Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Ebola virus disease wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Orthohantavirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
West Nile fever wikipedia , lookup
Oesophagostomum wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Marburg virus disease wikipedia , lookup
Influenza A virus wikipedia , lookup
Henipavirus wikipedia , lookup
Hepatitis B wikipedia , lookup
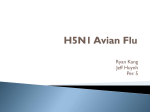
From www.bloodjournal.org by guest on June 18, 2017. For personal use only. Human Immunodeficiency Virus-Type 1 Replication Can Be Increased in Peripheral Blood of Seropositive Patients After Influenza Vaccination By William A. O’Brien, Kathie Grovit-Ferbas, Ali Namazi, Stanislava Ovcak-Derzic, He-Jing Wang, Julie Park, Christine Yeramian, Si-Hua Mao, and Jerome A. Zack Despite considerable evidence that cell activation enhances human immunodeficiency virus-type 1 (HIV-1) replication in vitro, there is very little data on the role of immune activation on in vivo HIV-1 replication. In this study, we examined the effect of influenza vaccinationon HIV-1 replication in the peripheral blood of 20 study subjects, and in 14 control subjects who did not receive influenza vaccination. Blood was obtained from each subject on three occasions during the month before vaccination and again on three occasions during the following month. Over the study period, there was F i l e change in levels of proviral DNA in peripheral blood mononuclear cells (PBMCs). However, peak PBMC viral RNA levels after influenza vaccination were significantly in- creased overthe mean of prevaccinationvalues. This change was not observed to the same extent in unvaccinated controls. Therefore, this is the first report showing that HIV-1 replication can increase in temporal association with influenza vaccination. Our results suggest that continued immunologic (antigenic) stimulation may result in increased virus load in vivo. To address the appropriateness of influenza vaccination in HIV-infected patients, expanded studies will be required to examine specific and generalized immune responses to vaccination, and differences in patient response based on disease stage. 0 1995 by The American Societyof Hematology. H UMAN IMMUNODEFICIENCY virus-type 1 (HIVviral load, as reflected by viral DNA and RNA levels and 1) infection leads to a progressive depletion of CD4+ by infectious HIV-1 Nonetheless, factors responsilymphocytes and acquired immunodeficiency syndrome ble for the regulation of virus expression in vivo remain (AIDS) in a majority of HIV-infected individuals.’ Although poorly defined. the median time course from acute infection to AIDS is One potential mechanism of virus induction is immune greater than 10 years: the duration of the clinically latent activation. Activation of CD4+ lymphocytes and mononustate is highly variable, and factors that govern clinical laclear phagocytes in vitro appears to be important for productency have not been elucidated. After acute infection, there tion of HIV-1. Cellular transcription factors induced after is a viremic phase with widespread distribution of v i r u ~ . ~ . ~activation of T cells can increase HIV-1 Viremia typically decreases within 2 to 3 weeks, at least in Other studies using cultured primary T cells have shown part because of sequestration of virus in lymph as that, although HIV-1 can bind and enter both quiescent and well as development of specific anti-HIV-1 immunity.’ Alactivated cells, activation is required for completion of rethough the acute HIV-1 syndrome maybe followed by a verse transcription, integration, andor subsequent progeny prolonged period of clinical latency, there does not appear virus f ~ r m a t i o n . ~Similarly, ~-*~ activation of mononuclear to be virologic latency. High levels of circulating virus partiphagocytes, by adherence to plastic or by cytokine treatment, cles can still be shown in the plasma of infected asymptomcan dramatically enhance virus production in vitro.28,2y atic individuals by quantitative HIV-1 RNA polymerase Therefore, we hypothesize that immunologic activation may chain reaction (PCR) inplasma: as well as in lymphoid also increase HIV-1 replication in vivo. tissue.6. Recently, the dynamic interaction between HIV- 1 To address this issue, we have examined the effect of replication and CD4+ lymphocyte destruction was shown antigenic stimulation by influenza vaccination on HIV-1 repin HIV-infected individuals after administration of potent lication in the peripheral blood of HIV-infected patients. Because cell-mediated immunity is important for containing antiretroviral drugs.”.” Moreover, clinical progression and influenza virus infection, HIV-infected patients are thought CD4’ lymphocyte depletion are associated with increases in to be at risk for prolonged andmore severe disease, and annual influenza vaccination is specifically rec~mmended.~’ In this report, we show increases in HIV-1 RNA levels in From the Veterans Affairs Medical Center, Department of Medicine, Division of Infectious Diseases, West Los Angeles, CA, and peripheral blood mononuclear cells (PBMCs) temporally asthe Department of Medicine, Divisionof Hematology-Oncology, the sociated with influenza vaccination. ’ University of California at Los Angeles. Submitted November 15, 1994; accepted March 14, 1995. Supported by Department of Veterans Affairs medical research funds, National Institutes of Health GrantNo. AI 33259, UCLA Institutional Training Grant No. PHS/5 T32 AI07388, and grants from the American Foundation for AIDS Research and Genentech, Inc,SouthSan Francisco, CA. Address reprint requests to William A. O’Brien, MD, Divisionof Infectious Disease, 691/11 IF, 11301 Wilshire Blvd, Los Angeles, CA 90073. The publication costsof this article were defrayedin part by page chargepayment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8603-00I6$3.00/0 1082 MATERIALSANDMETHODS Patients. Study subjects (n = 34) were HIV-l seropositive and at an intermediate stage of HIV disease at entry to the study with no AIDS-defining illnesses. This study was approved by the Veterans Affairs Medical Center West Los Angeles Internal Review Board for human subjects, and informed consent was obtained for all participants. Subjects were to have CD4+ lymphocyte counts of 200 to 500/mm3,although those having 100 to 200/mm3 or 500 to 550/mm3 at study entry were not excluded if willing to participate. Two patients (01 and 03) were studied in successive years, and are counted twice. Study subjects were self-assigned tothe vaccinated (n = 20) or nonvaccinated control group (n = 14), because influenza vaccination was, and still is, recommended for all HIV-infected individuals. Patients were excluded if there was clinical or laboratory Blood, VOI 86, N O 3 (August l), 1995: Pp 1082-1089 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1083 INFLUENZAVACCINE-INDUCED HIV-1 REPLICATION evidence of acute viral hepatitis, active herpes simplex virus infection, pneumonia, or other acute respiratory infection, psychosis, or transfusion within the last 2 months. Patients receiving immunization did not have an allergy to eggs, because vaccine antigens were derived from influenza virus preparations grown in eggs. At each visit, patients were specifically questioned about the presence of fever, cough, rash, cutaneous or respiratory infection, and diarrhea. Blood collection and processing. Blood was collected on three occasions during the month before influenza vaccination, with the third sample obtained on the day of vaccination. These baseline samples were obtained at 7-to 14-day intervals, and spanned a period of at least 3 weeks. Additional blood samples were obtained during the first week, the second week, and at 4 to 6 weeks after vaccination. PBMCs were purified by Ficoll/Hypaque (Pharmacia, Uppsala, Sweden) gradient centrifugation within 3 hours after collection. For PCR analysis, lo7 cells were lysed in buffer containing 4.7 m o m urea3' and stored at -70°C. Nucleic acids were purified simultaneously from all samples for each patient by phenolkhloroform extraction and ethanol precipitation. The remainder of PBMCs were cryopreserved in RPM1 1640 medium, 20% fetal calf serum, and 10% dimethylsulfoxide in the vapor phase of a liquid nitrogen freezer. PBMCs from HIV-negative donors used for plasma infections titer analysis were obtained from Red Cross leukopaks (Los Angeles, CA). Quantitative PCR analysis. Samples from each patient were analyzed in batch on the same test run to avoid interassay variation. Quantitative PCR for human P-globin sequence^"^^^^^^ was performed on samples from each patient to standardize for cell equivalents as a control both for nucleic acid recovery and for amplification efficiency. Sample volumes were then adjusted for subsequent HIV analysis. HIV-specific DNA in each sample was measured by quantitative PCR using "P-end-labeled long terminal repeat (LTR) R/U5 primers," followed by amplification for 30 cycles at 94°C for 1 minute and 65°Cfor 2 minutes. HIV-1 copy number was determined by comparison with linearized, cloned HIV-1 DNA standards amplified in parallel as previously described.%,33 To measure HIV- 1 RNA levels in PBMCs, total nucleic acids for each sample from an equivalent number of cells (standardized by cell number, and subsequently by @-globin DNA content) were treated with RNase-free DNase I at 37°C for 40 minutes to digest the DNA. Purified RNA from a 3 X 105 cells was amplified using rTth polymerase (Perkin ElmerCetus, Nonvalk, CT) with reverse transcription in the presence of MnCI, and 12 pmol of the antisense gag primer LA9% at 70°C for 15 minutes, followed by 35 cycles of amplification using 6 pmol of the y3'P-labeled sense primer LA8" and 6 pmol cold LA8 added for a total amount of 12 pm01 per reaction, under the conditions described above. The absence of HIV-l DNA wasshown by omitting the reverse transcription step in a duplicate sample, and analyzing in parallel. Cell equivalence for RNA analysis was shown by subjecting selected samples to quantitative RT-PCR using P-actin primers. Quantitation was achieved by comparison with amplicons generated from serial dilutions of RNA purified from PBMCs infected in vitro by HIV-lJR.Cs$4and subjected to reverse transcription and PCR in parallel. The signal intensity of the amplified product was measured from the autoradiograph by densitometry using an optical imaging system (Ambis, San Diego, CA). Standard curves were generated from the values obtained for 0-globin, and HIV-l DNA and RNA standards, which were used to derive values for experimental samples after interpolation of the standard curve. Statistics. Nonparametric analyses were usedto assess change in viral RNA levels. The mean of the three preimmunization RNA measurements for each patient wasdefined as the baseline RNA level. Relative change in RNA level was defined as the difference between the peak RNA value postimmunization and the mean baseline value, divided by the mean baseline value. The sign rank test was used to evaluate the changes within each study group, whereas the Wilcoxon rank sum test was used to compare the changes between the two study groups. RESULTS The mean C M ' lymphocyte count for all study subjects was 301 ? 112/mm3;range, 55 to 547/mm3.Only one subject had a CD4' lymphocyte count less than 120/mm3;this was patient Olb on his second evaluation. The mean CD4+ lymphocyte count at entry was not significantly different for control and vaccinated patients (337 2 112 and 2772 107, respectively, P = .13). The racial composition of the two study groups was similar; 40% of the study subjects were black, 7% were Hispanic, and the remainder were white. All of the study patients were believed to have acquired HIV-1 infection sexually, none admitted to recent intravenous drug use. All but two of the study patients (04 and 34) were receiving zidovudine therapy. Patient histories and examinations at l- to 2-week intervals during the 2-month study period did not show any side effects from vaccination, nor were there any symptoms of acute infections in the study population. Therefore, we do not believe overt infections with bacteria or with heterologous viruses were important confounders during the course of observation. This analysis is critical, because infection may be another potential source of stimulation, and hence, viral induction. In addition, none of the study patients reported blood transfusions or symptoms of allergy or hay fever during the study period. PBMCs were then analyzed for HIV-1 DNA and RNA levels by quantitative PCR at each time point for each patient. To account for differences in nucleic acid extraction efficiency, each sample for each patient set was standardized for cell equivalence by using quantitative PCR for &globin gene sequences. HIV-1 DNA PCR results for five representative patients are shown in Fig 1. With one exception (patient 04, data not shown), there was no detectable increase in HIV-1 DNA levels on a per-cell basis during the 2-month study period in either the vaccinated or nonvaccinated control group. Of importance, patient 0 4 , a vaccinated subject, had not been receiving zidovudine therapy. Antiretroviral therapy with zidovudine wouldbe expected to inhibit formation ofnew viral DNA. Patient 26, a nonvaccinated control, exhibited a fall in PBMC HIV-1 DNA levels during the latter half of the 2-month study period, which was roughly matched by a fall in PBMC HIV-1 RNA levels (Fig 2). This higher HIV1 replication level at the earlier time points may reflect an activation event that immediately preceded the study period. HIV-1 RNA was detected in every patient and in most (over 80%) of the individual PBMC samples. Representative HIV-1 RT-PCR experiments from the same five patients in Fig 1 are shown in Fig 2. In contrast with what wasobserved for viral DNA, there was a significant relative increase in postvaccination HIV-1 RNA levels in PBMC from the 20 patients receiving influenza vaccination (1 1.6- t 5.0-fold increase, median 2.7, P < .002). Greater than fourfold increases were seen in 10/20 (50%)of the vaccinated subjects. The peak HIV-1 RNA levels typically occurred at 1 or 2 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. O'BRIEN ET AL 1084 HIV-I Standards (Copy number) i K 300 100 30 10 3 Subject Blood Sampling (Weeks) -4 -2 0 +l +2 +4 B - 22 - 23*- 28- 33- or, 26- e* 0 - weeks postvaccination (in 9/10 patients showing greater than fourfold increase), and returned to baseline at later time points. Thus, in most patients, HIV-I RNA induction was transient. Equivalent increases in peak PBMC RNA levels during the same time frame were not seen in the 14 nonvaccinated controls (2.4- ? 1.6-fold increase; median, 0.0; P = .24), andonly 2/14 control patients (14%) had increases greater than fourfold. These data are summarized in Table 1. As another measure of viralinduction. we measured plasma infectious titer by limiting dilution culture analysis13.14 I n 15 of the 20 vaccinated subjects, and 4 of the 14 ' nonvaccinated controls. In this analysis, sequential fivefold dilutions of patient plasma were added to IO" phytohemagglutinin (PHA)-stimulated peripheral blood lymphocytes (PBL) in duplicate in 24-well plates, and assayed for p24 production at days 7 and 14. A fivefold or greater increase in infectious plasma virus titer was seen in one of four nonvaccinated controls (patient 15), a patient in whom increases in cellular HIV-I RNA were also detected. Plasma HIV-I infectious titer increases of fivefoldor greater were also seen in 6 of the 15 vaccinated subjects. Five of these 6 subjects also had increases in cellular HIV-I RNA, and 1 patient (09) in whom there was a 79-fold increase in cellular HIV-I RNA, also had a greater than 25-fold increase in plasma infectious virus titer. Thus, increases in plasma infectious virus titer were consistent with results seen for cellular RNA expression. The peak RNA PBMC level was plotted against the mean baseline levels for vaccinated and nonvaccinated control patients in Fig 3. Comparison of increases betweenthetwo groups indicated a trend toward significance of the change in vaccinated patients ( P = .089). Although there were highly Fig1. Ouantitative HIV-1 PCR analysisofPBMC DNA. PBMC DNA was purified and equivalent amounts were ampliiied asdescribed in Materials and Methods using LTR-specific primers M667 and AA55 (140-bp product). Patients 22, 23, 28, and 33 were vaccinated (V); patient 26 was a nonvaccinated control (C). B is the reagent controlsample subjected to amplification in parallel for each patient. significant changes in PBMC RNA levels after vaccination when the mean value of baseline samples wasused as a control for individual patients, thereweremarked HIV-I RNA increases at later time points in PBMCsfromtwo nonvaccinated control patients (subjects IS and 78) that reduced the significance of vaccine-related HIV-I induction in the overall study population. In retrospect, this type of variation in the control subjects wouldbeexpected if immune stimulation by environmental antigens has an influence on virus replication. We have followed study patients longitudinally to determine the relationship between virologic response to vaccination, and clinical outcome. At more than 3 years mean follow-up, 12 of 20 vaccinated subjects have developed AIDS, and 8 have died. We have indicated the CD4' lymphocyte counts at baseline, and 6 months after enrollment in Table 1. Of the I O vaccinated patients who exhibited a fourfold increase in HIV-I RNA, S had a fall in CD4' lymphocyte number at 6 months of20% or more,andall 5 of these subjects developed AIDS. Moreover, 3 of S vaccinated subjects with HIV-I RNA increases who did not have a decrease in CD4 cell count have not developed AIDS. Finally, 3 of the 10 study subjects whodid not show an HIV-I RNA increase developed AIDS over 6 months, and 2 of these patients had a 20% decrease in CD4 cell count. Therefore, the pattern of virologic response to influenzavaccination does not entirely predict outcome. 0the.r factors appear to be involved in determining the rate of clinical progression. DISCUSSION These results show that HIV-I expression in PBMCs markedly increased in one-half of patients during the 2 weeks after influenza vaccination. This appears tobe a transient From www.bloodjournal.org by guest on June 18, 2017. For personal use only. INFLUENZA VACCINE-INDUCED HIV-1 REPLICATION Blood Sampling (Weeks) HIV-I Standards (Relative)Subject -4 -2 3K tK 300 (00 30 10 1085 RT- - 0 +! +2 +4 23 V 33- 44 l C 2 6 - M @ 0 Fig 2. Quantitative HIV-1 PCR analysis of PBMC RNA. PBMC RNA was purified after DNAse I treatment of total PBMC nucleic acid and subjected to in vitro reverse transcription and PCR amplification as described in Materials and Methods. RNA results are of the five patients shown in Fig l.RT indicates amplification of the most positive PBMC sample following incubation at 4°C during the reverse-transcription step. induction that generally does not lead to a sustained increase in virus replication. The importance of cell activation for HIV-I replication has been well shown in vitro. Infection of quiescent PBLs results in an incompletely formed reverse transcript that cannot give rise to infectious virions. Activation of cells with cytokines, lectins, or mitogens either before, or shortly after infection, results in completion of reverse transcription and infectious progeny virions. Chronically HIV-infected cell lines havebeenused as in vitro models for effects of HIV-I activation. Cell clones chronically infected with HIV-I LAV were established from the monocytoid cell line U937 or the T-cell line CEM (U1 and ACH2 cell clones, respectively), but generally produced low levels of HIV-I .3s.3h When these cell lines are activated by cytokines or other agents, viral RNA and progeny virion production is increased in association with increases in a variety of cellular factor~.*~.''~~' Reporter constructs have also shown increased LTR-driven chloramphenicol acetyl transferase (CAT) expression in cell lines activated with mitogens andor cytokines." There have been other reports suggesting a relationship between immune activation in vivo and induction of HIV-I replication. Treatment of HIV-l -infected chimpanzees with various vaccine preparations, or adjuvant alone, caused transient increases in numbers of infectious PBMCs.4" Suggestive evidence indicates that both influenza vaccination and influenza virus infection in patients can increase numbers of HIV-I -infected PBMCs.4' We chose to focus our analysis on changes in PBMC HIV-I RNA, rather than extracellular virus, because of the immediacy of the response to stimulation. Cell activation appears to invoke production of factors that can induce HIV1 expression, and leadto detectable increases in PBMC HIVI RNA.*4 Weaddressed extracellular virus levels using quantitative viral titers in plasma, which yielded similar results. However, plasmaviral titer isless sensitive than cellular HIV-I RNA assays for several reasons. First, infectious assays measure only virus competent for replication in culture. Furthermore, plasma virus assays may be affected by factors elaborated from CD8' lymphocytes, as well as by antigen-antibody complexing of virions. It will be important to confirm our observation in cells using the newer plasma HIV-I RNA assays. Recent studies'".'' have concluded that activation of latently infected PBMCs is not the major source of plasma viremia. Rather, these data suggest that plasma virus originates either from recently infected cells," or via trafficking through the lymphoreticular system."' Therefore, although we show an increase in HIV-I RNA in circulating PBMCs, activation may result in HIV-I induction in either the intravascular or the tissue compartments. We do not believe that the HIV-l induction observed is a result of the specific response to influenzaantigen, because there is a fairly small population of influenza-specific memory cells:* Furthermore, most patients in our study are not expected to mount a measurable specific response to vacThe HIV-I induction may be a consequence of a generalized immune response resulting from antigen presentation by macrophages and dendritic cells. This could cause cytokines to be produced that result inboth activation of latently infected cells and induction of virus expression, as well as increased replication from infection of newly activated cells. There are several potential explanations for the transient nature of the HIV-l induction seen in our study. First, the period of viral induction may be limited by the duration of minor specific T-cell responses to antigen. As influenzaspecific T-cell clones return to quiescence or the memory state, cell factors involved in augmenting virus expression are also down regulated.*'Alternatively, stimulation of HIVinfected, influenza-specific T cells may result in deletion of the infected population, and a subsequent decrease in HIV-I expression. This phenomenon has previously been shown after in vitro antigenic stimulation of PBMCs from HIV-infected asymptomatic individuals, butwasnot addressed in this study:6 Finally, the fall in virus expression may be related to immune clearance of cells acutely expressing viral antigens. Our studies cannot distinguish between these possibilities. With this in mind, it is unclear why two control subjects exhibited a substantial increase in viral RNA production during the course of the study. Although we cannot document this, it is possible that subclinical infection or other immune stimuli such as an allergic reaction could have led to this induction of viral expression. This is consistent with our hypothesis that other activation events in addition to influenza vaccination can affect HIV-l replication. However, there was no evidence in our study for increases in HIV-I DNA load over the short term. Because most pa- From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1086 O’BRIEN ET AL Table 1. Study Patients Characteristics and Response t o Vaccination Patient at No. of CD4 Cells CDC Entry ImmunizationStage Age Previous Influenza No. of CD4 Cells at 6 Mos No No 63 240 308 286 20 Relative RNA Change Vaccinated Ola 287 258 189 02 03a 04 01b 07 08 09 10 03b 21 22 23 28 29 30 31 33 56 61 Controls 12 15 26 34 47 48 75 77 78 79 80 81 83 88 49 63 42 49 256 225 263 313 50 45 57 43 65 30 37 47 51 43 46 38 31 46 41 52 39 39 37 41 59 220 259 41 351 232 111 II II IV c IV B IV c II II II IV c 287 111 IV A 111 IV c 55 4 121 348 535 365 485 474 547 250 301 283 232 321 204 352 446 235 218 111 Ill IV c 111 II IV c 111 II II IV c II 111 IV c IV A II IV c IV c IV c II IV B -0.29 Yes 7.78 4.59 No Yes No Yes Yes Yes Yes9.15 Yes Yes 63.15 Yes Yes 0.17 Yes 0.44 Yes Yes Yes Yes Yes 0.20 16.79 16.15 -0.30 0.01 No No No No No No Yes Yes No Yes No No No No 258 194 260 375 240 4 270 165 410 275 56 320 583 61 409 228 490 553 316 104 59 226 287 56 399 443 255 285 4.94 4.85 10.07 -0.60 79.04 0 -0.74 -0.14 8.96 -0.54 0.73 39.55 0.03 -0.80 0.32 1.96 -0.74 -0.18 0 0.92 0 0 Demographic and clinical data of study patients enrolled over three successive influenza vaccination seasons (1990, 1991, and 1992). CD4 cell counts are expressed per cubic millimeter; values shown are at enrollment, and at 6 months after immunization. Quantitative RT-PCR was performed on PBMC extracts obtained on three occasions during the month before and again at 1,2, and 4 weeks postvaccination. Relative RNA change is defined in Materials and Methods. tients were receiving antiretroviral therapy with zidovudine, new viral DNA formation would be inhibited, even in patients exhibiting marked increases inHIV-1 RNA expression. In addition, our assay would not reliably detect increases in HIV-1 DNA of twofold or less, which may still be relevant for clinically important increases in proviral burden. It is also possible that vaccination increased the number of infected cells in compartments not assayed here, such as lymphoid tissues. Although in our study, we did not detect increases in HIV-1 DNA over 2 months, it seems likely that the progressive increases in viral load during the course of HIV disease are a consequence of many such small inductions of HIV-1 replication which occur intermittently over several years. Our study involved onlya single immune stimulation event which may be inconsequential to a chronic disease such as AIDS where an infected individual is expected to be exposed to numerous antigenic stimuli. Thus, events that stimulate T cells or macrophages may result in adverse consequences for HIV-infected patients. In addition to immune-mediated events, another potential cofactor in HIV-1 pathogenesis is infection with heterologous viruses. Coexpression of HIV and either herpes simplex virus or cytomegalovirus genes in T cells, or stimulation of HIV-infected cells by HTLV particles, can result in increases in HIV-1 repli~ation.4”~~ This increase in HIV-1 RNA expression can be mediated by interaction of herpesvirus products with the HIV-l LTR.’”” In addition, a recent study suggests that recurrent herpes simplex virus infection can also lead to marked increases in HIV-1 expre~sion.~’ Furthermore, actual influenza virus infection may lead to a greater level of HIV-1 expression than the transient nature of the increase in viral expression observed here, because of the prolonged nature of the infection. This relationship may hold true for other vaccine-versus-disease combinations; how- From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1087 INFLUENZAVACCINE-INDUCED HIV-l REPLICATION 0 Fig 3. Plot of peak log R N A postvaccination versus mean log prevaccination for vaccinated IO1 and nonvaccinated control (0)subjects. ever, our study does not distinguish which process has the more deleterious effect in HIV-infected individuals. Therefore, it may be necessary to balance HIV-1 induction by influenza vaccination or other immune-based therapies, with the HIV-1 potentiation effects of other acute infections. However, the relative impact of these phenomena on viral load accumulation and disease progression has not yet been delineated, and it appears likely that progressive viral load increases are a result of repeated episodes of immune activation and subsequent bursts of replication that can occur after a variety of stimuli. This study does not attempt to address the appropriateness of influenza vaccination in HIV-infected patients, nor do we suggest that these findings should be generalized to all vaccines. Our study does suggest that it might be prudent to administer antiretroviral therapy to all individuals receiving immune augmentation therapies to minimize potential increases in viral load. The HIV-1 inductive response to influenza vaccination could not be used in our study to predict clinical course. Immunologic and clinical deterioration ensued over a 3-year period in only half of the vaccinated subjects who exhibited a fourfold or greater increase in HIV-1 RNA expression. Notably, patient 03, who showed vaccine-related HIV-l induction in 2 different years, has had stable CD4+ lymphocyte counts for over 6 years, and is still without AIDS. Viral strain differences and/or differences in host response may account for the weak correlation between HIV-1 induction and clinical outcome. In addition, the efficacy of vaccination, as well as the HIV-1 response, varies in patients even at similar stages of disease. Our initial evaluation focused on patients at an intermediate stage of HIV-1 disease. Although there were three patients below 200 CD4+ lymphocytes/mm3 and two above 500/mm3at study entry, none of the patients had been diagnosed with AIDS. However, it is likely that patients at different stages of disease may exhibit distinct responses. At early stages of disease (patients with over 500 CD4+ lymphocytes/ m m 3 ) , proliferative responses to antigenic stimulation tend to be more v i g o r o ~ s . ~ These ~ . ~ ’ patients also show lower virus and more effective antiviral immunologic re- 1 2 3 4 Log R N A Before Immunization (Relative Copy Number) spon~es,5~.~’ which may prevent detectable viral induction. However, patients at advanced stages of disease (<200 CD4+ lymphocytes/mm3)show markedly impaired proliferative responses to antigen:’”’ and have high background levels of HIV-1 replication. The virologic response to immune stimulation at early or late stages of disease is notwell described. Individual genetic diferences are also likely to be important. For example, differences in response to immunization have been shown in patients based on HLA haplotype.’jO Our studies suggest the need for expanded clinical trials to identify subgroups of patients who might be expected to benefit mostfrom vaccination and other immune-based therapies, as well as those in whom vaccination is not helpful and, in fact, may be deleterious. The significance of transient viral induction needs to be assessed using other assays and long-term clinical observation, and inHIV-infected individuals at different stages of disease. ACKNOWLEDGMENT We thank DXGrace Aldrovandi for critical review of the manuscript, Thang Nguyen for8-actin RT-PCR assays, Felicitas Lorenzo and Carole Silbar for data and sample collection, Yun Chon for help withthedata analysis, and Michelle Estrellado andMizue Aizeki for manuscript preparation. REFERENCES 1. LangW,PerkinsH,Anderson RE, RoyceR, Jewel1 N, and WinkelsteinWJ:Patterns of T lymphocytechangeswithhuman immunodeficiency virus infection: From seroconversionto the development of AIDS. J Acquir Immune Defic Syndr 2:63, 1989 2. Biggars A J : AIDS incubation in 1891 HIV seroconverters from different exposure groups. International Registryof Seroconverters. AIDS 4:1059, 1990 3. Daar ES, Moudgil T, Meyer Ho DD: Transient high levels of viremia in patients with primary human immunodeficiency virus type 1 infection. N Engl J Med 324:961, 1991 4. ClarkSJ, Saag MS, Decker WD, Campbell-Hill S, Roberson JL, Veldkamp PJ, Kappes JC, Hahn BH, Shaw GM: High titers of cytopathicvirusinplasma of patientswithsymptomaticprimary HIV-1 infection. N Engl J Med 324:954, 1991 RD. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1088 5 . Fox CH, Tenner-Racz K, Racz P, Firpo A, Pizzo PA, Fauci AS: Lymphoid germinal centers are reservoirs of human immunodeficiency virus type 1 RNA. .lInfect Dis 164:1051, 1991 6. Pantaleo G, Graziosi C, Demarest JF, Butini L, Montroni M, Fox CH, Orenstein JM, Kotler DP, Fauci AS: HIV infection is active and progressive in lymphoid tissue during the clinically latent stage of disease. Nature 362:355, 1993 7. Embretson J, Zupancic M, Ribas JL, Burke A, Racz P, TennerRacz K, Haase AT: Massive covert infection of helper T lymphocytes and macrophages by HIV during the incubation period of AIDS. Nature 362359, 1993 8. Safrit JT, Andrews CA, Zhy T, Ho DD, Koup RA: Characterization of HIV-l-specific cytotoxic T lymphocyte clones isolated during acute seroconversion: Recognition of autologous virus sequences within a conserved immunodominant epitope. J Exp Med 179:463, 1994 9. PiatakM, Saag MS,Yang LC, Clark SJ, Kappes JC, Luk K-C,HahnBH, Shaw GM, Lifson JD: High levels of HIV-I in plasma during all stages of infection determined by competitive PCR. Science 259:1749, 1993 IO. Wei X, Ghosh SK, Taylor ME, Johnson VA, Emini EA, Deutsch P, Lifson JD, Bonhoeffer S, Nowak MA, Hahn BA, Saag MS, Shaw GM: Viral dynamics in human immunodeficiency virus type 1 infection. Nature 373:117, 1995 11. Ho DD, Neumann AU, Perelson AS, Chen W, Leonard JM, Markowitz M: Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 373:123, 1995 12. Schnittman SM, Greenhouse JJ, Psallidopoulos MC, Baseler M, Salzman NP, Fauci AS, Lane HC: Increasing viral burden in CD4’ T cells from patients withhuman immunodeficiency virus (HIV) infection reflects rapidly progressive immunosuppression and clinical disease. Ann Intern Med 113:438, 1990 13. Coombs RW, Collier AC, Allain JP, Nikora B, Leuther M, Gjerset GF, Corey L Plasma viremia in human immunodeficiency virus infection. N Engl J Med 321:1626, 1989 14. Ho DD,Moudgil T, Alam M: Quantitation of human immunodeficiency virus type I in the blood of infected persons. N Engl J Med 321:1621, 1989 15. Saag MS, Crain MJ, Decker WD, Campbell-Hill S, Robinson S, Brown WE, Leuther M, Whitley RJ, Hahn BH, Shaw GM: Highlevel viremia in adults and children infected with human immunodeficiency virus: Relation to disease stage and CD4’ lymphocyte levels. J Infect Dis 16472, 1991 16. Connor RI, Mohri H, Cao Y, Ho DD: Increased viral burden and cytopathicity correlate temporally with CD4’ T-lymphocyte decline and clinical progression in humanimmunodeficiencyvirus type l-infected individuals. J Virol 67:1772, 1993 17. Shaw GM, Harper ME, Hahn BH, Epstein LG, Gajdusek DC, Price RW, Navia BA, Petito CK, O’Hara CJ, Groopman JE, Cho E-S, Oleske JM, Wong-Stall F, Gallo RC: HTLV-I11 infection in brains of children and adults with AIDS encephalopathy. Science 227:177, 1985 18. Michael NL, Vahey M, Burke DS, Redfield RR: Viral DNA and mRNAexpression correlate with thestage of human immunodeficiency virus (HIV) type 1 infection in humans: Evidence for viral replication in all stages of HIV disease. J Virol 66:310, 1992 19. Daar ES, Chernyavskiy T, Zhao J-Q, Krogstad P, Chen IYS, Zack JA: Sequential determination of viral load and phenotype in human immunodeficiency virus type 1 infection. AIDSResHum Retroviruses 11:3, 1995 20. Nabel G, Baltimore D: An inducible transcription factor activates expression of human immunodeficiencyvirus in T cells. Nature 326:711, 1987 21. Jones KA, Kadonaga JT, Luciw PA, Tjan R: Activation of O’BRIEN ET AL theAIDS retrovirus promoter by the cellular transcription factor. Science 232:755, 1986 (suppl) 22. Garcia JA, Wu FK, Mitsuyasu R, Gaynor RB: Interactions of cellular proteins involved in the transcriptional regulation of the human immunodeficiency virus. EMBO J 6:3761, 1987 23. Gaynor R: Cellular transcription factors involved i n the regulation of HIV-I gene expression. AIDS 6:346, 1992 24. Zack JA, Arrigo SJ, Weitsman SR, Go AS, Haislip A, Chen ISY: HIV-I entry into quiescent primary lymphocytes: Molecular analysis reveals a labile. latent viral structure. Cell 6 I :2 13, 1990 25. Zack JA, Haislip AM, Krogstad P, Chen ISY: Incompletely reverse-transcribed human immunodeficiency virus type 1 genomes in quiescent cells can function as intermediates in the retroviral life cycle. J Virol 66: 17 17, I992 26. Stevenson M, Stanwick TL, DempseyMP, Lamonica CA: HIV- I replication is controlled at the level of T cell activation and proviral integration. EMBO J 9:155 I, 1990 27. Bukrinsky MI, Stanwick TL, Dempsey MP, Stevenson M: Quiescent T lymphocytes as an inducible virus reservoir in HIV-I infection. Science 254:423, 1991 28. Koyanagi Y, O’Brien WA, Zhao JQ. Golde DW, Gasson JC, Chen ISY: Cytokines alter production ofHIV from primary mononuclear phagocytes. Science 241: 1673, 1988 29. Rich EA, Chen ISY, Zack JA, Leonard ML, O’Brien WA: Increased susceptibility of differentiated mononuclear phagocytes to productive infection withhuman immunodeficiency virus expression. J Clin Invest 87: 176, 1992 30. AICP: Preventionand control of influenza-part I, vaccines: Recommendation of the AdvisoryCommittee on Immunization Practices. MMWR 42:1, 1993 (publication no. RR-6) 31. Amgo SJ, Weitsman S, Rosenblatt JD, Chen ISY: Analysis of rev gene function on human immunodeficiency virus type I replication in lymphoid cells by using a quantitative polymerase chain reaction method. I Virol 63:4975, 1989 32. Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchl R, Horn GT, Mullis KB, Erlich HA: Primer-directed enzymatic amplification ofDNAwith a thermostable DNA polymerase. Science 239:487, 1988 33. O’Brien WA,Koyanagi Y, Namazie A, Zhao J-Q, Diagne A, Idler K, Zack JA, Chen ISY: HIV-I tropism for mononuclear phagocytes can be determined by regions of gp120 outside the CD4binding domain. Nature 348:69, 1990 34. Koyanagi Y, Miles S, Mitsuyasu RT, Merry1 JE, Vinters HV, Chen ISY: Dual infection of the central nervous system by AIDS viruses with distinct cellular tropisms. Science 236:819, 1987 35. Folks T, Powell DM, Ligbtfoote MM, Benn S, Martin MA, Fauci AS: Induction of HTLV-III/LAV from a nonvirus-producing T cell line: Implications for latency. Science 231:600, 1986 36. Poli G, Kinter A, Justement S, Kebrl JH, Bressler P, Stanley S, Fauci AS: Tumor necrosis factor alpha functions in an autocrine manner in the induction of human immunodeficiency virus expression. Proc Natl Acad Sci USA 87:782, 1990 37. Folks T M , Justement J, Kinter A, Dinarello CA, Fauci AS: Cytokine-induced expression of HIV-l in a chronically infected promonocyte cell line. Science 238:800, 1987 38. Folks TM, Clouse KA, Justement J, Rabson A, Duh E, Kehrl JH, Fauci AS: Tumor necrosis factor induces expression of human immunodeficiency virus in a chronically infected T-cell clone. Proc Natl Acad Sci USA 86:2365, 1989 39. Latham PS, Lewis AM, Varesio L, Pavlakis GN, Felber BK. Ruscetti F W , Young HA: Expression of human immunodeficiency virus long terminal repeat in the human promonocyte cell line U937: Effect of endotoxin and cytokines. Cell Immunol 129513, 1990 40. Fultz PN, Guckman JC, Muchmore E, Girard M: Transient increases in numbers of infectious cells in an HIV-infected chimpan- From www.bloodjournal.org by guest on June 18, 2017. For personal use only. INFLUENZA VACCINE-INDUCED HIV-l REPLICATION zee following immune stimulation. AIDS Res Hum Retroviruses 8:313, 1992 41. Ho DD: HIV-l viremia and influenza. Lancet 1:1549, 1992 42. Sabbaj S , Para MF, Fass W,Adams PW, Orosz CG, Whitacre CC: Quantitation of antigen-specific immune responses in human immunodeficiency virus (W)-infected individuals by limiting dilution analysis. J Clin Invest 12:216, 1992 43. Huang KL, Ruben FL, Rinaldo CR. Kingsley L, Lyter DW, Ho M: Antibody responses after influenza and pneumococcal immunization in HIV-infected homosexual men. JAMA 257:2047, 1987 44. Nelson KE, Clements ML, Miotti P, Cohn S, Polk B F The influence of human immunodeficiency virus (HIV) infection on antibody responses to influenza vaccines. Ann Intem Med 109:383,1988 45. Miotti PG, Nelson KE, Dallabetta GA, Farzadegan H, Margolick J, Clements M L The influence of HIV infection on antibody responses to a two-dose regimen of influenza vaccine. JAMA 262:779, 1989 46. Groux H, Torpier G, Monte D, Mouton Y, Capron A, Ameisen JC: Activation-induced death by apoptosis in CD4+ T cells from human immunodeficiency virus-infected asymptomatic individuals. J Exp Med 175:331, 1992 47. Tremblay M,Gornitsky M, Wainberg M: Active replication of human immunodeficiency virus type 1 by peripheral blood mononuclear cells following coincubation with herpes viruses. J Med Virol 29:109, 1989 48. Ostrove JM, Leonard J, Week K, Rabson AB, Gendelman H E Activation of the human immunodeficiency virus by herpes simplex virus type 1. J Virol 61 :3726, 1987 49. Cesareale D, Fiala M, Chang CM, Cone LA, Mocarski ES: Cytomegalovirus enhances lysis of HIV-infected lymphoblasts. Int J Cancer 44:124, 1989 50. Zack JA, Cann AJ, Lug0 JP, Chen ISY: HIV-l production from infected peripheral blood T cells after HTLV-l induced mitogenic stimulation. Science 240:1026, 1988 5 1. Laurence J: Molecular interactions among herpesviruses and human immunodeficiency viruses. J Infect Dis 162:338, 1990 1089 52. Barry P, Pratt-Lowe E, Peterlin BM, Luciw P: Cytomegalovirus activates transcription directed by the long terminal repeat of human immunodeficiency virus type 1. J Virol 64:2932, 1990 53. Mosca JD, Bednarik DP, Raj NBK, Rosen CA, Sodroski JG, Haseltine WA, Pitha PM: Herpes simplex virus type 1 can reactivate transcription of latent human immunodeficiency virus. Nature 325:67, 1990 54. Gimble JM, Duh E, Ostrove J M , Gendelman HE, Max EE, Tabson AB: Activation of the human immunodeficiency virus long terminal repeat by herpes simplex virus type 1 is associated with induction of a nuclear factor that binds to the NF-kB/core enhancer sequence. J Virol 62:4104, 1988 55. Mole L, Ripich S , Margolis D, Holodniy M: Plasma HIV RNA levels are increased during active Herpes simplex virus i n k tion. Abstracts of the 2nd National Conference on Human Retroviruses and Related Infections, Washington, DC, January 29-February 2, 1995 (abstr 239) 56. Trauger RJ, Giermakowska WK. Ferre F, Duffy PC, Wallace MR. Lewis DE, Beecham W ,Bumett KG, Jensen FC, Carlo DJ: Cell-mediated immunity to H I V - 1 in Walter Reed stages 1-6 individuals: Correlation with virus burden. Immunology 78:611, 1993 57. Fauci AS: Multifactorial nature of human immunodeficiency virus disease: Implications for therapy. Science 262:1011, 1993 58. Clerici M, Stocks WI, Pajacra RA, Roswell RN, Lucey DR, Via CS, Shearer GM: Detection of three distinct patterns of T helper dysfunction in asymptomatic HIV seropositive patients. J Clin Invest 84:1892, 1989 59. Miedema F, Petit AJC, Terpstra FG, Ekflinck Schatternkerk JKM, de Wolf F, AI BJM, Roos M, Lange JMA, Danner SA, Goudsmit J, Schellenkens PTA: Immunological abnormalities inhuman immunodeficiency virus (W)-infected asymptomatic homosexual men. J Clin Invest 82:1908, 1988 60. Cunningham-Rundles S , Brown S , Gross D, Braun D, Hansen JA, Good RA, Armstrong D, Dupont B: Association of HLA in immune response to influenza-A immunization. Transplant Proc 11:1849, 1979 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1995 86: 1082-1089 Human immunodeficiency virus-type 1 replication can be increased in peripheral blood of seropositive patients after influenza vaccination WA O'Brien, K Grovit-Ferbas, A Namazi, S Ovcak-Derzic, HJ Wang, J Park, C Yeramian, SH Mao and JA Zack Updated information and services can be found at: http://www.bloodjournal.org/content/86/3/1082.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.