Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Rheumatic fever wikipedia , lookup
Artificial heart valve wikipedia , lookup
Aortic stenosis wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Detection of Pulmonic and Tricuspid Valvular
Regurgitation by Means of Indicator Solutions
By N. PERRYMAN COLLINS, M.D., EUGENE BRAUNWALD, M.D.,
AND
ANDREW G. MORROW, M.D.
The presence of pulmnonic and tricuspid valvular regurgitation may often be suspected
from careful clinical examination. However, the validity of the generally accepted
clinical criteria remain to be established by technics that permit the direct demonstration
of reverse flow across these valves during life. This has been made possible by the detection of cardiogreen and of radioactive krypton (Kr85) in the right atrium or right
ventricle after injection of these substances into a distal chamber.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
heart catheterizatioii, and to present the results obtained ill 29 patients studied at the
National Heart Institute. A similar approach
to diagnosis has also been described recently
by Bajec, Birkhead, Carter, and Wood.10
A LTHOUGH the presence of valvular regurgitation may be suspected from clinical studies, the actual demonstration of blood
traversing a valve in reverse direction is
necessary for a definitive diagnosis. Indicatordilution curves recorded from a systemic
artery following injections into the right side
of the heart are often modified by the presence
of a regurgitant valve between the sites of
injection and of sampling.1-3 Decreased cardiac output or a left-to-right shunt may, however, obscure the changes produced in such
curves by valvular regurgitation.
Mitral regurgitation has been demonstrated
by the prompt appearance in the left atrium
of either an indicator dye4' 5or of a radiopaque medium" following injection into the
left ventricle. In the presence of aortic regurgitation, indicator dye injected into the descending thoracic aorta regurgitates to the
ascending aorta and may be detected in the
right ear. This lesion may also be demonstrated by thoracic aortography.8 The reflux
of radiopaque dye into the right ventricle
following its injection into the pulmonary
artery has recently been observed in the presence of pulmonic regurgitation.9
It is the purpose of this report to describe
2 technics for the detection of pulmonic and
tricuspid valvular regurgitation that may be
applied conveniently at the time of right
,tL
METHODS
From the Clinic of Surgery, National Heart Institute, Bethesda, Md.
*Manufactured by Nuclear Corporation of America,
Brooklyn, N. Y.
561
Right heart catheterization was performed with
a no.-9 double-lumen Cournand catheter, modified
so that the openings of the 2 lumina were 5 cia.
apart. When the competency of the pulnmonic
valve was studied, the catheter was positioned so
that the distal opening was in the pulmonary artery
and the proximnal one in the right ventricle. When
tricuspid valve function was examined, the distal
lumen opened into the right ventricle, while the
proximal opened into the right atrium. Simultaneous pressures were recorded from each chamnber immediately prior to and following injection
of the indicator in order to confirm the position of
the catheter.
Cardiogreen (tricarboeyanine) dye" was injected through the distal opening of the catheter
as blood was sampled continuously from the proximal opening (fig. 1). The concentration of the
indicator was determined by withdrawal through
a euvette densitometer12 by means of a constantrate motor-driven syringe. Time-coneentration
curves were recorded either with a photographic
cathode-ray instrument or a direct-writing recorder.
The order of magnitude of the relationship between regurgitant and forward flows was estimated
by the "forward triangle" method described by
Hetzel and collaborators.13 14 The "regurgitant
fraction" was calculated as the ratio of the product of the build-up time and peak-concentration of
the "regurgitant curve" to that of the "recirculation curve" (fig. 2). It is realized that this ratio
does not provide precise quantification.
Circulation, Volume XX, October 1951
,
COLLINS, BRAUNWALD, MORROW
r.)
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
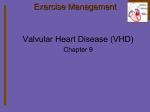
FIG. 1. Representation of the test for competency of the pulmonic valve with cardiogreen
dye. Dye is injected through the distal opening of the catheter, and regurgitates back into
the right ventricle. It is detected by sampling right ventricular blood from the proximal opening of the catheter through a cuvette densitometer.
In 12 of the 29 patients valvular competency
studied in a similar manner with injections of
30 to 50 jac. of radioactive krypton (Kr85) solution into the distal opening of the catheter. Immediately after injection blood was sampled at a
constant rate for 10 seconds from the proximal
lumen and for 15 seconds from a systemic artery.
The radioactivity in these samples was then measured by inserting themn into a continuous gas-flow
Geiger-Muller tube.
was
RESULTS
In the presence of a competent valve, either
no dye or only a minimal quantity appeared
in the proximal chamber immediately after
injection; Fifteen to 20 seconds after injection, dye that had recirculated through the
systemic circuit appeared (figs. 3 and 4).
When valvular regurgitation was present, a
substantial amount of dye appeared in the
proximal chamber within 2 seconds of the
onset of the injection, well before the appearance of the recirculation curve (figs. 2 and 5).
In the presence of valvular regurgitation combined with a left-to-right shunt entering upstream to the proximal catheter opening, the
curve produced by the regurgitant valvular
flow was inscribed significantly earlier than
the curve produced by the shunted blood; the
latter, while delayed in its path through the.
pulmonary circulation and to the right side
of the heart, nevertheless appeared earlier
than the systemic recirculation curve (fig. 6).
The competency of the pulmonic valve was
examined in 28 patients, and in 7 of these
significant regurgitation was considered to be
present with "regurgitant f -actions" ranging
from 17 to 72 per cent. Three of these 7 patients (W.J., J.B., J.S.) had previously had
portions of their pulmonic valves excised at
the time of pulmonary valvulotomy, but only
2 (J.B., J.S.) had murmurs considered typical
of pulmonic regurgitation. Another patient
(M.B.) had previously undergone pulmonic
valvulotomy and closure of a small ventricular septal defect in which no valvular tissue
was removed. A murmur typical of pulmonic
regurgitation developed. One patient (C.C.)
had mitral regurgitation, pulmonary hypertension, and a typical Graham Steell murmur.
DYE DETECTION OF REGURGITATION
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Patient J.K., who had not been operated upon,
had the murmurs considered typical of pulmonic stenosis and regurgitation. At right
heart catheterization, there was a gradient of
26 mm. Hg across the pulmonary valve, and
the diastolic pressures in the pulmona; y artery and right ventricle were identical. The
seventh patient (S.C.) had an atrial septal
defect, pulmonary hypertension and a typical Graham Steell murmur; the presence of
pulmonic regurgitation was confirmed at the
time of operative closure of the defect when
a distinct jet of blood was felt in the right
ventricle during diastole. In only 3 (W.J.,
J.K., M.B.) of these 7 patients was the enddiastolic pressure in the pulmonary artery
identical to that in the right ventricle. Pulmonary regurgitation was not suspected in 5
other patients who had "regurgitant fi actions" ranging from 2 to 6 per cent. It is believed that such minute amounts of reflux do
not necessarily indicate organic valvular dysfunction, but are presumably artifacts produced by the presence of the catheter. There
was no relation between the presence of this
small degree of regurgitation and the pulmonary artery pressure.
The competency of the tricuspid valve was
tested in 17 patients and in 8 of these significant regurgitant flow was demonstrated. The
" regurgitant fractions" ranged from 11 to
65 per cent in 7 of the patients and could not
be calculated in the eighth, a patient with a
very prolonged circulation time in whom no
recirculation curve had appeared after 55
seconds of sampling. In all 8 of these patients
there was clinical evidence of tricuspid regurgitation and the right ventricular pressure
was elevated (table 1); in 5 of these, the mean
right atrial pressure and the right atrial "v"
wave pressures were elevated. In 2 of the patients with significant tricuspid regurgitation
the diagnosis was confirmed at subsequent
postmortem examination. In one of these patients, J.O., the tricuspid ring was widely
dilated and the valve leaflets were held in a
position of partial inversion into the right
ventricle. Ill the other patient, A.R., the tricuspid valve was both stenotic and regurgi-
5 63
1) S
E4
Injection
R.A.Sampli
R.V.
T. R.
W7
P. A. Injection
R.V. Sampling
1M ECIRC,
tOQ
LLIIi
R.V. Injection
R.A.Sampling
SEC-.
_
h
h
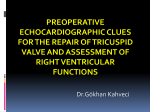
FIG. 2 Top. Indicator-dilution curve obtained after
right ventricular injection and right atrial sampling
in a patient with rheumatic heart disease, mitral stenosis and regurgitation and tricuspid regurgitation.
Verlical arrow, time of injection. The first upward
deflection (T.R.) represents the dye that regurgitated
across the tricuspid valve. The systemic recirculation
curve is seen on the right (RECIRC.). 1-2, build-up
timie; 2'-3, peak concentration of the regurgitant
curve; 4-5, build-up time; 5-6, the peak concentration
of the recirculation curve. Tricuspid regurgitation
was also revealed waith the Kr' test performed on this
lPatiellt.
FIG. 3 Middle. Dye-dilution curve resulting from
pulmonary artery injection and right ventricular sampling in patient L.R. with rheumatic heart disease,
mitral stenosis, and aortic insufficiency. The absence
of dye in right ventricular blood prior to recirculation
is thought to exclude pulmonic regurgitation. The Kr'
test also showed the absence of pulmnonic regurgitatioln.
FIG. 4 Bottom. Dye-dilution curve after right ventricular injection and right atrial sampling in a patient without tricuspid regurgitation.
taut, rigid and immobile with a fixed opening
1.5 cm. in diameter. Patient S.C. had an atrial
septal defect with pulmonary and right ventricular systolie hypertension. The tricuspid
regurgitant fraction was 11 per cent and a
small regurgitant jet was palpable at opera-
564
COLLINS, BRAUNWALD, MORROW
P.A. Injection
R.V. Sampling
'i
110
SEC-j
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
FIG. 5 Top. Dye-dilution curve obtained from the
right ventricle following pulmonary artery injection
in a patient with pulmonary regurgitation. The dye
that appears immediately (P.R.) indicates pulmonic
reflux and precedes the recirculation curve (RECIRC.).
FIG. 6 Bottom. Dilution curve resulting from pulmonary artery injection and right ventricular sampling in a patient who had a portion of his pulmonic
valve excised at the time of pulmonary valvotomy for
pulmonic stenosis. A left-to-right shunt due to an
atrial septal defect persisted. The first component of
the curve (P.R.) is indicative of pulmonic regurgitation, the second (L.R.) is related to blood that has
been shunted across the atrial septal defect, and the
third component (RECIRC.) is due to systemic recirculation.
tion. In only one instance minimal ("catheter
induced ") tricuspid regurgitation was encountered with regurgitant fraction of 3 per
cent.
It has been demonstrated previously that
approximately 95 per cent of Kr85 injected
into the venous system or right side of the
heart is eliminated into the expired air during its passage through the pulmonary cireulation.15-18 The small remaining fraction that
reaches the systemic arterial bed does not behave in a fashion similar to a simple intravascular indicator such as cardiogreen. A
portion leaves the intravascular compartment
and diffuses into the interstitial fluid as well
as into the cells,19 further diminishing the
quantity of Kr85 in the systemic venous blood
immediately after injection into the right side
of the heart or pulmonary artery. The presence of Kr85 in the blood sampled from the
right atrium or right ventricle immediately
after injection into the right ventricle or pulmonary artery could therefore result only
from valvular regurgitation.
Twelve patients had both Kr85 and cardiogreen dye tests for pulmonic regurgitation
while 5 had both tests for tricuspid regurgitation. The results were in general agreement.
In 8 tests the cardiogreen "regurgitant fraction" exceeded 15 per cent and the right heart
Kr85 count per minute (c.p.m.) exceeded
background by more than 100 c.p.m. Similarly, in 7 tests the cardiogreen regurgitant
fraction ranged between 0 and 3 per cent while
the right heart Kr85 activity ranged between
0 and 54 c.p.m. above background. However,
the results in the other 2 patients indicated a
discrepancy between the 2 tests. In patient
J.B., significant pulmonic regurgitation was
revealed only by cardiogreen dye while in
patient M.E., it was demonstrated only with
Kr85
DISCUSSION
The technics for the detection of pulmonic
and tricuspid valvular regurgitation described herein have been found simple and
convenient to apply at the time of right heart
catheterization and should prove of considerable clinical value. The diagnosis of pulmonary regurgitation is usually made when a
patient with evidence of pulmonary hypertension presents with a high-pitched, decrescendo, blowing diastolic murmur along the
left sternal border, unaccompanied by the
peripheral dynamics of aortic regurgitation.
Seven such patients wvere studied with an indicator-dilution method for the detection and
estimation of aortic regurgitant flow.7 It was
with considerable surprise that mild aortic
565
DYE DETECTION OF REGURGITATION
TABLE 1.-Results of Dye-Dilution Tests for Valvular Regurgitation
Regurgitant fraction
Pressure
PA
S/D
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
J. P.
R. J.
M. S.
A. L.
D. D.
M. B.
P. D.
A. R.
AI. P.
T. L.
L. M.
R. P.
W. J.
J. B.
C. C.
H. E.
S. C.
J. S.
C. M.
C. H.
J. 0.
R. J.
IL. R.
D. M.
M. E.
D. W.
J. K.
B. S.
M. B.
27/11
22/7
42/20
29/10
54/12
34/14
47/34
80/40
72/34
25/9
40,20
41/23
20/3
64/30
RV
S/D
28/1
22/4
42/8
33/1
54/0
35/4
48/4
80/10
73/7
28/5
43/4
42/0
45/3
66/10
RA
Mean
V Wave
4
3
7
2
1
5
5
10
8
5
4
5
4
6
2
10
4
1
2
7
7
2
4
3
10
5
4
4
-
6
6
10
3
3
8
7
14
18
6
7
6
6
7
4
16
3
3
3
8
11
3
5
4
15
6
5
4
Tricuspid Pulmonic
0
57
50
65
0
0
0
0
0
0
0
0
0
0
0
0
3
2
53
29
17
2
23
18
Diagnosis
ASD
ASD
MS, MI
PDA
VSD
MS, AI
VSD
rMS, MI, TS, TI
MlS, M I, TI
AS
MS, MI, TI
MS, AI, TS
PS, PI, ASD (postop.)
PI, Tet. of Fallot (postop.)
MI, PI
MS, MI, TI
ASD, PI, TI
PS, PI (postop.)
0
50/3
22
58/5
11
80/4
3
35/0
-MI
0
16/0
2
AI, MS
0
23/6
*
MS, MI, AS, AI, TI
0
70/7
ASD
0
6
16/3
MS, AI
0
54/4
MS, AI
0
22/10
22/10
19
MS, MI, TI
0
40/6
40/20
MS, TI
0
59
75/7
73/34
PS, PI
72
48/8
22/8
AI, MI
0
0
43/5
43/22
VSD, PS, PI (postop.)
55
28/2
28/2
All pressures expressed in mm. Hg: S/D, systolic/diastolic pressures; *large regurgitant
curve but no recirculation curve recorded; ASD, atrial septal defect; MS, mitral stenosis;
MI, mitral insufficiency; PDA, patent ductus arteriosus; AI, aortic insufficiency; VSD, ventricular septal defect; TI, tricuspid insufficiency; TS, tricuspid stenosis; AS, aortic stenosis;
PS, pulmonic stenosis; PI, pulmonic insufficiency.
50/20
56/14
78/30
15/5
15/7
23/7
68/38
18/6
50/30
regurgitation was discovered in 6 of these 7
patients believed on clinical grounds to have
pulmonary regurgitation. If the indicatordilution methods are applied to the study of
both the aortic and pulnionic valves, the origin of any diastolic murmur due to regurgitation may be determined. A patient recently
studied illustrates the clinical application of
these technics.
L.R. (Clinical Center #00-24-61), an 18year-old girl, was admitted for diagnostic
study and the treatment of rheumatic heart
disease. She had had acute rheumatic fever
at 8 years of age and was told shortly thereafter that she had a heart murmur. No symp-
toms ensued until 1 year prior to admission
when exertional dyspnea, easy fatigability,
occasional paroxysmal nocturnal dyspnea, and
hemoptysis began. On physical examination
the blood pressure was 106/70; the pulse was
94 and regular. The point of maximal impulse
was in the left midelavicular line in the fifth
left intercostal space and there was only a
slight right ventricular lift. At the apex the
first heart sound was accentuated. The second
heart sound in the pulmonic area was loud
and showed normal respiratory splitting. In
the pulmonic area and along the left sternal
border there was a grade-II high-pitched,
decrescendo, blowing diastolic murmur, and
CO56CLLINS, BRAUNWALD, MORROW
566
TABLE 2.-Results of Radioactive Krypton Tests
for Valvular Regurgitation
Right ventricular
injection
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
L. R.
W. J.
H. E.
C. H.
J. O.
L. AI.
J. B.
J. S.
S. C.
D.M.
M. E.
M. B.
-
12
5 79
345
230
0
2
*
65
-
-
139
59
Pulmonary artery
injection
3
301
44
54
0
31
7
199
245
7
1223
0
53
2
2
0
3
29
18
23
0
0
-m30
55
All counts have been corrected for background.
RA, right atrium; RV, right ventricle; *, very large
regurgitant curve, but no recirculation curve recorded.
a grade-TI rumbling diastolie murmur with
presystolic accentuation was heard at the
apex. The electrocardiogram showed right
ventricular hypertrophy and right axis deviation. X-rays revealed the heart to be slightly
enlarged in its transverse diameter and there
was prominence of the main pulmonary artery segment and enlargement of the left
atrium. Right heart catheterization revealed
the pulmonary artery pressure to be 50/30,
the cardiac index was 1.98 lJ./miln./M.2, and
no shunts were preseIit. Transbronchial left
heart catheterization revealed a mean left
atrial pressure of 22 mm. Hg and the enddiastolic gradient across the mitral valve was
20 mm. Hg. It was considered that this patient had mitral stenosis and that the diastolic
murmur along the left sternal border represented pulmonic regurgitation. However, no
regurgitation was demonstrated either by the
dye-dilution method (table 1, fig. 3) or by the
Kr`1S technic (table 2). Retrograde aortic
catheterization and quantification of aortic
regurgitation was then carried out and revealed regurgitation of dye from the thoracic
aorta at the level of the eighth thoracic vertebra to the origin of the innominate artery.
The final diagnosis was severe mitral stenosis
and moderate aortic regurgitation.
In the past, the definitive diagnosis of tricuspid regurgitation has rested primarily on
elinieopathologic correlations. It was suggested by the contour of the right atrial pressure pulse in 60 patients studied by Sepulveda
and Lucas.20 However, tricuspid regurgitation
had been suspected clinically in only 23 per
cent of this group. On the other hand, in the
present investigation, substantial tricuspid
regurgitation was demonstrated in patients
L.M., S.C., and D.W. in whom the right atrial
pressure pulse was normal. In this connection
it is also of interest that the right atrial pressure pulse was not modified in the 4 patients
with congenital left ventriculo-right atrial
communications whom we have recently studied.2' In this malformation, blood is ejected
into the right atrium during ventricular systole in a manner similar to tricuspid regurgitation.
It is anticipated that the methods described
herein will provide a more precise approach
to the diagnosis of tricuspid regurgitation and
make clinico-hemodylamici-pathologic correlations more meaningful than heretofore. The
recognition of tricuspid regurgitation may be
of considerable clinical importance. It has
been pointed out by Schilder and Harvey22
that patients with mitral stenosis and tricuspid regurgitation have been denied commissurotomy because the presence of a loud systolic murmur led to the erroneous diagnosis
of mitral regurgitation. Such diagnostic errors
should be obviated by the recognition of tricuspid regurgitation with the indicator-dilution or radioactive gas technics.
SUMMARY
Technics for the demonstration of pulmonic
and tricuspid regurgitation and the estimation of the magnitude of regurgitant flow are
described. The pulnmonic valve was studied
by positioning a modified double-lumen catheter so that the distal lumen opened into the
pulmonary artery and the proximal lumen
opened into the right ventricle. When tricuspid function was examined, the distal lumen
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
DYE DETECTION OF REGURGITATION
567
opened into. the right ventricle and the proximal one into the right atrium. Cardiogreen
dye and radioactive krypton (Kr85) were injected through the distal opening of the catheter and sampled from the proximal opening.
With a competent valve, either no dye or Kr85
or only a minimal quantity could be detected
in the proximal chamber immediately after
injection. In the presence of valvular regurgitation, substantial amounts appeared in the
proximal chamber immediately after injection. Regurgitation was present in 7 of the
28 patients in whom the pulmoilic valve was
examined, with regurgitant fractions ranging
from 17 to 72 per cent. Tricuspid regurgitation was proved in 8 of the 17 patients studied; the regurgitant fractions were 11 to 65
per cent. The methods described appear reliable, simple to apply in the course of right
heart catheterization, and of clinical value in
the study of patients with known or suspected
valvular heart disease or with heart murmurs
of uncertain etiology.
28 patientes in qui le valvula pulmonic esseva
examinate. lie fractiones regurgitante variava
inter 17 e 72 pro cento. Regurgitation tricuspide esseva constatate in 8 del 17 patientes
studiate. Le fi actiones regurgitante variava
inter 11 e 65 pro cento. Le methodos describite es apparenitemenite digne de confidentia,
simple a applicar in le curso de catheterismo
dextero-cardiac, e de valor clinic in le studio
de pacientes con establite o suspicite morbo
de valvula cardiac o con murinures cardiac
de etiologia inicerte.
SUMMARIO IN INTERLINGUA
Es describite technicas pro le demonstration
de regurgitation pulmonic e tricuspide e pro
le estimation del magnitude del fluxo regurgitante. Lie valvula pulmonic esseva studiate
per positionar un modificate catheter a lumine
duple de inaniera que le lumine distal commnunicava con le arteria pulmonar e le lumime
proximal con le ventriculo dextere. In le examinie del function tricuspide, le catheter
esseva positionate de maniera que le lumine
distal conimunicava con le ventriculo dextere
e le lumine proximal con le atrio dextere. Un
colorante cardio-verde e krypton radioactive
(r1r85) esseva injicite via le lumine distal del
catheter e specimens esseva obtenite ab le
lumine proximal. Quando le valvula es competente, nulle colorante e nulle Kr85 - o al minus solmente un quantitate minimal de illos
- poteva esser detegite in le camera proximal
iInmnediatemente post le injection. In le presentia de regurgitation valvular, quantitates
substantial del indicatores appareva in le
camera proximal inimediatemente post le injection. Regurgitation esseva presente in 7 del
REFERENCES
1. KORNER, P. I., AND SHILLINGFORD, J. P.:
Further observations on the estimation of
valvular incompetence from indicator dilution curves. Clin. Se. 15: 417, 1956.
2. WRIGHT, J. L., AND W.XOOD, E. H.: Localization
of valvular regurgitation. Proc. Staff Meet.,
Mayo Clin. 32: 491, 1957.
3. WOODWARD, F.. J., BURCHELL, H. B., AND
/WOOD, E. H.: Dilution curves associated
with valvular regurgitation. Proc. Staff
Meet., Mayo Clin. 32: 518, 1957.
4. KEYS, J. R., SWAN, H. J. C., AND WOOD,
E. H.: Dye dilution curves from systemic
arteries and left atrium of patients with
valvular heart disease. Proc. Staff Meet.,
Mayo Clin. 31: 138, 1956.
5. WOODWARD, E., JR., SWAN, H. J. C., AND
WOOD, E. H.: Evaluation of a method for
detection of mitral regurgitation from indicator dilution curves recorded from the left
atrium. Proc. Staff Meet., Mayo Clin. 32:
525, 1957.
6. LEHMAN, J. S., MUSSER, B. G., AND LYKENS,
H. D.: Cardiac ventriculography. Direct
transtliori cic needle puncture opacification
of the left (or right) ventricle. Am. J.
Roentgenol. 77: 207, 1957.
7. BRAUNWALD, E., AND MORROW, A. G.: A method for the detection and estimation of aortic
regurgitant flow in man. Circulation 17:
505, 1958.
8. GRANT, R. P., SANDERS, R. J., MORROW, A. G.,
AND BRAUNWALD, E.: Symposium on diagnostic methods in the study of left-to-right
shunts. Circulation 16: 791, 1957.
9. COLLINS, N. P., BRAUNWALD, E., AND MORROW,
A. G.: Isolated congenital pulmonic valvular
regurgitation. Diagnosis by cardiac catheterization and angiocardiography. Am. J.
Med. In press.
10. BAJEc, D. F., BIRKHEAD, N. C., CARTER, S. A.,
COLLINS, BRAUNWALD, MORROW
568
11.
12.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
13.
14.
15.
16.
AND WOOD, E. H.: Localization and estimation of severity of regurgitant flow at the
pulmonary and tricuspid valves. Proc.
StafY Meet., Mayo Clin. 33: 569, 1958.
Fox, I. J., BROOKER, L. G. S., HESELTINE,
D. W., ESSEX, H. E., AND WOOD, E. H.:
A tricarboeyanine dye for continuous recording of dilution curves in whole blood
independent of variations in blood oxygen
saturation. Proc. Staff Meet., Mayo Clin.
32: 478, 1957.
GILFORD, S. R., GREGG, E. D., SHADLE, 0. W.,
FERGUSON, T. B., AND MARZETTA, L. A.:
An improved cuvette densitometer for cardiac output determined by dye dilution
method. Rev. Scient. Inst.unients 2'-: 696,
1953.
HETZEEL, P. S., RAMIREZ DE ARELLANO, A. A.,
AND WOOD, E. H.: Estinmation of cardiac
output from initial portion of arterial indicator-dilution curves. Fed. Proc. 14: 72,
1955.
-, SWAN, H. J. C., RAMIREZ DE ARELLANO,
A. A., AND WOOD, E. H.: Estimation of cardiac output from first part of arterial dyedilution curves. J. Appl. Physiol. 13: 92,
1958.
CHIDSEY, C. A., III, FRITTS, H. W., JR.,
HARDEWIG, A., RICHARDS, D. Wy., AND
COURNAND, A.: Fate of radioactive krypton
(Kr85) introduced intravenously in man. J.
Appl. Physiol. 14: 63, 1959.
BRAUNWALD, E., MORROW, A. G., SANDERS,
R. J., AND LONG, R. T. L.: The characteri-
17.
18.
19.
20.
21.
22.
zation of circulatory shunts by foreign gas
technics. Symposium, Am. Assoc. Advan.
Science, Dec. 1958. In press.
-, LONG, R. T. L., AND MORROW, A. G.: Injections of radioactive krypton (Kr 85)
solutions in the detection and localization
of cardiac shunts. Abstracted, J. Clin. Invest. 38: 990, 1959.
LONG, R. T. I., WVALDHAUSEN, J. A., CORNELL,
W. P., AND SANDERS, R. J.: The detection
of right-to-left circulatory shunts. A new
method utilizing injections of a radioactive
gas, Kr85. Proc. Soc. Exper. Biol. & Med.
In press.
-, LOMBARDO, C. R., AND BRAUNWALD, E.:
The use of radioactive krypton and eardiogreen dilution curves in the detection of experimental portal-systemic venous shunts.
Ann. Surg. In press.
SEPULVEDA, G., AND LUKAS, D. S.: The diagnosis of tricuspid insufficiency. Clinical features in 60 cases with mitral valve disease.
Circulation 11: 552, 1955.
BRAUNWALD, E., AND MORROW, A. G.: Left
ventriculo-right atrial communication: Diagnosis by clinical, hemodynamic and angiographic methods. Am. J. Med. In press.
SCHILDER, D. P., AND HARVEY, W. P.: Confusion of tricuspid incompetence with mitral
insufficiency. A pitfall in the selection of
patients for mitral surgery. Am. Heart J.
54: 359, 1957.
e.
With the invention of the microscope we can mark the first positive step towards the
goal to-day. A Jesuit priest, Kircher, in 1671, was the first to investigate putrefying
meat, milk, and cheese with the crude microscope of his day, and left us indefinite
remarks concerning 'very minute living worms' found therein. Four years after Kircher
a Dutch linen merchant, Antonius von Leeuwenhoek, by improving the lenses of the
microscope saw in rain-water, putrefying fluids, intestinal contents, and saliva, minute,
moving, living particles, which he called 'animalculae.' In medical circles of his day
these observations aroused the keenest interest, and the theory that these 'animalculae'
might be the cause of all disease was eagerly discussed. Plenciz, of Vienna, after much
observation of various fluids, putrefying and otherwise, wrote, in 1762, that it was his
firm belief that the phenomena of diseases and the decomposition of animal fluids were
wholly caused by minute living things.-WILLIAM OSLER. Aequanimitas and Other Addresses. Blakiston & Co., Philadelphia, and T. K. Lewis, London, 1904.
Detection of Pulmonic and Tricuspid Valvular Regurgitation by Means of
Indicator Solutions
N. PERRYMAN COLLINS, EUGENE BRAUNWALD and ANDREW G.
MORROW
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Circulation. 1959;20:561-568
doi: 10.1161/01.CIR.20.4.561
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX
75231
Copyright © 1959 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/20/4/561
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column
of the Web page under Services. Further information about this process is available in the
Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/