccinated mice. PLoS One. 2010;5:e15018. 18. Edin S, Wikberg ML, Dahlin AM, Rutegård J, Öberg Å, Oldenborg PA, Palmqvist R. The distribution of macrophages with a M1 or M2 phenotype in relation to prognosis and the molecular characteristics of colorectal cancer. PLoS One. 2012;7:e47045. 19.Schmieder A, Michel J, Schönhaar K, Goerdt S, Schledzewski K. Differentiation and gene expression profile of tumor-associated macrophages. Semin Cancer Biol. 2012;22:289–297. 20.Martinez FO, Helming L, Gordon S. Alternative activation of macrophages: an immunologic functional perspective. Annu Rev Immunol. 2009;27:451–483. 21. Cassol E, Cassetta L, Rizzi C, Gabuzda D, Alfano M, Poli G. Dendritic cell-specific icam-3 grabbing nonintegrin mediates hiv-1 infection of and transmission by m2a-polarized macrophages in vitro. Aids. 2012 22.Kuroda E, Yoshida Y, En Shan B, Yamashita U. Suppression of macrophage interleukin-12 and tumour necrosis factor-alpha production in mice infected with Toxocara canis. Parasite Immunol. 2001;23:305–311. Alfano et al Macrophage Polarization, HIV and Cancer 1151 Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 23. Mantovani A, Schioppa T, Porta C, Allavena P, Sica A. Role of tumorassociated macrophages in tumor progression and invasion. Cancer Metastasis Rev. 2006;25:315–322. 24. Bhatia K, Shiels MS, Berg A, Engels EA. Sarcomas other than Kaposi sarcoma occurring in immunodeficiency: interpretations from a systematic literature review. Curr Opin Oncol. 2012;24:537–546. 25. Kwakkenbos MJ, Kop EN, Stacey M, Matmati M, Gordon S, Lin HH, Hamann J. The EGF-TM7 family: a postgenomic view. Immunogenetics. 2004;55:655–666. 26. Kwakkenbos MJ, Matmati M, Madsen O, Pouwels W, Wang Y, Bontrop RE, Heidt PJ, Hoek RM, Hamann J. An unusual mode of concerted evolution of the EGF-TM7 receptor chimera EMR2. FASEB J. 2006;20:2582–2584. 27. Heusinkveld M, van der Burg SH. Identification and manipulation of tumor associated macrophages in human cancers. J Transl Med. 2011;9:216. 28. Joyce JA, Pollard JW. Microenvironmental regulation of metastasis. Nat Rev Cancer. 2009;9:239–252. 29. Lin H-H, Gordon S. Macrophage phenotype in tumours. In: Lawrence L, Hagemann T, editors.Tumor-Associated Macrophages. New York, NY: Springer Science. 2012:3–16. 30. Austyn JM, Gordon S. F4/80, a monoclonal antibody directed specifically against the mouse macrophage. Eur J Immunol. 1981;11:805–815. 31. Lin HH, Faunce DE, Stacey M, Terajewicz A, Nakamura T, Zhang-Hoover J, Kerley M, Mucenski ML, Gordon S, Stein-Streilein J. The macrophage F4/80 receptor is required for the induction of antigen-specific efferent regulatory T cells in peripheral tolerance. J Exp Med. 2005;201:1615–1625. 32. van den Berg TK, Kraal G. A function for the macrophage F4/80 molecule in tolerance induction. Trends Immunol. 2005;26:506–509. 33. McKnight AJ, Gordon S. EGF-TM7: a novel subfamily of seven-transmembrane-region leukocyte cell-surface molecules. Immunol Today. 1996;17:283–287. 34.Bjarnadóttir TK, Fredriksson R, Schiöth HB. The adhesion GPCRs: a unique family of G protein-coupled receptors with important roles in both central and peripheral tissues. Cell Mol Life Sci. 2007;64:2104–2119. 35. Chang NC, Hung SI, Hwa KY, Kato I, Chen JE, Liu CH, Chang AC. A macrophage protein, Ym1, transiently expressed during inflammation is a novel mammalian lectin. J Biol Chem. 2001;276:17497–17506. 36. Raes G, De Baetselier P, Noël W, Beschin A, Brombacher F, Hassanzadeh Gh G. Differential expression of FIZZ1 and Ym1 in alternatively versus classically activated macrophages. J Leukoc Biol. 2002;71:597–602. 37.Jarvis MA, Nelson JA. Molecular basis of persistence and latency. In: Arvin A, Campadelli-Fiume G, Mocarski E, Moore PS, Roizman B, Whitley R, Yamanishi K, editors. Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge: Cambridge University Press; 2007. 38. Sinclair J, Sissons P. Latent and persistent infections of monocytes and macrophages. Intervirology. 1996;39:293–301. 39. Sinzger C, Jahn G. Human cytomegalovirus cell tropism and pathogenesis. Intervirology. 1996;39:302–319. 40. Jiménez VC, Booiman T, de Taeye SW, van Dort KA, Rits MA, Hamann J, Kootstra NA. Differential expression of HIV-1 interfering factors in monocyte-derived macrophages stimulated with polarizing cytokines or interferons. Sci Rep. 2012;2:763. 41. Booss J, Dann PR, Griffith BP, Kim JH. Host defense response to cytomegalovirus in the central nervous system. Predominance of the monocyte. Am J Pathol. 1989;134:71–78. 42.Pulliam L. Cytomegalovirus preferentially infects a monocyte derived macrophage/microglial cell in human brain cultures: neuropathology differs between strains. J Neuropathol Exp Neurol. 1991;50:432–440. 43. Degré M. Has cytomegalovirus infection any role in the development of atherosclerosis? Clin Microbiol Infect. 2002;8:191–195. 44. Streblow DN, Orloff SL, Nelson JA. Do pathogens accelerate atherosclerosis? J Nutr. 2001;131:2798S–2804S. 45. Smith MS, Bentz GL, Alexander JS, Yurochko AD. Human cytomegalovirus induces monocyte differentiation and migration as a strategy for dissemination and persistence. J Virol. 2004;78:4444–4453. 46. Smith MS, Bentz GL, Smith PM, Bivins ER, Yurochko AD. HCMV activates PI(3)K in monocytes and promotes monocyte motility and transendothelial migration in a PI(3)K-dependent manner. J Leukoc Biol. 2004;76:65–76. 47.Yurochko AD, Huang ES. Human cytomegalovirus binding to human monocytes induces immunoregulatory gene expression. J Immunol. 1999;162:4806–4816. 48.Chan G, Bivins-Smith ER, Smith MS, Smith PM, Yurochko AD. Transcriptome analysis reveals human cytomegalovirus reprograms monocyte differentiation toward an M1 macrophage. J Immunol. 2008;181: 698–711. 49.Cornelissen M, van der Kuyl AC, van den Burg R, Zorgdrager F, van Noesel CJ, Goudsmit J. Gene expression profile of AIDS-related Kaposi’s sarcoma. BMC Cancer. 2003;3:7. 50. Monini P, Colombini S, Stürzl M, et al. Reactivation and persistence of human herpesvirus-8 infection in B cells and monocytes by Th-1 cytokines increased in Kaposi’s sarcoma. Blood. 1999;93:4044–4058. 51. Ensoli B, Sgadari C, Barillari G, Sirianni MC, Stürzl M, Monini P. Biology of Kaposi’s sarcoma. Eur J Cancer. 2001;37:1251–1269. 52. Deeks SG, Autran B, Berkhout B, et al. Towards an hiv cure: a global scientific strategy. Nat Rev Immunol. 2012;12:607–614 53.Orenstein JM. Replication of HIV-1 in vivo and in vitro. Ultrastruct Pathol. 2007;31:151–167. 54. Carter CA, Ehrlich LS. Cell biology of HIV-1 infection of macrophages. Annu Rev Microbiol. 2008;62:425–443. 55. Morrow G, Vachot L, Vagenas P, Robbiani M. Current concepts of HIV transmission. Curr HIV/AIDS Rep. 2007;4:29–35. 56. Wahl SM, Greenwell-Wild T, Vázquez N. HIV accomplices and adversaries in macrophage infection. J Leukoc Biol. 2006;80:973–983. 57. Ziegler-Heitbrock L. The CD14+ CD16+ blood monocytes: their role in infection and inflammation. J Leukoc Biol. 2007;81:584–592. 58. Jaworowski A, Kamwendo DD, Ellery P, Sonza S, Mwapasa V, Tadesse E, Molyneux ME, Rogerson SJ, Meshnick SR, Crowe SM. CD16+ monocyte subset preferentially harbors HIV-1 and is expanded in pregnant Malawian women with Plasmodium falciparum malaria and HIV-1 infection. J Infect Dis. 2007;196:38–42. 59. Williams DW, Eugenin EA, Calderon TM, Berman JW. Monocyte maturation, HIV susceptibility, and transmigration across the blood brain barrier are critical in HIV neuropathogenesis. J Leukoc Biol. 2012;91:401–415. 60. Brown JN, Kohler JJ, Coberley CR, Sleasman JW, Goodenow MM. HIV-1 activates macrophages independent of Toll-like receptors. PLoS One. 2008;3:e3664. 61.Porcheray F, Samah B, Léone C, Dereuddre-Bosquet N, Gras G. Macrophage activation and human immunodeficiency virus infection: HIV replication directs macrophages towards a pro-inflammatory phenotype while previous activation modulates macrophage susceptibility to infection and viral production. Virology. 2006;349:112–120. 62. Graff JW, Dickson AM, Clay G, McCaffrey AP, Wilson ME. Identifying functional microRNAs in macrophages with polarized phenotypes. J Biol Chem. 2012;287:21816–21825. 63.Martinez-Nunez RT, Louafi F, Friedmann PS, Sanchez-Elsner T. MicroRNA-155 modulates the pathogen binding ability of dendritic cells (DCs) by down-regulation of DC-specific intercellular adhesion molecule-3 grabbing non-integrin (DC-SIGN). J Biol Chem. 2009;284:16334–16342. 64. Swaminathan G, Rossi F, Sierra LJ, Gupta A, Navas-Martín S, Martín-García J. A role for microRNA-155 modulation in the anti-HIV-1 effects of Tolllike receptor 3 stimulation in macrophages. PLoS Pathog. 2012;8:e1002937. 65. van der Vlist M, van der Aar AM, Gringhuis SI, Geijtenbeek TB. Innate signaling in HIV-1 infection of dendritic cells. Curr Opin HIV AIDS. 2011;6:348–352. 66. Gobeil LA, Lodge R, Tremblay MJ. Differential HIV-1 endocytosis and susceptibility to virus infection in human macrophages correlate with cell activation status. J Virol. 2012;86:10399–10407. 67. Herbein G, Varin A. The macrophage in HIV-1 infection: from activation to deactivation? Retrovirology. 2010;7:33. 68.Khallou-Laschet J, Varthaman A, Fornasa G, Compain C, Gaston AT, Clement M, Dussiot M, Levillain O, Graff-Dubois S, Nicoletti A, Caligiuri G. Macrophage plasticity in experimental atherosclerosis. PLoS One. 2010;5:e8852. 69. Zanni MV, Grinspoon SK. HIV-specific immune dysregulation and atherosclerosis. Curr HIV/AIDS Rep. 2012;9:200–205. 70.Stöger JL, Goossens P, de Winther MP. Macrophage heterogeneity: relevance and functional implications in atherosclerosis. Curr Vasc Pharmacol. 2010;8:233–248. 71. Stöger JL, Gijbels MJ, van der Velden S, Manca M, van der Loos CM, Biessen EA, Daemen MJ, Lutgens E, de Winther MP. Distribution of macrophage polarization markers in human atherosclerosis. Atherosclerosis. 2012;225:461–468. 72. Qian BZ, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141:39–51. 73. Ruffell B, DeNardo DG, Affara NI, Coussens LM. Lymphocytes in cancer development: polarization towards pro-tumor immunity. Cytokine Growth Factor Rev. 2010;21:3–10. 74. Dumont P, Berton A, Nagy N, Sandras F, Tinton S, Demetter P, Mascart F, Allaoui A, Decaestecker C, Salmon I. Expression of galectin-3 in the tumor immune response in colon cancer. Lab Invest. 2008;88:896–906. 1152 Arterioscler Thromb Vasc Biol June 2013 Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 75. Khorana AA, Ryan CK, Cox C, Eberly S, Sahasrabudhe DM. Vascular endothelial growth factor, CD68, and epidermal growth factor receptor expression and survival in patients with Stage II and Stage III colon carcinoma: a role for the host response in prognosis. Cancer. 2003;97:960–968. 76. Oberg A, Samii S, Stenling R, Lindmark G. Different occurrence of CD8+, CD45R0+, and CD68+ immune cells in regional lymph node metastases from colorectal cancer as potential prognostic predictors. Int J Colorectal Dis. 2002;17:25–29. 77. Zhou Q, Peng RQ, Wu XJ, Xia Q, Hou JH, Ding Y, Zhou QM, Zhang X, Pang ZZ, Wan DS, Zeng YX, Zhang XS. The density of macrophages in the invasive front is inversely correlated to liver metastasis in colon cancer. J Transl Med. 2010;8:13. 78.Funada Y, Noguchi T, Kikuchi R, Takeno S, Uchida Y, Gabbert HE. Prognostic significance of CD8+ T cell and macrophage peritumoral infiltration in colorectal cancer. Oncol Rep. 2003;10:309–313. 79. Kang JC, Chen JS, Lee CH, Chang JJ, Shieh YS. Intratumoral macrophage counts correlate with tumor progression in colorectal cancer. J Surg Oncol. 2010;102:242–248. 80. Pancione M, Forte N, Sabatino L, Tomaselli E, Parente D, Febbraro A, Colantuoni V. Reduced beta-catenin and peroxisome proliferator-activated receptor-gamma expression levels are associated with colorectal cancer metastatic progression: correlation with tumor-associated macrophages, cyclooxygenase 2, and patient outcome. Hum Pathol. 2009;40:714–725. 81. Sica A, Larghi P, Mancino A, Rubino L, Porta C, Totaro MG, Rimoldi M, Biswas SK, Allavena P, Mantovani A. Macrophage polarization in tumour progression. Semin Cancer Biol. 2008;18:349–355. 82. Condeelis J, Pollard JW. Macrophages: obligate partners for tumor cell migration, invasion, and metastasis. Cell. 2006;124:263–266. 83. Biswas SK, Gangi L, Paul S, Schioppa T, Saccani A, Sironi M, Bottazzi B, Doni A, Vincenzo B, Pasqualini F, Vago L, Nebuloni M, Mantovani A, Sica A. A distinct and unique transcriptional program expressed by tumorassociated macrophages (defective NF-kappaB and enhanced IRF-3/ STAT1 activation). Blood. 2006;107:2112–2122. 84.Sakai Y, Honda M, Fujinaga H, Tatsumi I, Mizukoshi E, Nakamoto Y, Kaneko S. Common transcriptional signature of tumor-infiltrating mononuclear inflammatory cells and peripheral blood mononuclear cells in hepatocellular carcinoma patients. Cancer Res. 2008;68:10267–10279. 85.Beck AH, Espinosa I, Edris B, Li R, Montgomery K, Zhu S, Varma S, Marinelli RJ, van de Rijn M, West RB. The macrophage colony-stimulating factor 1 response signature in breast carcinoma. Clin Cancer Res. 2009;15:778–787. 86.Sica A, Saccani A, Mantovani A. Tumor-associated macrophages: a molecular perspective. Int Immunopharmacol. 2002;2:1045–1054. 87.Coussens LM, Tinkle CL, Hanahan D, Werb Z. MMP-9 supplied by bone marrow-derived cells contributes to skin carcinogenesis. Cell. 2000;103:481–490. 88. Baay M, Brouwer A, Pauwels P, Peeters M, Lardon F. Tumor cells and tumor-associated macrophages: secreted proteins as potential targets for therapy. Clin Dev Immunol. 2011;2011:565187. 89.Duluc D, Corvaisier M, Blanchard S, Catala L, Descamps P, Gamelin E, Ponsoda S, Delneste Y, Hebbar M, Jeannin P. Interferon-gamma reverses the immunosuppressive and protumoral properties and prevents the generation of human tumor-associated macrophages. Int J Cancer. 2009;125:367–373. 90.Beatty GL, Chiorean EG, Fishman MP, Saboury B, Teitelbaum UR, Sun W, Huhn RD, Song W, Li D, Sharp LL, Torigian DA, O’Dwyer PJ, Vonderheide RH. CD40 agonists alter tumor stroma and show efficacy against pancreatic carcinoma in mice and humans. Science. 2011;331:1612–1616. 91. Coscia M, Quaglino E, Iezzi M, Curcio C, Pantaleoni F, Riganti C, Holen I, Mönkkönen H, Boccadoro M, Forni G, Musiani P, Bosia A, Cavallo F, Massaia M. Zoledronic acid repolarizes tumour-associated macrophages and inhibits mammary carcinogenesis by targeting the mevalonate pathway. J Cell Mol Med. 2010;14:2803–2815. 92. Huang Z, Zhang Z, Jiang Y, Zhang D, Chen J, Dong L, Zhang J. Targeted delivery of oligonucleotides into tumor-associated macrophages for cancer immunotherapy. J Control Release. 2012;158:286–292. 93. Rolny C, Mazzone M, Tugues S, et al. HRG inhibits tumor growth and metastasis by inducing macrophage polarization and vessel normalization through downregulation of PlGF. Cancer Cell. 2011;19:31–44. 94. Germano G, Frapolli R, Simone M, et al. Antitumor and anti-inflammatory effects of trabectedin on human myxoid liposarcoma cells. Cancer Res. 2010;70:2235–2244. 95. Fujita E, Shimizu A, Masuda Y, Kuwahara N, Arai T, Nagasaka S, Aki K, Mii A, Natori Y, Iino Y, Katayama Y, Fukuda Y. Statin attenuates experimental anti-glomerular basement membrane glomerulonephritis together with the augmentation of alternatively activated macrophages. Am J Pathol. 2010;177:1143–1154. 96. Cassetta L, Cassol E, Poli G. Macrophage polarization in health and disease. ScientificWorldJournal. 2011;11:2391–2402. Downloaded from http://atvb.ahajournals.org/ by guest on June 18, 2017 Macrophage Polarization at the Crossroad Between HIV-1 Infection and Cancer Development Massimo Alfano, Francesca Graziano, Luca Genovese and Guido Poli Arterioscler Thromb Vasc Biol. 2013;33:1145-1152 doi: 10.1161/ATVBAHA.112.300171 Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2013 American Heart Association, Inc. All rights reserved. Print ISSN: 1079-5642. Online ISSN: 1524-4636 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://atvb.ahajournals.org/content/33/6/1145 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online at: http://atvb.ahajournals.org//subscriptions/