Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
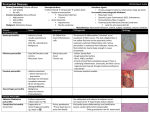
Acute Pericarditis Incidence – Post mortem 1-6%, diagnosed in only 0.1% of hospitalized patients. 5% of patients seen in emergency rooms with CP and no MI. Sequelae – Cardiac tamponade Recurrent pericarditis Pericardial constriction Etiology Viral or idiopathic After MI Infectious diseases With dissecting aortic aneurysms Trauma Metastasis XRT Uremia After cardiac or other thoracic surgery Autoimmune diseases Medications Clinical Presentation History Physical Exam- 85% have audible friction rub during the course of their disease ( the rub is high pitched scratchy or squeaky sound best heard at the left sternal border at end of expiration with the patient leaning forward) The rub has three components- atrial systole, ventricular systole and rapid ventricular filling during early diastole. Evaluation A diagnosis of acute pericarditis should be reserved for patients with an audible pericardial friction rub or CP with typical EKG findings, most notably ST- segment elevation. EKG Stages of pericarditis: I- Diffuse ST elevation and PR segment depression (seen in more than 80%) II- Normalization of the ST and PR III- Widespread T- wave inversions IV- Normalization of the T waves The most reliable distinguishing feature may be the ratio of ST segment elevation (in millimeters) to T-wave amplitude in lead V6; ratio > 0.24 Cardiac Tamponade Clinical Findings Systemic arterial hypotension Tachycardia Elevated JVP Pulsus paradoxus (most sensitive but not specific) 15% of patients with idiopathic pericarditis or as many as 60% of those with neoplastic, tuberculous, or purulent pericarditis can present with Cardiac Tamponade. Echo Findings in Pre-Tamponade Physiology Diastolic right ventricular collapse Right atrial collapse/inversion Exagerated respiratory variation in inflow velocity Exagerated respiratory variation in inferior vena cava flow Dilated IVC in the right setting Echo-Guided Pericardiocentesis Multiple Echo windows should be used to determine the distribution of the fluid. Specifically, the distribution and depth from the surface of the chest at which contact with the fluid is anticipated by the pericardiocentesis needle should be determined. If the location of a pericardiocentesis needle is in question, agitated saline can be injected to further define the location of the tip. Differential Diagnosis Pericarditis Clinical presentation should guide the ordering of additional tests. Routine serologic testing, including testing for ANA and RF, reveals a source for the pericarditis for only 10-15% of patients. Plasma troponin concentrations are elevated in 35-50% of patients with pericarditis. The magnitude of the ST elevation appears to correlate with magnitude of troponin elevation. A troponin elevation lasting more than 2 weeks, suggests associated myocarditis. Pericardiocentesis and Biopsy In those with pericardial tamponade and in those with known or suspected purulent or neoplastic pericarditis. In a study involving 230 patients with acute pericarditis in whom the cause was unknown, pericardiocentesis and pericardial biopsy provided a diagnosis in only 6% and 5% respectively. Laboratory Evaluation Red and white cell count. Cytology TG CTX No evidence for PH, glucose, LDH and protein measurement. PCR > 30 U/L for adenosine deaminase activity may help in identifying MTB Treatment In observational studies, NSAIDS relieved CP in 85-90% of patients: ASA, Indomethacin or Ibuprofen. Indomethacin may impair coronary blood flow in CAD. In a multicenter trial of 51 patients who had recurrent pericarditis despite tx with NSAIDS, glucocorticoids, pericardiocentesis or some combination. Only 7 of those treated with colchicine had a recurrence during 1004 patientmonths of follow up. Sauleda Treatment Typically CP improves within days of initiating antinflammatory tx. • If CP persists after two weeks of tx with an NSAID, a different NSAID should be given or colchicine should be added to provide combination therapy. • Glucocorticoids should be considered if CP persists after combination tx. • Lack of response to steroids often reflects the use of an inadequate dose or too rapid tapering. Treatment Several indicators of poor prognosis: >38*C Subacute onset Immunosuppressed After trauma Anticoagulation use Myopericarditis Large effusion or tamponade Treatment Use of steroids should be reserved for patients with CTD, recurrent severe pericarditis that is unresponsive to combination of NSAIDS and colchicine. Some studies suggest that the early use of these drugs may increase the risk of recurrence (exception colchicine). Observational data suggest that physical invasion of the pericardium (pericardiotomy or a window) promotes recurrences. Effusive Constrictive Pericarditis Is a clinical hemodynamic syndrome in which constriction of the heart by the visceral pericardium occurs in the presence of tense effusion in a free pericardial space. The hallmark is the persistence of elevated right atrial pressure after intrapericardial pressure has been reduced to normal levels by removal of pericardial fluid.