Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
1537
Effect of Definition on Incidence
of Postinfarction Pericarditis
Is It Time to Redefine Postinfarction Pericarditis?
Philip B. Oliva, MD; Stephen C. Hammill, MD; James V. Talano, MD
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
P ericarditis is possibly the most common cause of
chest pain after an acute transmural myocardial
infarction without reperfusion.' It occurs in
approximately 28% to 40% of fatal transmural infarctions,2-8 and a pericardial effusion is detectable by
serial echocardiograms in 28% to 63% of patients with
a nonfatal transmural infarction.9-12 Yet the clinically
reported frequency of postinfarction pericarditis
ranges between 7%13 and 41%.1 Such a wide range
seems inconsistent with the narrower frequency range
determined by pathological examination2-8 and serial
echocardiograms.9-12
Assuming that the wide frequency range of clinically
diagnosed postinfarction pericarditis is due to a difference in the clinical definition among various studies,
whereas the pathological and echocardiographic frequencies of postinfarction pericarditis and postinfarction pericardial effusion, respectively, are due to more
precise, objective diagnostic criteria and observations,
the present report reviews the clinical frequency of
postinfarction pericarditis according to its definition
(see below) and compares it with the available pathological and echocardiographic data.
Types of Postinfarction Pericarditis
Between 1936 and 1941, four articles14-'7 emphasized
an 80% to 85% incidence of acute localized - ie, regional-postinfarction pericarditis, in contrast to a 15% to
20% incidence of the diffuse variety. Both types occurred during the first week after an acute myocardial
infarction. In 1956, Dressler18 described a form of
postinfarction pericarditis characterized by prolonged
or recurrent positional pleuritic chest pain, pulmonary
infiltrates, fever, an increased erythrocyte sedimentation rate, and/or a pericardial friction rub. This syndrome usually occurs 2 to 11 weeks after the infarction,19 although occasionally it is recognized during the
first week.'8'20'21 Although some authors22,23 subsequently have questioned the existence of Dressler's
Received February 8, 1994; revision accepted April 18, 1994.
From the Heart Research and Education Association of Colorado, Rose Medical Center, Denver (P.B.O.); the Electrocardiography and Electrophysiology Laboratories, Mayo Clinic and Foundation, Rochester, Minn (S.C.H.); and the Cardiac Graphics
Laboratory, Division of Cardiology, Northwestern Memorial Hospital, Chicago, Ill (J.V.T.).
Correspondence to Philip B. Oliva, MD, Heart Research and
Education Association of Colorado, Rose Medical Center, Cardiology Division, 4567 E Ninth Ave, Denver, CO 80220.
X 1994 American Heart Association, Inc.
syndrome, despite a 12% incidence of postinfarction
heart muscle antibodies,24 general experience has established its incidence as 5%20 or less,21'25 a much lower
incidence than the accepted, consistently earlier form.
Definition of Pericarditis
During the pre-World War II years, when a three- or
four-lead ECG was standard, interest was focused on
the ECG alterations associated with pericarditis.26-34
The diagnosis of pericarditis was based on the presence
of a pericardial friction rub, a pericardial effusion, or
autopsy evidence of pericardial injury.26-34 Symptoms
were not used. Evolutionary changes of the ST segment
and T waves were recognized26-34 and shown to be due
to subepicardial inflammation and/or injury.28-32 It remained for Spodick35 to formally establish the characteristic four phases of repolarization changes due to
pericarditis.
After World War II, a spate of reports36-42 appeared
describing the clinical characteristics of acute rheumatic
or nonspecific pericarditis. These articles emphasized
the importance of recognizing positional pleuritic chest
pain as evidence of pericarditis. Whereas 92% to 100%
of patients with pericarditis had typical chest pain, only
47% to 74% had a pericardial friction rub.36-42
With regard to postinfarction pericarditis, authors of
late 20th-century textbooks on cardiology also advised
avoiding reliance on a friction rub as the sole indicator
of pericarditis. In 1966, Dr Charles K. Friedberg43
stated that "even when no rub is heard a highly probable diagnosis of acute pericarditis can be made on the
basis of the typical pleuropericardial pain." Six years
later he added that positional pleuritic chest pain is
"adequate to diagnose pericarditis whether or not a rub
is audible."44 In 1978, Dr J. Willis Hurst et a145 wrote
that "pericarditis secondary to transmural infarction is
much more common than the 15% incidence customarily quoted (by rub)." Moreover, they noted that if an
"observer demands the presence of a pericardial friction rub," the diagnosis of pericarditis may be "unrecognized in spite of typical pain." Others46 warned that
requiring a friction rub to diagnose postinfarction pericarditis will result in a "gross underestimate" of its
incidence since "many patients have classic symptoms,
but the friction rub does not occur or is missed because
of its fleeting nature." Gersh et all further state that
"pericarditis is possibly the commonest cause of recurring chest pain after admission to the hospital" for an
acute myocardial infarction, but the clinical diagnosis of
1538
Circulation Vol 90, No 3 September 1994
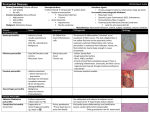
TABLE 1. Relation of Incidence of Postinfarction Pericarditis to Definition of Condition
Definition
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
No. of Cases
With AMI
62
100
145
200
NS
109
41
176
208
NS
779
195
1284
305
338
554
300
1505
400
261
196
80
43
1264
121
423
46
703
No. (%)
With Per
8 (13)
Year
Author
White47
1926
7 (7)
1928
Parkinson and Bedford48
1929
Levine and Brown49
20 (14)
1931
White and Bland50
20 (10)
1935
Master and Jaffe51
2
Blumer14
1936
32 (29)
1936
Vander Veer and Brown52
7 (17)
1938
Bean53
24 (14)
1941
Rosenbaum and Levine54
33 (16)
1968
Wood55
(1 0)
1971
Thadani et a156
52 (7)
1973
22 (11)
Niarchos and McKendrick57
1973
Barman et a158
106 (8.25)
1974
31 (10)
Lichstein et a159
1974
Yan60
41 (10.6)
Toole and Silverman13
1975
40 (7)
1975
Liem et ai61
44 (15)
1975
McLean et a162
224 (14.9)
1976
Guillevin and Valere63 64
64 (16)
1980
38 (14.5)
Sawaya et a165
1981
Hutter et al66
28 (14)
1984
Northcote et a120
23 (28)
1985
12 (28)
Kaplan et a19
1985
Dubois et a167
297 (23.4)
1986
Galve et al10
35 (29)
1985
Krainin et a168
31 (7.3)
Somolinos et alll
1987
19 (41)
Tofier et al69
141 (20)
1989
Oliva et a170
1993
26 (30)
85t
AMI indicates acute myocardial infarction; Peri, postinfarction pericarditis;
*AII five patients with symptoms also had a friction rub.
tExclusive of 1 15 patients who received lytic therapy.
pericarditis is "likely underestimated" because pericardial friction rubs are often evanescent or overlooked or
because the pain may be "attributed to recurrent ischemia." Despite these recommendations by textbook
authors to accept the diagnosis of postinfarction pericarditis if typical symptoms exist without a friction rub,
authors publishing in medical journals have frequently
required a pericardial friction rub to establish the
diagnosis. Table 1 (References 47 through 69) discloses
that all published articles in the English-language literature from 1926 through 1973 based the diagnosis of
postinfarction pericarditis on a rub only. Not until
1974 was an article published that accepted typical
pericardial pain and/or a pericardial friction rub to
diagnose postinfarction pericarditis. From 1974 to
1993, 7 of 14 peer-reviewed articles9-1120,60,62,70 and two
letters to the Editor6364 accepted classic symptoms
and/or a friction rub.
Q-Wave
Non-Q-Wave
AMI, %
AMI, %
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
100
0
100
0
100
0
93
7
NS
NS
70
30
83
17
NS
NS
100
0
86
14
NS
NS
79
21
14
86
91
9
90
10
100
0
70
30
89
11
and NS, not stated.
Rub
NS
Symptoms
NS
+
NS
NS
+
+
+
+
+
+
+
+
+
+
+
+
_
+
5*
+
+
+
+
+
+
If a friction rub alone is used to diagnose postinfarction pericarditis, the mean incidence of this condition
among patients not receiving lytic therapy is 14%. If
classic symptoms or a friction rub or both are used as
diagnostic criteria, the mean incidence rises to 25%
(Table 1). This frequency approximates the autopsyobserved frequency of postinfarction pericarditis of
28% to 40%.2-8
Sensitivity of ECG Criteria for Regional
Postinfarction Pericarditis and Relation of
ECG Criteria to Definition of the Condition
Recently, through an autopsy examination of 70 patients with fatal left ventricular free-wall rupture, we
learned that regional postinfarction pericarditis accompanied rupture in 94% of instances and was consistently
associated with an atypical form of postinfarction
Oliva et al Definition of Postinfarction Pericarditis
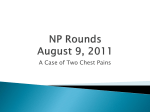
TABLE 2. Effect of Lytic Therapy on Frequency of
Postinfarction Pericarditis
Incidence of Postinfarction
Pericarditis
Non-Lytic Therapy Lytic Therapy
Year
Author
Group, %
Group, %
17
7
Simoons et at75 1985
12
6.4
GISS176
1986
11
ECS77
1988
6.3
7
1990
15
AIMS71
30
Oliva et at74
1993
15
GISSI indicates Gruppo Italiano per lo Studio delta Streptochinasi nett'tnfarto Miocardico; ECS, European Cooperative Study
Group; and AIMS, Anistreplase in Acute Myocardial tnfarction
Study.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
T-wave evolution during the day, or more often several
days, before rupture.71 These T-wave changes were
similar to those recorded in dogs with localized postinfarction pericarditis in 1939.72 Two types of atypical
T-wave evolution were observed clinically. Either the T
waves remained persistently positive for 48 hours or
longer after the onset of an acute myocardial infarction
(type I), or initially inverted T waves gradually became
positive deflections (type II). The sensitivity and specificity, as defined previously, of these atypical T-wave
changes were 100% and 77%, respectively.70 The specificity rose to 96% if patients who had reinfarction,
underwent cardiopulmonary resuscitation, or sustained
a very small initial infarct as a consequence of early lytic
therapy were excluded. The frequency of postinfarction
pericarditis defined by classic symptoms and/or a rub
was 30% in those patients who did not receive lytic
therapy. There was a 2.5% frequency of unexplained
atypical T-wave evolution ("false-positives"). One explanation for this 2.5% incidence of false-positives is
that those patients may have had painless and acoustically silent postinfarction pericarditis. If so, the actual
incidence of postinfarction pericarditis would be 32.5%
in patients not receiving lytic therapy, in harmony with
the autopsy range of 28% to 40%.
The sensitivity of these ECG alterations for postinfarction pericarditis was recently confirmed by an investigation performed at Northwestern University.73 We
reviewed the serial ECGs of all patients from that
institution with clinically recognized (by typical positional pleuritic chest pain and/or a friction rub) postinfarction pericarditis reported by Kaplan et al.9 All
patients had one of the two types of atypical T-wave
evolution,73 affirming the 100% sensitivity of these ECG
changes to diagnose postinfarction pericarditis and also
justifying the use of typical symptoms and/or a friction
rub to diagnose this condition.
Effect of Lytic Therapy on the Incidence of
Postinfarction Pericarditis
Since 1985, five reports74-78 have addressed the effect
of lytic therapy on the incidence of postinfarction
pericarditis (Table 2). All agree that the incidence is
halved by lytic therapy, whether typical symptoms
and/or a friction rub or a rub alone is used to define
postinfarction pericarditis. We found that the incidence
1539
of postinfarction pericarditis as defined by typical symptoms and/or a rub was reduced from 30% to 15% by
lytic therapy.74 Other reports75-78 using a rub alone
found an incidence reduction from between 11% and
17% without lytic therapy to between 6% and 7% with
lytic therapy. The absolute numbers are, of course,
lower when a rub alone is used to define postinfarction
pericarditis, for reasons discussed earlier. However,
regardless of the definition, a 50% reduction of the
incidence of postinfarction pericarditis by lytic therapy
is observed.
Conclusions
Postinfarction pericarditis can be diagnosed when an
accurate history is elicited by an informed cardiologist
from an observant, articulate. patient. The requirement
of a friction rub leads to a significant underestimation of
the incidence of postinfarction pericarditis. Postinfarction pericarditis occurs in an average of 25% of instances of acute transmural myocardial infarction not
treated with lytic therapy when typical symptoms and a
pericardial friction rub are accepted as indicative of
pericarditis, whereas the average incidence is only 14%
when a friction rub alone is required.
Atypical T-wave evolution appears to be a very
sensitive and reasonably specific ECG sign of regional
postinfarction pericarditis. It is more sensitive than a
friction rub and, when observed in a patient with chest
pain after an acute myocardial infarction, provides an
objective method of differentiating among the three
causes of postinfarction chest pain.
Lytic therapy reduces the frequency of postinfarction
pericarditis by 50% whether classic symptoms and a
friction rub or a rub alone is used to define the
condition. Since postinfarction pericarditis is almost
always the consequence of a transmural infarction,7879
its reduction by lytic therapy implies sparing of the
pericardium and subjacent myocardium.
Acknowledgments
This work was supported, in part, by research grants from
the Rose Medical Foundation, Denver, Colo, and Marquette
Electronics, Inc, Milwaukee, Wis. The assistance of Marty
Bender at the Heart Research and Education Association of
Colorado, Marlene Ploetz at the Mayo Clinic, and Sharon
Baruch and Michell Parker, RN, at Northwestern University is
appreciated.
References
1. Gersh BJ, Chesebro JH, Clements JP. In: Giuliana EP, Fuster VJ,
Gersh BJ, McGoon MD, eds. Cardiology Fundamentals and
Practice. St Louis, Mo: Mosby Year Book Inc; 1991:1423.
2. Appelbaum E, Nicolson GHB. Occlusive disease of the coronary
arteries: an analysis of the pathologic anatomy in one hundred
sixty-eight cases, with electrocardiographic correlation in thirty-six
of these. Am Heart J. 1934-35;10:662-680.
3. Bean WB. Infarction of the heart, III: clinical course and morphologic findings. Ann Intern Med. 1938;12:71-94.
4. Wang CH, Bland EF, White PD. A note on coronary occlusion and
myocardial infarction found postmortem at the Massachusetts
General Hospital during the twenty year period from 1926 to 1945
inclusive. Ann Intern Med. 1948;29:601-606.
5. Wartman WB, Hellerstein HK. The incidence of heart disease in
2000 consecutive autopsies. Ann Intern Med. 1948;28:41-65.
6. Achor RWP, Futch WD, Burchell HB, Edwards JE. The fate of
patients surviving acute myocardial infarction: a study of clinical
and necropsy data in two hundred fifty cases. Arch Intern Med.
1956;98:162-174.
1540
Circulation Vol 90, No 3 September 1994
7. Erhardt LR. Clinical and pathological observations in different
types of acute myocardial infarction. Acta Med Scand (suppl 560).
1974:59-67.
8. Roeske WR, Savage RM, O'Rourke RA, Bloor CM. Clinicopathologic correlations in patients after myocardial infarction.
Circulation. 1981;63:36-45.
Kaplan K, Davison R, Parker M, Przybylek J, Light A, Bresnahan
D, Ribner H, Talano JV. Frequency of pericardial effusion as
determined by M-mode echocardiography in acute myocardial
infarction. Am J Cardiol. 1985;55:335-337.
10. Galve E, Garcia-del-Castillo H, Evangelista A, Batlle J, PermanyerMiralda G, Soler-Soler J. Pericardial effusion in the course of myocardial infarction: incidence, natural history, and clinical relevance.
9.
Ciwrulation. 1986;73:294-299.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
11. Somolinos M, Violan S, Sanz R, Marrero P. Early pericarditis after
acute myocardial infarction: a clinical echocardiographic study.
Crit Care Med. 1987;15:648-651.
12. Pierard LA, Albert A, Henrard L, Lempereur P, Sprynger M,
Carlier J, Kulbertus HE. Incidence and significance of pericardial
effusion in acute myocardial infarction as determined by twodimensional echocardiography. JAm Coll Cardiol. 1988;8:517-520.
13. Toole JC, Silverman ME. Pericarditis of acute myocardial
infarction. Chest. 1975;67:647-653.
14. Blumer G. Pericarditis epistenocardica. JAMA. 1936;107:178-181.
15. White PD. Heart Disease. New York, NY: MacMillan Publishing
Co; 1937:463.
16. Stewart CF, Turner KB. A note on pericardial involvement in
coronary thrombosis. Am Heart J. 1938;15:232-234.
17. Langendorf R. The effect of diffuse pericarditis on the electrocardiographic pattern of recent myocardial infarction. Am Heart J.
1941;22:86-104.
18. Dressier W. A post-myocardial infarction syndrome: preliminary
report of a complication resembling idiopathic, recurrent, benign
pericarditis. JAMA. 1956;160:1379-1383.
19. Dressler W. The post-myocardial-infarction syndrome: a report of
forty-four cases. Arch Intern Med. 1959;103:28-41.
20. Northcote RJ, Hutchison SJ, McGuinnes JB. Evidence for the
continued existence of the postmyocardial infarction (Dressler's)
syndrome. Am J Cardiol. 1984;53:1201-1202.
21. Davidson C, Oliver MF, Robertson RF. Post-myocardial-infarction
syndrome. Br Med J. 1961;2:535-539.
22. Kossowsky WA, Lyon AF, Spain DM. Reappraisal of the post
myocardial infarction (Dressler's) syndrome. Am Heart J. 1981;102:
954-956.
23. Lichstein E, Arsura E, Hollander G, Greengart A, Sanders M.
Current incidence of postmyocardial infarction (Dressler's)
syndrome. Am J Cardiol. 1982;50:1269-1271.
24. Liem KL, ten Veen H, Lie KI, Feltkamp TEW, Durrer D.
Incidence and significance of heart muscle antibodies in patients
with acute myocardial infarction and unstable angina. Acta Med
Scand. 1979;206:473-475.
25. Welin L, Vedin A, Wilhelmsson C. Characteristics, prevalence,
and prognosis of postmyocardial infarction syndrome. Br Heart J.
1983;50:140-145.
26. Scott RW, Feil HS, Katz LN. The electrocardiogram in pericardial
effusion, I: clinical. Am Heart J. 1929;5:68-76.
27. Katz LN, Feil HS, Scott RW. The electrocardiogram in pericardial
effusion, II: experimental. Am Heart J. 1929;5:77-83.
28. Harvey J, Scott JW. Changes in the electrocardiogram of pericardial effusion with paracentesis and pericardiotomy. Am Heart J.
1932;7:532-535.
G, Schwab EH. Some experimental and clinical electrocardiographic observations on R-S-T and T changes in pericarditis. Trans Assoc Am Physicians. 1934;49:229-243.
Schwab EH, Herrmann G. Alterations of the electrocardiogram in
diseases of the pericardium. Arch Intern Med. 1935;55:917-941.
Vander Veer JB, Norris RF. The electrocardiographic changes in
acute pericarditis: a clinical and pathological study. Am Heart J.
1938;4:31-50.
Winternitz M, Langendorf R. The electrocardiogram in pericarditis. Acta Med Scand. 1938;94:141-188.
Bellet S, McMillan TM. Electrocardiographic patterns in acute
pericarditis: evolution, causes and diagnostic significance of
patterns in limb and chest leads: a study of fifty-seven cases. Arch
Intern Med. 1938;61:381-400.
Noth PH, Barnes AR. Electrocardiographic changes associated
with pericarditis. Arch Intern Med. 1940;63:291-320.
29. Herrmann
30.
31.
32.
33.
34.
35. Spodick DH. Acute Pericarditis. New York/London: Grune &
Stratton; 1959:18-19.
36. Nay RM, Boyer NH. Acute pericarditis in young adults. Am Heart
J. 1946;32:222-233.
37. Burchell HB. Acute nonspecific pericarditis. Mod Concepts Cardiovasc Dis. 1947;16:no. 3.
38. Logue RB, Wendkos MH. Acute pericarditis of benign type. Am
Heart J. 1948;36:587-599.
39. Levy RL, Patterson MC. Acute serofibrinous pericarditis of undetermined cause. Am J Med. 1950;3:34- 45.
40. Carmichael DB, Sprague HB, Wyman SM, Bland EF. Acute nonspecific pericarditis: clinical, laboratory and follow-up considerations. Circulation. 1951;3:321-331.
41. Gilley EW, McCord MC, Taguchi JT. Acute nonspecific pericarditis. Am J Med Sci. 1951;222:249-256.
42. McGuire J, Kotte JH, Helm RA. Clinical progress: acute pericarditis. Circulation. 1954;9:425-442.
43. Friedberg CK. Acute pericarditis. In: Friedberg CK, ed. Disease of
the Heart. Philadelphia/London: WB Saunders Co; 1966:1945.
44. Friedberg CK. Symposium: Myocardial Infarction, 1972 (pt I).
Circulation. 1972;45:179-188.
45. Hurst JW, Logue RB, Walter PH. The clinical recognition and
management of atherosclerotic heart disease. In: Hurst JW, Logue
RB, Schlant RC, Wenger NK, eds. The Heart. New York, NY:
McGraw-Hill Book Co; 1978:1205.
46. Darsee JR, Braunwald E. In: Braunwald E, ed. Heart Disease: A
Textbook of Cardiovascular Medicine. Philadelphia, Pa: WB
Sanders Co; 1980:1558.
47. White PD. The prognosis of angina pectoris and coronary
thrombosis. JAMA. 1926;87:1525-1530.
48. Parkinson J, Bedford DR. Cardiac infarction and coronary
thrombosis. Lancet. 1928;1:4-11.
49. Levine SA, Brown CL. Coronary thrombosis: its various clinical
features. Medicine. 1929;8:245-413.
50. White PD, Bland EF. A further report on the prognosis of angina
pectoris and of coronary thrombosis: a study of five hundred cases
of the former condition and of two hundred cases of the latter. Am
Heart J. 1931;7:1-14.
51. Master AM, Jaffe HL. Coronary arterial thrombosis with pericardial effusion. JAMA. 1935;104:1212-1214.
52. Vander Veer JB, Brown LE. The diagnosis and prognosis of
coronary occlusion: the electrocardiogram as an aid. Penn Med J.
1936;39:303-309.
53. Bean WB. Infarction of the heart, II: symptomatology of acute
attack. Ann Intern Med. 1938;11:2086-2108.
54. Rosenbaum FF, Levine SA. Prognostic value of various clinical and
electrocardiographic features of acute myocardial infarction, I:
immediate prognosis. Arch Intern Med. 1941;68:913-944.
55. Wood P. Disease of the Heart. London, UK: Eyre and Spottiswoode; 1968:859.
56. Thadani U, Chopra MP, Aber CP, Portal RW. Pericarditis after
acute myocardial infarction. Br Med J. 1971;2:135-137.
57. Niarchos AP, McKendrick CS. Prognosis of pericarditis after acute
myocardial infarction. Br Heart J. 1973;35:49-54.
58. Barman PC, Krishnaswam V, Gerac AR. Pericarditis in acute
myocardial infarction. N Y State J Med. 1973;72:645-648.
59. Lichstein E, Liu H, Gupta P. Pericarditis complicating acute myocardial infarction: incidence of complications and significance of
electrocardiogram on admission. Am Heart J. 1974;87:246-252.
60. Yan V. Pericarditis in acute myocardial infarction. Heart Lung.
1974;3:247-251.
61. Liem KL, Durrer D, Lie KI, Wellens HJJ. Pericarditis of acute
myocardial infarction. Lancet. 1975;2:1004-1006.
62. McLean KH, Bett JHN, Saltups A. Pericarditis in acute myocardial infarction. Aust N Z J Med. 1975;5:1-2.
63. Guillevin L, Valere PE. Pericarditis in acute myocardial infarction.
Lancet. 1976;1:429. Letter.
64. Guillevin L, Valere PE. Infarction-associated pericarditis. N Engl J
Med. 1985;312:548. Letter.
65. Sawaya JI, Mujais SK, Armenian HK. Early diagnosis of pericarditis in acute myocardial infarction. Am Heart J. 1980;100:
144-151.
66. Hutter AM, DeSanctis R, Flynn T, Yeatman LA. Nontransmural
myocardial infarction: a comparison of hospital and late clinical
course of patients with that of matched patients with transmural
anterior and transmural inferior myocardial infarction. Am J
Cardiol. 1981;48:595-602.
67. DuBois C, Smeets JP, DeMoulin JC, Pierard LA, Henrard L,
Kulbertus HE. Frequency and clinical significance of pericardial
friction rub in the acute phase of myocardial infarction. Eur J
Cardiol. 1986;6:766-768.
Oliva et al Definition of Postinfarction Pericarditis
68. Krainin FM, Flessas AP, Spodick DH. Infarction-associated pericarditis. Rarity of diagnostic electrocardiogram. N Engl J Med.
1985;311:1211-1214.
69. Tofler GH, Muller JE, Stone PH, Willich SN, Davis VG, et al.
Pericarditis in acute myocardial infarction: characterization and
clinical significance. Am Heart J. 1989;117:86-90.
70. Oliva PB, Hammill SC, Edwards WD. Electrocardiographic
diagnosis of postinfarction regional pericarditis: ancillary observations regarding the effect of reperfusion on the rapidity and
amplitude of T wave inversion after acute myocardial infarction.
Circulation. 1993;88:896-904.
71. Oliva PB, Hammill SC, Edwards WD. Cardiac rupture: a clinically
predictable complication of acute myocardial infarction: a report
of 70 cases with clinical-pathological correlations. J Am Coll
Cardiol. 1993;22:720-726.
72. Burchell HB, Barnes AR, Mann FC. The electrocardiographic
picture of experimental localized pericarditis. Am Heart J. 1939;
18:133-144.
73. Oliva PB, Hammill SC, Talano JV. T wave changes consistent with
epicardial involvement in acute myocardial infarction: observations in patients with a postinfarction pericardial effusion
without clinically recognized postinfarction pericarditis. JAm Coll
Cardiol. In press.
1541
74. Oliva PB, Hammill SC. The clinical distinction between postinfarction regional pericarditis and other causes of postinfarction
chest pain: ancillary observations regarding the effect of lytic
therapy upon the frequency of postinfarction pericarditis, postinfarction angina and reinfarction. Clin CardioL In press.
75. Simoons ML, Brand MVD, de Zwaan C, Verheught FWA, Remme
WJ, Serruys PW, Bar F, Res J, Krauss XH, Vermeer F, Lubsen J.
Improved survival after early thrombolysis in acute myocardial
infarction: a randomized trial by the Interuniversity Cardiology
Institute in the Netherlands. Lancet. 1985;2:578-582.
76. Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto
Miocardico (GISSI). Effectiveness of intravenous streptokinase
thrombolytic treatment in acute myocardial infarction. Lancet.
1986;1:397-402.
77. Van de Werf F and the European Cooperative Study Group. Lessons
from the European Cooperative Recombinant Tissue-Type Plasminogen Activator (rt-PA) Versus Placebo Trial. JAm Coil Cardiol.
1988;12:14A-19A.
78. AIMS Trial Study Group. Long-term effects of intravenous anistreplase in acute myocardial infarction: final report of the AIMS
study. Lancet. 1990;335:427-431.
79. Spodick DH. Pericarditis in acute myocardial infarction. Am Heart
J. 1989;118:1354-1355. Letter.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Effect of definition on incidence of postinfarction pericarditis. It is time to redefine
postinfarction pericarditis?
P B Oliva, S C Hammill and J V Talano
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Circulation. 1994;90:1537-1541
doi: 10.1161/01.CIR.90.3.1537
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1994 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circ.ahajournals.org/content/90/3/1537.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located,
click Request Permissions in the middle column of the Web page under Services. Further information about
this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/