Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
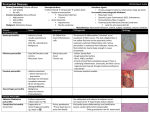
General Medical Officer (GMO) Manual: Clinical Section Pericarditis Department of the Navy Bureau of Medicine and Surgery Peer Review Status: Internally Peer Reviewed (1) Introduction Acute pericarditis, caused by inflammation of the pericardium, manifests as chest pain, a pericardial friction rub, and has serial electrocardiogram (ECG) abnormalities. The incidence is 1/1000 hospital admissions. At autopsy, changes of pericarditis appear in 2 to 6 percent of cases. The majority of cases are idiopathic or postviral, but acute myocardial infarction, uremia, bacterial infection, tuberculosis, collagen-vascular disease, neoplasm, and trauma must be considered. (2) Symptoms suggestive of pericarditis Pericarditis chest pain occurs in the pericardium with a pleuritic component. Recumbency increases the pain, which often radiates to the trapezius ridge. Swallowing may exacerbate pain. Dyspnea results from pleural irritation or, on occasion, accumulation of a large pericardial effusion. Symptoms typically occur with an ongoing or preceding upper respiratory infection. Exertion may exacerbate chest pain, but the pleuritic nature and positional component persist. When pericarditis follows myocardial infarction, ischemic chest pain precedes. Coexistent symptoms of pneumonitis suggest a bacterial etiology, especially with high fever. Recurrent fevers, sweats, and weight loss suggest tuberculosis. Malignant pericarditis is usually metastatic with other clinical evidence of malignancy. Common primary tumors include lung, breast, melanoma, lymphoma, and leukemia. (3) Physical exam findings Physical examination includes a careful assessment of vital signs with determination of pulsus paradoxicus. Neck vein distension, distant heart tones, and poor peripheral perfusion suggest cardiac tamponade, especially with a pulsus paradoxicus of greater than 10 mm Hg. Lung auscultation may show signs of consolidation. Cardiac auscultation provides the important, but often evanescent, pericardial friction rub, which may be of one, two, or three components. The complete blood count (CBC), which is usually normal, may indicate an infection or leukemia. An erythrocyte sedimentation rate (ESR) is often elevated; a nonspecific finding. A tuberculin test, PPD (purified protein derivative), should be applied to patients who have not been previously reactive. The chest x-ray is usually normal, but may include evidence of pneumonitis, tumor, or cardiomegaly suggesting pericardial effusion. Electrocardiogram (ECG) ECG diagnosis of pericarditis depends on serial changes from a current injury caused by superficial myocardial inflammation or epicardial injury. Four stages are described. Stage I occurs with the onset of chest pain. ST segment elevations are concave upward and usually noted in all leads except AVR and V1. Stage II, seen several days later, shows return of ST segments to baseline with T flattening. T inversion is seen in stage III, without loss of R voltage or new Qs. In stage IV, weeks to months later, Ts revert to normal. Atypical ECG patterns occur in up to 50 percent of patients and prompt careful consideration of an ischemic etiology, especially with an atypical history or the absence of a pericardial friction rub. (4) Differential diagnosis of pericarditis (a) (b) (c) (d) (e) pneumonitis pulmonary embolism myocardial infarction herpes zoster chest tumors (f) mechanical chest wall pain (g) reflux esophagitis (h) diaphragmatic irritation from an abdominal process (5) Management considerations In port, patients with acute pericarditis should be admitted to a hospital. In rare cases, mild illness may be handled as an outpatient with close follow up by an internist. At sea, patients with a typical history, physical, and ECG findings of postviral or idiopathic pericarditis may be treated and closely observed in sick bay. Significant improvement is expected in 1 to 2 days. Dysrhythmias and hemodynamic complications are rare. Patients should be referred to a specialist upon arrival in port, even if asymptomatic. They should rest until asymptomatic and should not return to duty until full evaluation is completed. Patients with atypical presentations, especially if ischemia, tuberculosis bacterial infection, or suspected tumor, should be expeditiously transferred to a tertiary care facility. Hemodynamic compromise demands rapid evaluation. Pericardiocentesis may be required. (6) Treatment Acute pericarditis responds well to rest and nonsteroidal anti-inflammatory treatment. Most physicians prefer ibuprofen, 400-800 mg orally TID or QID. In mild cases, aspirin may be used, 650 mg PO QID. In the past, indomethacin was used, but caused more gastric irritation. Prednisone has proven effective in difficult cases, but is frequently associated with recurrence. Colchicine 0.6 mg BID has been effective in treating recurrent pericarditis. For a discussion of pericardiocentesis, see the American Heart Association’s Advanced Cardiac Life Support (ACLS) Manual. The severity of illness, suspected etiology, and firmness of diagnosis dictate the disposition and urgency of disposition. Ischemia or hemodynamic compromise mandate emergent transfer. Overt infection similarly requires emergency culture, treatment, and transfer. Suspicion of malignancy or infection dictates urgent referral. Timely communication with a specialist provides helpful, case-specific assistance. Reference (a) Permanyer-Miralda G, Sagrista Sauleda J, and Soler-Soler J. Primary Acute Pericardial Disease: A Prospective Series of 231 Consecutive Patients. AM J Cardiol 1985; 56 623-630. Reviewed by CAPT K. F. Strosahl, MC, USN, Cardiology/Computer Assisted Program of Cardiology Specialty Leader, Cardiovascular Disease Division, Portsmouth Naval Hospital, Portsmouth, VA (1999).