Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Fatty acid metabolism wikipedia , lookup
Expression vector wikipedia , lookup
Ribosomally synthesized and post-translationally modified peptides wikipedia , lookup
Magnesium transporter wikipedia , lookup
Ancestral sequence reconstruction wikipedia , lookup
Interactome wikipedia , lookup
Metalloprotein wikipedia , lookup
Western blot wikipedia , lookup
Nuclear magnetic resonance spectroscopy of proteins wikipedia , lookup
Point mutation wikipedia , lookup
Protein purification wikipedia , lookup
Protein–protein interaction wikipedia , lookup
Genetic code wikipedia , lookup
Biosynthesis wikipedia , lookup
Two-hybrid screening wikipedia , lookup
Amino acid synthesis wikipedia , lookup
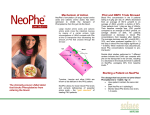
The introduction and use of PKU sphere™, a Glycomacropeptide (GMP) based protein substitute, in children and adults with PKU Vitaflo in Association With You Supporting education in the dietary management of rare diseases Disclaimer These guidelines should be read in conjunction with local guidelines for the dietary management of Phenylketonuria (PKU). They are based on the most recent scientific evidence available on the use of GMP based protein substitutes in PKU. PKU sphere is a protein substitute consisting of a blend of GMP and free amino acids (GMP-AA) for use in the dietary management of children 6 years + and adults with PKU. These guidelines are for use by health care professionals working with children and adults diagnosed with PKU. They are not for use by parents/caregivers of children or adults with PKU. They are for general information only and must not be used as a substitute for professional medical advice. Any product information contained in these guidelines, although accurate at the time of publication, is subject to change. The most current product information may be obtained by referring to product labels. PKU sphere is a food for special medical purposes (FSMP) to be used under medical supervision. PKU sphere is not suitable as a sole source of nutrition and is designed to supplement a low phenylalanine (Phe) diet. A low Phe diet should provide essential Phe requirements, energy, nutrients and water to supply fluid and general nutritional requirements. PKU sphere contains Phe - 36mg per 20g PE; this must be taken into consideration when introducing PKU sphere into the dietary management of PKU. The example for introducing PKU sphere in section 2.3A is based on data from a clinical trial (soon to be published) where natural protein/exchanges remained the same throughout introduction of PKU sphere. Introducing PKU sphere gradually, in a systematic way, allows monitoring of metabolic control and discussion with patient/caregiver at each step. It is the responsibility of the managing health care professional to use their clinical judgment to introduce PKU sphere in the most appropriate way for their individual patients. Allergies/intolerances As GMP is the dominant protein source in PKU sphere and it is derived from cow’s milk there may be a risk of a reaction for those with cow’s milk allergy. Collaborators Vitaflo® dietitians in collaboration with: Professor Anita MacDonald PhD, BSc, OBE (Consultant Dietitian, Birmingham Children’s Hospital, UK) Anne Daly MSc, RD (Senior metabolic dietitian, Birmingham Children’s Hospital, UK) 1 Contents Foreword 3.0 Example case Study 1.0 GMP 1.1 What is GMP and how is it produced? 4.0 Guideline references 1.2 What is PKU sphere? 1.3 Features of PKU sphere 5.0 Appendices 5.1 Appendix 1 – Summary of references related to GMP potential benefits 2.0 Application of PKU sphere 2.1 Who is PKU sphere for? 5.2 Appendix 2 – Safety of GMP 2.2 Considerations for the use of PKU sphere 5.3 Appendix 3 – Why is GMP classed as a whole protein? 2.3 How to introduce PKU sphere A. For an individual with good metabolic control B. For an individual on a relaxed or non-adherent diet 2.4 Practical points and troubleshooting Abbreviations AA Amino acids. GMP Glycomacropeptide. GMP-AA Protein substitutes based on GMP supplemented with the limiting free amino acids +/- micronutrients and essential fatty acids. May vary in format - powder, liquid or bar. L-AA supplement Phenylalanine free protein substitutes based on synthetic amino acids +/ micronutrients and essential fatty acids. May be powder, liquid, bar or tablet. LNAAs Large neutral amino acids. PE Protein equivalent. Phe Phenylalanine. PS Protein substitute. Unmodified GMP Glycomacropeptide as a raw material isolated from cheese whey. 2 Foreword In the 1950’s, the first protein substitute (PS), which was based on protein hydrolysate, was developed to treat the first patient with PKU managed with diet therapy1. For the last 30 years, the most commonly used PS have been Phe-free L-amino acid supplements (L-AA supplements). They were originally developed using human breast milk as the reference protein. Dietary treatment of PKU is multifaceted, challenging and lifelong2-4. Key dietary behaviours associated with optimal control of blood Phe levels include the avoidance of high protein foods plus evenlydistributed consumption of the L-AA supplements throughout the day3-5. PKU is a chronic condition, and although it is not unusual for adherence to be poor6 particularly in teenagers and adults, it is essential that treatment is lifelong in order to achieve optimal neuropsychological functioning. Common issues with PS adherence in patients of all ages is their palatability, smell, taste, texture and aftertaste2, 7, 8. In PKU, any new dietary option that offers an alternative to L-AA supplements should be considered as it may help to improve adherence and quality of life9, 10. Glycomacropeptide (GMP) is a well-researched protein that offers an alternative approach to PS provision in PKU. GMP is a natural protein that is produced as a by-product of the cheese making process. Unmodified, it has an incomplete amino acid profile; it is not only low in Phe, but it is also low in other important amino acids in PKU such as tyrosine, leucine and tryptophan11-13. Thereby, GMP requires measured and appropriate supplementation of these amino acids (apart from Phe) in order to aid attainment of satisfactory blood Phe levels as well as have potential to correct some large neutral acid (LNAAs) deficiencies in the brain14. GMP combined with these limiting essential amino acids (GMP-AA) and additional micronutrients ensure its suitability as an alternative to L-AA supplements9, 15, 16. Due to its structure, GMP may also have other potential health benefits (see Appendix 1). The vast majority of evidence is from animal studies, however short-term cohort studies and case studies have been reported9, 16, 17. Vitaflo has carefully developed and researched a new GMP-AA (PKU sphere) suitable for PKU. We now have over 2 years’ experience of using this product in children and teenagers with PKU in the UK; we have assessed its acceptability and tolerance plus its effects on plasma amino acid profiles, micronutrient levels and growth when compared with conventional L-AA supplements (See Appendix 2 for further information on the safety of GMP). Vitaflo have developed guidelines on the use and introduction of PKU sphere in children over the age of 6 years and adults. Like any GMP-AA, it does contain some Phe (36 mg/20g protein equivalent), so it is essential that every patient with PKU is assessed individually taking into account their current adherence to PS and diet, Phe tolerance, metabolic control and this residual amount of Phe within PKU sphere. Following the suggested step wise system for introducing PKU sphere will aid its successful introduction without loss of metabolic control. Some patients may be able to fully or partially replace their conventional L-AA supplement with this new PS. Anita MacDonald 3 1.0 1.0 GMP 1.1 What is GMP and how is it produced? 1.2 What is PKU sphere? 1.3 Features of PKU sphere 4 1.1 What is GMP and how is it produced? Glycomacropeptide (GMP) is a 64 amino acid (AA) glycophospho-peptide produced as a by-product during the cheese making process. GMP is formed at the coagulation stage when rennet (a complex of enzymes) is added to the milk, to produce a mixture of curds and whey. An enzyme in rennet specifically hydrolyses kappa (k)-casein (a protein in milk) at the peptide bond between the Phe 105 and methionine 106 amino acid residues. It therefore splits into para-k-casein containing Phe, which remains in the cheese curd, whilst the GMP drains off with all the whey proteins forming the whey fraction11 (see figure 1.). Figure 1. illustrates how GMP is formed and isolated through the cheese making process. The cheese making process Milk + rennet Curds Coagulation stage curds + whey Hydrolyses the peptide bond between Phe 105 + Met 106 Cheese Whey fraction drained and separated Mixture of whey proteins For GMP to be suitable for use in the dietary management of PKU it must be isolated from the whey fraction and further purified. 15-20% GMP 80 - 85% other whey proteins including BLG* & ALA** GMP Isolation + purification process Patented fractionation process+. During this isolation process GMP becomes contaminated with other whey proteins that contain Phe15 Unmodified Isolated GMP The purification process reduces the Phe level, however, all GMP based products on the market will contain some Phe. *BLG = beta-lactoglobulin **ALA = alpha-lactalbumin + The patent for this process is held by the manufacturer. 5 Amino acid profile of isolated, unmodified GMP Isolated, unmodified GMP has an unusual amino acid profile. It contains low levels of Phe and other aromatic amino acids and has two to three times the amount of the LNAAs threonine and isoleucine compared to other proteins12, 15. Unmodified GMP Ile Thr High levels of LNAAs: Pro Ala Threonine Low levels of the Met Lys following amino acids: Thr Isoleucine Glu Valine Gln Ile Ile Pro Asn Glu Histidine Asp Pro Thr Ser Gly Leucine Tryptophan Methionine Ala Phenylalanine Tyrosine Cysteine Arginine Addition of free amino acids Isolated, unmodified GMP must be supplemented with the limiting indispensable amino acids (apart from Phe) to ensure it is a viable alternative to L-AA supplements in PKU. GMP-AA GMP supplemented with the limiting essential amino acids provides a low-Phe ‘protein*’ for individuals with PKU. The inclusion of micronutrients and DHA in GMP-AA provides a more nutritionally comprehensive product. Ile Thr Pro Ala Lys Met Tyr His Thr Gly Glu Ile Ile Pro Gln Asn Glu Tyr Pro Thr Trp Ser Gly Ala Leu Arg Asp + Trp Leu Met Arg Tyr Trp Leu Tyr + Micronutrients & DHA His Trp Gly Leu GMP Met Free Amino Acids All commercial GMP-AA contain Phe and therefore partial or full replacement of the L-AA supplements will depend on an individual’s blood Phe control. * See Appendix 3 for more information on why GMP is classed as a whole protein 6 1.2 What is PKU sphere? PKU sphere is a blend of isolated unmodified GMP and free amino acids with added micronutrients and DHA. Isolated unmodified GMP AA r c opep a m o t c i y Low in Phe. Naturally high in the LNAAs threonine, isoleucine and valine. Low in a number of essential amino acids. G l 7 mb Added amino acids to complement GMP. e cin u Le Ensures overall good quality protein* for growth, repair and development. an toph p y r T DHA Vitamins and minerals Prevents essential amino acid deficiencies which would be rate limiting for protein synthesis. Histidine Met hio Ar gi Achieves an overall balanced amino acid profile to optimise blood Phe control. nin e ni ne * When coupled with tolerated Phe allowance. e in yc Gl Sy Ty ro si ne e d Palatable source of natural protein. iotic relatio n s p i h 8 1.3 Features of PKU sphere Optimal nutritional profile Low volume Gl High volumes of protein substitute can be difficult to manage especially in addition to maintaining a healthy food intake. Sy mb e in uc Le Tryp DHA Vitamins and minerals toph an Histidine Met hio Ar gi nin e ni ne e in yc Gl PKU sphere has been designed to deliver a set protein equivalent in a low volume to help aid adherence. Ty ro si ne acropep om ti yc de Amino acid profile - PKU sphere is formulated using the latest nutritional science to ensure the combination of the added LNAAs and GMP are in balance to optimise blood Phe control. iotic relatio n s h The added LNAAs in PKU sphere are key and may compete with Phe both at the blood brain barrier and in the gut. Contains DHA Comprehensive micronutrient profile ip Low volume of PKU sphere allows it to fit easily into a ‘3-a-day’ protein substitute approach. Low in energy PKU sphere has been designed to be low in calories and sugar. PKU sphere contains 120 calories per 20g PE and is similar in energy content to L-AA supplements such as PKU express, PKU cooler and PKU air. Volume per sachet PKU sphere20 x 3/day - 60g PE PKU sphere 500 400 Obesity is a global issue. The calorie content and overall nutritional intake should be monitored closely in PKU with encouragement and advice on how to maintain a healthy weight, an important aspect of dietary care, particularly in teenage and adult patients. It is expected that most of the energy requirements will be met by low Phe food. ml 300 200 100 140ml 140ml 140ml Breakfast Lunch Dinner PKU cooler20 = 420ml per day 0 1 sachet PKU sphere20 + 120ml water = 140ml Palatable Convenient Interchangeable PKU sphere offers an alternative tasting product to L-AA supplements. PKU sphere is available in 2 different flavours: Vanilla and Red berry. Due to its palatability, PKU sphere could improve adherence in a patient group where it may waver. PKU sphere has been developed in line with the micronutrient profile of other PKU products in Vitaflo’s portfolio. For example, 1 sachet of PKU sphere, which contains 20g PE, is equivalent to one sachet of PKU express20 or 1 pouch of either PKU cooler20 or PKU air20. PKU sphere is presented in a convenient pre-measured sachet which can be made up accurately, quickly and easily. Providing blood Phe control is maintained, PKU sphere is interchangeable with an equivalent amount of PE from these L-AA supplements. 9 10 11 2.0 Application of PKU sphere 2.1 Who is PKU sphere for? 2.2 Considerations for using PKU sphere 2.3 How to introduce PKU sphere 2.0 A. For an individual with good metabolic control B. For an individual on a relaxed or non-adherent diet 2.4 Practical points for introducing PKU sphere 12 2.1 Who is PKU sphere for? PKU sphere: • Is for children aged 6 years + and adults with PKU. • Offers an alternative to L-AA supplements for individuals experiencing taste fatigue or struggling with adherence. • May be appealing to those who are interested in the potential health benefits of GMP-AA. • Offers a new palatable option to those who are ‘off diet’ and would like to go back on diet. Teenagers and adults There may be particular interest in using PKU sphere in teenage and adult patients. PKU is a life long condition and it is not unusual for adherence to be poor in such conditions6. A high percentage of blood Phe levels are above target range18, particularly in teenagers and adults, indicating inadequate adherence. Common issues with adherence to protein substitutes, found in patients of all ages, are the palatability, smell, taste, aftertaste and texture of these protein substitutes2, 7, 8. Also often through teenage years, with growing independence, changes at school, peer pressure, condition resentment, adherence with diet and protein substitutes may deteriorate. Published studies reveal patients may prefer GMP-AA, are able to take them frequently spread through the day and in many cases do not want to switch back to L-AA supplements9, 17, 18. All individuals who want to try PKU sphere need to be assessed on an individual basis. Progressing with PKU sphere will depend on metabolic control, adherence to the low protein diet and the clinical judgement of the managing health care professional. Section 2.3 gives an example of (a) how to introduce PKU sphere to an individual with good metabolic control and (b) an individual on a relaxed or non-adherent diet. 13 2.2 Considerations for the use of PKU sphere Managing Phe intake and blood levels The potential impact the extra Phe from PKU sphere will have on blood Phe levels will likely be less in an individual with a higher natural protein/exchange tolerance. If a child/adult is taking 60g of protein equivalent from PKU sphere (108mg Phe) the percentage extra they will receive will depend on their natural protein/exchange tolerance. Natural protein tolerance / day Extra phe from PKU sphere 4g 50% 10g 20% 20g 10% In addition, the target Phe levels varies per population group, as teenagers and adults have a higher maximum target Phe level than children below the age of 124. There are certain individuals where the introduction of a GMP-AA requires additional consideration. Careful monitoring is required and some may only tolerate partial replacement of their L-AA supplement with a GMP-AA, or reduction of natural protein/exchanges could be considered. A reduction in the amount of natural protein intake can reduce variety, quality and adherence of the diet. A recent publication reported that although individuals were advised to reduce the Phe in the diet to compensate for the Phe in the GMP-based products they did not do so17. Introducing PKU sphere gradually, in a systematic way, allows monitoring of metabolic control and discussion with patient/caregiver at each step. A decision can be made as to continue to increase PKU sphere, remain on a combination of PKU sphere and L-AA supplements or consider reducing natural protein/exchanges depending on blood Phe control, individual preference and circumstance. Considerations Pregnancy Excellent blood Phe control prenatally and during pregnancy is crucial to minimise any risk of birth defects especially microcephaly and congenital heart disease19. It is common for natural protein/exchange tolerance to be extremely low prenatally and particularly in the first trimester of pregnancy. There are no published data of GMP-AA use in pregnancy. A few cases have been reported in the USA, however all 4 cases were taking sapropterin with higher natural protein/exchange tolerance20. For those individuals struggling to adhere to L-AA supplements during pregnancy, PKU sphere may be an alternative choice given under careful supervision. If PKU sphere is introduced the 36mg Phe per 20g PE should be accounted for and introduction carried out cautiously. It should be noted, that the use of GMP-AA may not be appropriate in some cases of maternal PKU. Young children The micronutrient profile for PKU sphere is suitable from 3 years of age however as yet there is no published evidence of use in young children under the age of 6 years. Research is ongoing in children from the age of 6 years, with preliminary results suggestive of the need for a gradual systematic introduction of PKU sphere for those with good metabolic control (See Section 2.3). Long term data is required to enable evidence based guidelines to be written for the use of GMP-AA in the younger population under the age of 6 years. 14 2.3 How to introduce PKU sphere A. For an individual with good metabolic control Maintaining or improving metabolic control is of the upmost importance. PKU sphere contains 36mg Phe / 20g PE; this should be taken into consideration when introducing and increasing PKU sphere. The following is an example demonstrating how to introduce PKU sphere. PKU sphere should be increased and titrated with the L-AA supplement gradually with blood Phe levels monitored regularly. PKU sphere should be carefully introduced in a systematic way. This approach will help build the confidence of the patient/caregiver and health care professional regarding the Phe content of PKU sphere and metabolic control. Some individuals may only partially transition, ultimately taking a combination of PKU sphere and L-AA supplement. Others will transition fully to PKU Sphere. This will depend on their blood Phe control, Phe tolerance and individual preference. Assuming a daily intake of 60g PE from PS, taken as 3 x 20g PE throughout the day. Key: L-AA Start 20g PE 20g PE Stage 1 20g PE 20g PE Stage 2 20g PE 20g PE 20g PE sphere L-AA L-AA L-AA L-AA Taking 3 x L-AA supplements with good blood Phe control L-AA Replace 1 dose of L-AA supplement with 1 sachet of PKU sphere Discuss PKU sphere as an alternative PS and the pro’s and con’s of GMP. Consider starting transition to PKU sphere. Advise on keeping the natural protein / exchanges intake the same throughout introduction of PKU sphere. Liquid or powdered L-AA supplement sphere Stage 3 20g PE 20g PE 20g PE 20g PE 20g PE sphere sphere sphere sphere sphere L-AA Replace another dose of L-AA supplement with 1 sachet of PKU sphere Monitor fasting blood Phe levels weekly/ fortnightly Monitor fasting blood Phe levels weekly/ fortnightly If blood Phe control maintained over 3 consecutive tests - Progress to stage 2. If blood Phe control maintained over 3 consecutive tests - Progress to stage 3. NB: 1 sachet of PKU sphere is unlikely to have any impact on blood Phe levels. Encourage adherence with L-AA supplement during this transition stage. Continue to monitor fasting blood Phe levels as per local/ national policy. Replace last dose of L-AA supplement with 1 sachet of PKU sphere If blood Phe control maintained over 3 consecutive tests continue on PKU sphere. If blood Phe level is high Check all other reasons or causes for high levels. NOTE: Take into consideration any significant calorie difference between current L-AA supplement and PKU sphere; advise on nutritional intake accordingly. If no other cause suspected, consider reducing PKU sphere by 1 sachet and replace with L-AA supplement. Monitor blood Phe levels and once there are 3 consecutive results within target treatment range increase again by 1 sachet and continue transition. If blood Phe levels have increased and no other cause detected - some indiviuals with a higher Phe/ natural protein tolerance may prefer to reduce natural protein in the diet rather than reduce PKU sphere. 15 GMP-AA = 36mg Phe 16 2.3 How to introduce PKU sphere B. For an individual on a relaxed or non-adherent diet Those adults on a more relaxed diet or individuals who are struggling to take their recommended amount of L-AA supplements may find a GMP-AA easier and more manageable to take. Discuss PKU sphere as an alternative PS, the pro’s and con’s and potential health benefits of GMP-AA . PKU sphere may help individuals to return to diet and/or regain control of blood Phe levels. Consider introducing PKU Sphere taking into account the below points. The amount of Phe in PKU sphere is unlikely to be as much of a concern in this group. The introduction and increase of PKU sphere could therefore be much quicker, or the full required amount started at once should the individual desire. How PKU sphere is introduced will depend on the individual’s ability to cope, tolerance of the product and motivation. However, this may be unrealistic for some and therefore aiming for 1 or 2 PKU sphere sachets per day may be more manageable which would still be beneficial. A gradual systematic introduction could aid adherence. Consider the amount of protein and energy being consumed from foods in addition to that from PKU sphere. Advise accordingly where possible to aim for recommended/target amounts. Ideally the amount of PKU sphere, coupled with the natural protein from food, would meet protein requirements. In those individuals previously nonadherent who start taking PKU sphere, blood phe levels may significantly improve. Advising to start off with 3 sachets per day (if required) of PKU sphere could be overwhelming for those already finding the diet difficult. NOTE: Continue to monitor fasting blood Phe levels as per local policy. 17 2.4 Practical points and troubleshooting How PKU sphere is introduced into the dietary management of PKU will very much depend on the individual. Outlined below are some practical reminders of what to take into consideration and how to encourage an easier transition. olic l, metab dividua in e c th n ing o a realisti Depend e, agree c n a r le to re to and Phe KU sphe control unt of P o m a e tute oal for th in substi target g tal prote to f o % e.g. 50 be taken 0%. ed or 10 d but a prescrib is agree t n u o m lower a d or vice e that a achieve y ll It may b a tu n eve mount is higher a versa. Emphasise the im portance of continuing to take the usual protein substitute whilst building up the amount of PKU sphere taken. When first build ing up PKU sphere ch oose a time in the day which is more convenient to prepare and take PKU sphere. PKU sphere has a diffe rent taste to L-AA supp lements. It may take a week or tw o to accust om to the n ew taste of PK U sphere. Many indiv iduals onc e establish ed prefer their GMP-AA a nd find it easier to ta ke and spre ad through the day. Explain that droppin g off any L-AA supplement can affect blood Phe control and co uld also delay progression with PK U sphere. Regular contact with regular blood Phe testing is important not only to assess tolerance but to enhance motivation and Those taking a liquid L-AA supplement may feel a switch back to a powdered product more inconvenient, however the pre measured sachet and provided sports beaker help to ‘normalise’ the product and make it quick and easy to prepare. 18 adherence. Trouble shooting High Phe levels Possible cause Action Fever/infection/trauma • Increase energy intake • Ensure intake of PS • Identify and treat source of infections, as clinically indicated Excess natural protein intake • Check PKU sphere has not been increased of the patient’s own accord • Check adherence (at home, school, work, out socialising) • Check understanding/calculation of exchanges/Phe allowance, dietary adherence and hidden sources of natural protein • Check any special products used are low protein and not gluten free by mistake Inadequate intake of protein substitutes • Check adherence (at home, school, work, out socialising) • Check intake of usual PS has not dropped off whilst introducing PKU sphere • Timing of PS intake (should be spread evenly throughout the day) • Check adequate home supply of PS • When necessary recalculate PS requirements and adjust dosage appropriately Incorrect protein substitute taken • Check which PS is being taken. Occasionally the wrong PS may be prescribed or delivered Hormonal fluctuations • Example menstruation No obvious reason or explanation • Reduce PKU sphere by 1 sachet and replace the equivalent amount of protein with usual PS • Consider decreasing natural protein intake from foods by approximately 0.5 – 1g per day. Monitor blood Phe levels carefully Adapted from Ref 21. Advice for illness It is still important to continue to take PKU sphere during illness to assist the stabilisation of blood Phe levels. However it may be necessary to recommend taking the same daily dose but in smaller amounts more frequently through the day. Parents/patients should be given written advice on how to manage illness. 19 3.0 Example Case study 3.1 Case study 3.0 20 3.1 Case study Changing from L-AA supplement to PKU sphere. Patient: 8 year old girl Weight: 24 kg (25th percentile) Height: 125 cm (25th percentile) PE from L-AA supplement: 60g/day (3 x 20gPE L-AA supplement) Natural protein tolerance: 4g/day Total protein intake: 2.7g/kg/day Target phe range: 120-360μmol/L Background An 8-year-old girl taking conventional L-AA supplements three times a day expressed an interest in taking a new GMP-AA product after tasting it in the PKU clinic. The median blood Phe concentration for her previous 12 months was 245 µmol/L with 76% of her blood spot Phe levels within the recommended target range for age. This was considered good control. Her growth, both weight and height were on the 25th centile, with an appropriate body mass index. She ate a limited variety of foods (low protein bread, potato products, salad and low protein biscuits only) despite many attempts to try to expand the variety of foods eaten in her diet. She was taking 60g/day protein equivalent from 3 x 20g PE L-AA supplement (2.5g protein/kg) and 4g/day of natural protein (200 mg/day Phe). Introduction of (GMP-AA) PKU sphere20 sachets The guidelines suggested in this publication for the introduction of GMP-AA sachets to replace the L-AA supplement were followed. No adjustment or reduction of Phe exchanges was required. Stage 1 1. One packet of PKU sphere20 replaces one L-AA supplement 2. Continue taking 2 x L-AA supplement 3. Weekly fasting capillary blood spots 4. Growth monitored frequently Table 1 Introduction of one PKU sphere20 (20g PE) in addition to 2 x L-AA supplements (40g PE) Week Phe µmol/L Tyr µmol/L Comments 1 240 40 No difficulties were observed 2 190 50 and the new product was 3 120 40 taken well. Weight stable. 4 280 50 After 4 weeks of introducing one packet of PKU sphere20, blood Phe concentration remained within target reference age. Therefore, PKU sphere20 increased to 2 packets per day with 1 x L-AA supplement. 21 Stage 2 1. Two packets of PKU sphere20 replace 2 x L-AA supplements 2. Continue taking 1 x 20g PE of L-AA supplement 3. Weekly fasting capillary blood spots 4. Growth monitored frequently 5. Review after 4 weeks and change to all PKU sphere20 providing Phe levels are consistently below the target reference range Table 2 Introduction of two PKU sphere20 (40g PE) in addition to 1 x L-AA supplement (20g PE) Week Phe µmol/L Tyr µmol/L Comments 5 260 30 No illness. 6 400 50 Reported taking all 7 120 40 protein substitute. 8 580 50 Weight stable. Comments There appeared to be no obvious reason for the increase in the blood Phe concentration. The patient had no illness and appeared to be adherent with her diet. However, her parents noticed she was reluctant to finish all her L-AA supplement making total PS intake less consistent than usual. A home visit established a few potential causes: a) It was holiday time and the familiar daily routine of taking PS was changed. Each morning she had a ‘lie in’ in bed therefore took the protein substitute later in the mornings. b) Intake of food was less regular and Phe exchanges had not been measured accurately when eating outside the home. c) She had attended a ‘sleep-over’ on two occasions and delayed taking her PS till later in the morning. Plan As it appeared the fluctuating Phe control may have been either due to inadequate PS intake or extra natural protein intake when eating out, it was agreed to repeat stage 2 and review after 4 weeks. Table 3 Continuation of two PKU sphere20 (40g PE) in addition to 1 x L-AA supplement (20g PE) Week Phe µmol/L Tyr µmol/L 9 270 40 Routine established. 10 130 50 Weight stable. 11 190 40 12 260 50 22 Comments Once her usual routine returned and she was back in school, the Phe concentrations returned to the patient’s usual high standards. She was able to change to 3 packets/daily of PKU sphere20 after 4 weeks of following 2 sachets of PKU sphere20 and 1 pouch of L-AA supplement. Stage 3 1. Increase to three packets of PKU sphere20 2. Stop L-AA supplement 3. Weekly fasting capillary blood spots 4. Growth monitored frequently Table 4 Increase to three PKU sphere20 (60g PE) Week Phe µmol/L Tyr µmol/L Comments 13 180 40 No illness. 14 220 50 Reported taking all 15 190 40 protein substitute. 16 240 40 Weight stable. This young girl continued to have regular assessment of blood concentrations and she demonstrated good control of both Phe and tyrosine concentrations (see Table 4.). Her growth continued to follow the 25th percentile for both height and weight and she continued to do well with her GMP-AA; PKU sphere20. Key messages 1. Transitioning to any new protein supplement needs regular monitoring. 2. If Phe control deteriorates it is important to consider changes to daily routine, in addition to other common causes of poor Phe control. 3. A methodical change highlights when difficulties arise, and gives the family confidence when finding the cause of a problem and enabling a solution to be found. Case study by Anne Daly MSc, RD (Senior metabolic dietitian, Birmingham Children’s Hospital, UK). 23 4.0 Guideline references 4.0 24 References 1. Bickel H, Gerrard J, Hickmans EM. The influence of phenylalanine intake on the chemistry and behaviour of a phenylketonuria child. Acta paediatr. 1954;43(1):64-77. 2. MacDonald A, Gokmen-Ozel H, van Rijn M, Burgard P. The reality of dietary compliance in the management of phenylketonuria. J Inherited Metab Dis. 2010;33(6):665-70. 3. Singh RH, Cunningham AC, Mofidi S, Douglas TD, Frazier DM, Hook DG, et al. Updated, web-based nutrition management guideline for PKU: An evidence and consensus based approach. Mol Genet Metab.2016; 118(2): 72-83. 4. Van Spronsen FJ, Van Wegberg AMJ, Ahring K, Belanger-Quintana A, Blau N, Bosch A, et al. European guidelines on diagnosis and treatment of PKU. J Inherited Metab Dis. 2016;39 (Suppl 1):S101. 5. MacDonald A, Chakrapani A, Hendriksz C, Daly A, Davies P, Asplin D, et al. Protein substitute dosage in PKU: how much do young patients need? Arch Dis Child. 2006;91(7):588-93. 6. Burkhart PV, Sabaté E. Adherence to long-term therapies: evidence for action. J Nurs Scholarsh. 2003;35(3):207. 7. MacDonald A, Daly A, Davies P, Asplin D, Hall SK, Rylance G, et al. Protein substitutes for PKU what’s new? J Inherited Metab Dis. 2004;27(3):363-71. 8. Hoeks MP, den Heijer M, Janssen MC. Adult issues in phenylketonuria. Neth J Med. 2009;67(1):2-7. 9. Ney DM, Gleason ST, van Calcar SC, MacLeod EL, Nelson KL, Etzel MR, et al. Nutritional management of PKU with glycomacropeptide from cheese whey. J Inherited Metab Dis.2009;32(1):32-9. 10 van Calcar SC, Ney DM. Food products made with glycomacropeptide, a low-phenylalanine whey protein, provide a new alternative to amino acid-based medical foods for nutrition management of phenylketonuria. J Acad Nutr Diet. 2012; 112(8): 1201-10. 11. Doultani S, Turhan K, Etzel M. Whey Protein Isolate and Glyco‐macropeptide recovery from whey using ion exchange chromatography. J Food Sci. 2003;68(4):1389-95. 12. Etzel MR. Manufacture and use of dairy protein fractions. J Nutr. 2004;134(4):996s-1002s. 13. Neelima S, Sharma R, Rajput Y, Mann B. Chemical and functional properties of glycomacropeptide (GMP) and its role in the detection of cheese whey adulteration in milk: a review. Dairy Sci & Technol. 2013; 93(1): 21-43. 14. van Vliet D, Bruinenberg VM, Mazzola PN, van Faassen MH, de Blaauw P, Kema IP, et al. Large Neutral Amino Acid supplementation exerts its effect through three synergistic mechanisms: Proof of principle in phenylketonuria mice. PloS one. 2015;10(12):e0143833. 15. LaClair CE, Ney DM, MacLeod EL, Etzel MR. Purification and use of glycomacropeptide for nutritional management of phenylketonuria. J Food Sci.2009;74(4):E199-E206. 16. van Calcar SC, MacLeod EL, Gleason ST, Etzel MR, Clayton MK, Wolff JA, et al. Improved nutritional management of phenylketonuria by using a diet containing glycomacropeptide compared with amino acids. Am J Clin Nutr. 2009;89(4):1068-77. 17. Ney DM, Stroup BM, Clayton MK, Murali SG, Rice GM, Rohr F, et al. Glycomacropeptide for nutritional management of phenylketonuria: a randomized, controlled, crossover trial. Am J Clin Nutr. 2016;104(2):334-45. 18. Walter JH, White FJ, Hall SK, MacDonald A, Rylance G, Boneh A, et al. How practical are recommendations for dietary control in phenylketonuria? Lancet. 2002;360(9326):55-7. 19. Matalon KM, Acosta PB, Azen C. Role of nutrition in pregnancy with phenylketonuria and birth defects. Pediatrics. 2003;112(6 Pt 2):1534-6. 20. Bausell H, Aspan A, Arduini K, Paras A, Burton BK. Review of maternal phenylketonuria treatment methods including sapropterin and glycomacropeptide. 2016. Poster presented at National Phenylketonuria Alliance (NPKUA) conference, Indianapolis, USA. 21. MacDonald A, White F. Amino Acid Disorders. In: Shaw V (ed.) Clinical Paediatric Dietetics, 4th edition, Oxford, John Wiley & Sons Ltd. 2015. p. 391-456. 25 5.0 Appendices 5.1 Appendix 1 – Summary of references related to GMP potential benefits 5.2 Appendix 2 – Safety of GMP 5.3 Appendix 3 – Why is GMP classed as a whole protein? 5.0 26 5.1 Appendix 1 Summary of references related to GMP potential benefits GMP scientific evidence summary GMP has a unique chemical structure. It is highly polar with a strong negative charge and is a rich source of sialic acid (also known as N-acetylneuraminic acid (NANA)), a carbohydrate moiety attached to the threonine sites of the protein. Many of the biological properties of GMP are attributed to this unique structure. Since the 1970’s GMP has been of interest for its potential benefits in many population groups and conditions. Potential GMP benefits directly related to PKU The vast majority of evidence is from animal studies, however Reduction of phe in the brain Ney et al 20081, Pietz et al 19992, Sanjuro et al 20033, van Spronson et al 20104 Increased efficacy of protein utilisation / improved nitrogen retention Ney et al 20145, van Calcar et al 20096 Improved long term bone health Solverson et al 20127 Better palatability Lim et al 20078, van Calcar et al 20096, Ney et al 20169 Oral hygiene White et al 201010, Aimutis 200411, Brody 200012 27 Specific investigations into GMP for use in the management of PKU first arose because of the natural low levels of Phe; further potential benefits of GMP have been proposed and reported, mainly in relation to bone and gut health, but also its impact on overall nitrogen metabolism. The following is a summary of evidence listing the potential benefits of GMP. References marked in bold font denote research directly linked to GMP whereas references marked in non-bold font denote research that, whilst not directly linked to GMP, are of relevance to the highlighted issue. Other potential GMP related benefits r short-term cohort studies and case studies have been reported. Prebiotic effect Brody 200012, Chen et al 201213, Sawin et al 201514 Anti-inflammatory effect Jia et al 201115, Sprong et al 201016, Requena et al 200817, Wang et al 201218, Daddaoua et al 200519, Hvas et al 201620, Solverson et al 201221 Binds to enterotoxins & inhibits bacterial and viral adhesion Kawasaki et al 199222, Nakajima et al 200523, Hermes et al 201324, Dziuba et al 199625 Improved satiety Burton-Freeman et al 200826, Macleod et al 201027 Role in weight management Xu et al 201328, Royle et al 200829 Improvement of zinc absorption Kelleher et al 200330 Stimulation of brain development Wang et al 200731 28 References 1. Ney DM, Hull AK, van Calcar SC, Liu X, Etzel MR. Dietary glycomacropeptide supports growth and reduces the concentrations of phenylalanine in plasma and brain in a murine model of phenylketonuria. J Nutr. 2008;138(2):316-22. 2. Pietz J, Kreis R, Rupp A, Mayatepek E, Boesch C, Bremer HJ. Large neutral amino acids block phenylalanine transport into brain tissue in patients with phenylketonuria. J Clin Invest. 1999;103(8):1169-78. 3. Sanjurjo P, Aldamiz L, Georgi G, Jelinek J, Ruiz J, Boehm G. Dietary threonine reduces plasma phenylalanine levels in patients with hyperphenylalaninemia. J Pediatr Gastroenterol Nutr 2003;36(1):23-6. 4. van Spronsen FJ, de Groot MJ, Hoeksma M, Reijngoud DJ, van Rijn M. Large neutral amino acids in the treatment of PKU: from theory to practice. J Inherit Metab Dis. 2010;33(6):671-6. 5 Ney DM, Blank RD, Hansen KE. Advances in the nutritional and pharmacological management of phenylketonuria. Curr Opin Clin Nutr Metab Care. 2014;17(1):61-8. 6. van Calcar SC, MacLeod EL, Gleason ST, Etzel MR, Clayton MK, Wolff JA, et al. Improved nutritional management of phenylketonuria by using a diet containing glycomacropeptide compared with amino acids. Am J Clin Nutr. 2009;89(4):1068-77. 7. Solverson P, Murali SG, Litscher SJ, Blank RD, Ney DM. Low bone strength is a manifestation of phenylketonuria in mice and is attenuated by a glycomacropeptide diet. PloS one. 2012;7(9):e45165. 8. Lim K, van Calcar SC, Nelson KL, Gleason ST, Ney DM. Acceptable low-phenylalanine foods and beverages can be made with glycomacropeptide from cheese whey for individuals with PKU. Mol Genet Metab. 2007;92(1):176-8. 9. Ney DM, Stroup BM, Clayton MK, Murali SG, Rice GM, Rohr F, et al. Glycomacropeptide for nutritional management of phenylketonuria: a randomized, controlled, crossover trial. Am J Clin Nutr. 2016. Aug;104(2):334-45. 10. White A, Gracia L, Barbour M. Inhibition of dental erosion by casein and casein-derived proteins. Caries res. 2010;45(1):13-20. 11. Aimutis WR. Bioactive properties of milk proteins with particular focus on anticariogenesis. J Nutr. 2004;134(4):989S-95S. 12. Brody EP. Biological activities of bovine glycomacropeptide. Brit J Nutr. 2000;84 Suppl 1:S39-46. 13. Chen Q, Cao J, Jia Y, Liu X, Yan Y, Pang G. Modulation of mice fecal microbiota by administration of casein glycomacropeptide. Microbiol Res. 2012;3(1):3. 14. 26. Sawin E, Aktas B, DeWolfe T, Stroup B, Murali S, Steele J, et al. Glycomacropeptide Shows Prebiotic and Immune Modulating Properties in Phenylketonuria and Wild Type Mice. FASEB J. 2015;29(1 Supplement). 15. Jia Y-c, Chen Q-s, Feng Y-n, Xu Y-j, Li Y. Effect of Bovine Casein Glycomacropeptide on MUC2 Expression in Mice with Ulcerative Colitis. Food Science . 2011;15:050. 16. Sprong R, Schonewille A, Van der Meer R. Dietary cheese whey protein protects rats against mild dextran sulfate sodium–induced colitis: Role of mucin and microbiota. J Dairy Sci. 2010;93(4):1364-71. 17. Requena P, Daddaoua A, Martínez‐Plata E, González M, Zarzuelo A, Suárez M, et al. Bovine glycomacropeptide ameliorates experimental rat ileitis by mechanisms involving downregulation of interleukin 17. Brit J Pharmacol. 2008;154(4):825-32. 18. Wang H, Chen Q-s. Milk-derived casein glycomacropeptide inhibits ulcerative colitis in mice through apoptosis resistance. Food Science . 2012;33:230-4. 29 19. Daddaoua A, Puerta V, Zarzuelo A, Suárez MD, de Medina FS, Martínez-Augustin O. Bovine glycomacropeptide is anti-inflammatory in rats with hapten-induced colitis. J Nutr. 2005;135(5):116470. 20.Hvas CL, Dige A, Bendix M, Wernlund PG, Christensen LA, Dahlerup JF, et al. Casein glycomacropeptide for active distal ulcerative colitis: a randomized pilot study. Eur J Clin Invest 2016;46(6):555-63. 21. Solverson P, Murali SG, Brinkman AS, Nelson DW, Clayton MK, Yen CL, et al. Glycomacropeptide, a lowphenylalanine protein isolated from cheese whey, supports growth and attenuates metabolic stress in the murine model of phenylketonuria. Am J Physiol Endocrinol Metab. 2012;302(7):E885-95. 22. Kawasaki Y, Isoda H, Tanimoto M, Dosako S, Idota T, Ahiko K. Inhibition by lactoferrin and kappacasein glycomacropeptide of binding of Cholera toxin to its receptor. Biosci Biotechnol Biochem. 1992;56(2):195-8. 23.Nakajima K, Tamura N, Kobayashi-Hattori K, Yoshida T, Hara-Kudo Y, Ikedo M, et al. Prevention of intestinal infection by glycomacropeptide. Biosci Biotechnol Biochem. 2005;69(12):2294-301. 24.Hermes RG, Molist F, Pérez JF, de Segura AG, Ywazaki M, Davin R, et al. Casein glycomacropeptide in the diet may reduce Escherichia coli attachment to the intestinal mucosa and increase the intestinal lactobacilli of early weaned piglets after an enterotoxigenic E. coli K88 challenge. Brit J Nutr. 2013;109(06):1001-12. 25. Dziuba J, Minkiewicz P. Influence of glycosylation on micelle-stabilizing ability and biological properties of C-terminal fragments of cow’s κ-casein. Int Dairy J. 1996;6(11):1017-44. 26.Burton-Freeman BM. Glycomacropeptide (GMP) is not critical to whey-induced satiety, but may have a unique role in energy intake regulation through cholecystokinin (CCK). Physiol Behav. 2008;93(1– 2):379-87. 27.MacLeod EL, Clayton MK, van Calcar SC, Ney DM. Breakfast with glycomacropeptide compared with amino acids suppresses plasma ghrelin levels in individuals with phenylketonuria. Mol Genet Metab. 2010;100(4):303-8. 28.Xu S-P, Mao X-Y, Cheng X, Chen B. Ameliorating effects of casein glycomacropeptide on obesity induced by high-fat diet in male Sprague-Dawley rats. Food Chem Toxicol. 2013;56:1-7. 29. Royle PJ, McIntosh GH, Clifton PM. Whey protein isolate and glycomacropeptide decrease weight gain and alter body composition in male Wistar rats. Brit J Nutr. 2008;100(1):88-93. 30. Kelleher SL, Chatterton D, Nielsen K, Lönnerdal B. Glycomacropeptide and α-lactalbumin supplementation of infant formula affects growth and nutritional status in infant rhesus monkeys. Am J Clin Nutr. 2003;77(5):1261-8. 31. Wang B, Yu B, Karim M, Hu H, Sun Y, McGreevy P, et al. Dietary sialic acid supplementation improves learning and memory in piglets. Am J Clin Nutr. 2007;85(2):561-9. 30 5.2 Appendix 2 Safety of GMP GMP has an excellent safety record and is already incorporated into foods, including infant formula1. The use of GMP in the dietary management of PKU was first reported in a paper in 20081. The investigators set out to assess if the ingestion of GMP could support the growth of mice with PKU. They also measured both brain and plasma amino acid levels. They found that PKU mice fed a diet of GMP supplemented with essential amino acids (GMP-AA) had a 20% decrease in their cerebellar Phe concentrations compared to mice fed a conventional L-AA supplements. They also observed similar levels of growth when mice were fed a GMP-AA based diet were compared with those fed a L-AA supplement. Another preclinical study investigated the body composition of PKU mice fed a predominately GMP based diet compared to an L-amino acid diet. They found that diet played a significant effect on body composition2 and mice fed a mainly GMP based diet showed a significantly lower percentage of body fat compared to mice fed an amino acid based diet, despite similar lean mass and gain in body weight in the 2 groups. The findings supported their hypothesis that a GMP based diet provides a more physiological source of protein compared to amino acids in mice but that further work in humans was required. The first report of GMP in an adult patient with PKU was a case study published in 20093. The study lasted a total of 15 weeks with the first 3 and last 2 weeks requiring the patient to take his usual amino acid based protein substitute. During the middle 10 weeks GMP based protein substitutes replaced his usual amino acid protein substitute. The patient achieved a 10% reduction in blood Phe levels when taking a GMP-AA compared to a L-AA supplement. The first trial to be conducted in patients with PKU was published in 20094. Although this was a small, short term, study investigating 11 patients over two 4-day periods, it compared patients taking both a GMP-AA and a L-AA supplement. It investigated the safety of GMP, plasma amino acid levels and acceptability. There were no physical concerns detected on examination or expressed by any subjects to indicate GMP-AA had a negative effect of health and at the end of the study 6 of the 7 adult patients expressed a strong preference to continue with the GMP-AA. A second larger scale trial was published by the same centre in 20165, again looking at efficacy, acceptability and safety of using GMP-AA compared with L-AA supplements. This was a two stage, randomised crossover trial including 30 early treated PKU subjects aged 15 – 49 years. The period of treatment on GMP-AA was 3 weeks compared with 3 weeks on L-AA supplements. A 3 week washout period separated the 2 blocks of treatment. The most important finding of the study was that there was again no significant difference in the post prandial plasma Phe levels over time when subjects took GMP-AA compared to a L-AA supplement. In summary over the last 8 years, GMP products have been studied with respect to providing an alternative protein source within the management of PKU. GMP must be supplemented with limiting indispensable amino acids to be an appropriate alternative to some or all of a phenylalanine free L-amino acid protein substitute. It has proved to be safe in preclinical animal models and small scale human trials and case studies. It may have additional health benefits for the PKU individual of which further long term research is required. 31 References 1. Ney DM, Hull AK, van Calcar SC, Liu X, Etzel MR. Dietary glycomacropeptide supports growth and reduces the concentrations of phenylalanine in plasma and brain in a murine model of phenylketonuria. J Nutr. 2008;138(2):316-22. 2. Solverson P, Murali SG, Brinkman AS, Nelson DW, Clayton MK, Yen CL, et al. Glycomacropeptide, a lowphenylalanine protein isolated from cheese whey, supports growth and attenuates metabolic stress in the murine model of phenylketonuria. Am J Physiol Endocinol Metab. 2012;302(7):E885-95. 3. Ney DM, Gleason ST, van Calcar SC, MacLeod EL, Nelson KL, Etzel MR, et al. Nutritional management of PKU with glycomacropeptide from cheese whey. J Inherit Metab Dis. 2009;32(1):32-9. 4. van Calcar SC, MacLeod EL, Gleason ST, Etzel MR, Clayton MK, Wolff JA, et al. Improved nutritional management of phenylketonuria by using a diet containing glycomacropeptide compared with amino acids. Am J Clin Nutr. 2009;89(4):1068-77. 5. Ney DM, Stroup BM, Clayton MK, Murali SG, Rice GM, Rohr F, et al. Glycomacropeptide for nutritional management of phenylketonuria: a randomized, controlled, crossover trial. Am J Clin Nutr. 2016 ;104(2):334-45. 32 5.3 Appendix 3 Why is GMP classed as a whole protein? Protein is a macronutrient which is an essential component of everyday nutritional requirements. It is essential for growth, tissue repair and many biological pathways within the body. A low phenylalanine diet, the principal treatment in PKU, is prescribed to reduce intake of Phe to a safe tolerated level. This together with evenly-distributed consumption of the protein substitute over the day are key dietary components associated with optimal control of blood Phe levels1. Amino acids are the building blocks of protein. There are 20 Amino acids different amino acids, 9 of which cannot be made by the body His Tyr Phe Cys Arg Trp and are therefore essential. When amino acids are not linked Leu Thr together in a chain they are termed ‘free amino acids’. Gln Met Phe is not added to a L-AA supplements for PKU making them Ile Asn Val Pro Glu ‘Phe free’. Lys Gly His Asp Tyr Phe Ser Cys Arg Trp Leu Ala Thr Conventional protein substitutes for PKU are based on free amino acids. Gln Met Ile Asn Val Pro Glu Lys Met Gly Asp Ser Pro Ala Thr Ile Ala Lys Peptides Peptides are short chains of amino acids joined together by Thr peptide bonds. Glu Ile Met His Cys Ile Ala Pro Trp Tyr Phe joined by a peptide bond, up to around 50 amino acids all linked Leu Thr together building a long chain peptide. Lys Arg Thr ThrGln Met Glu Glu Ile Ile Asn Val Pro Pro Lys Protein substitutes were first developed in the 1950’s using Thr IleLys Glu Thr Gly Asp Peptides can be as small as 2 amino acids (building blocks) Ser protein hydrolysates (containing peptides) passed through Thr Ala Ile charcoal to remove Phe and tyrosine. Ile Gln Pro Asn GluGlu Ile Ala Gly Thr Asp Pro Pro Ser Thr Met Lys Met Thr Ile Ile Ala Thr Ile Pro whole protein. Pro Asn Thr Glu Glu Asp Ala Pro Ser It has a unique amino acid profile which is Ala naturally low in Phe. Ile Met Protein Whole proteins are made up of hundreds or thousands of amino acid building blocks attached to each other in long chains. Glu Ile The sequence of the 20 amino acids determines each protein’s Thr Pro Lys Thr Thr Ile Ile Gln Asn Glu Asp Ala Gly of 64 amino acids linked together in a chain. With this number of amino acids it can be classified as a Gln Lys Gly GMP is a ‘macropeptide’ consisting Ala Ser Pro unique 3-dimensional structure and its specific function. In PKU, Phe is provided from whole protein food sources. Pro Ala Met 33 References 1. MacDonald A, Chakrapani A, Hendriksz C, Daly A, Davies P, Asplin D, et al. Protein substitute dosage in PKU: how much do young patients need? Arch Dis Child. 2006;91(7):588-93. 34 A Nestlé Health Science Company Vitaflo International Ltd, Suite1.11, South Harrington Building, 182 Sefton Street, Brunswick Business Park, Liverpool L3 4BQ, UK +44 (0)151 709 9020 www.vitafloweb.com ® Reg. Trademarks of Société des Produits Nestlé S.A. © Société des Produits Nestlé S.A. PKUSPHERE1-1216-V1 January 2017