Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Artificial heart valve wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Aortic stenosis wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Atrial septal defect wikipedia , lookup
Congenital heart defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
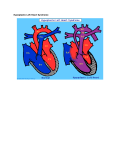
Hypoplastic Left Heart Syndrome: Diagnosis and Early Management Frederick Jay Fricker NeoReviews 2008;9;e253-e259 DOI: 10.1542/neo.9-6-e253 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://neoreviews.aappublications.org/cgi/content/full/neoreviews;9/6/e253 NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication, it has been published continuously since 2000. NeoReviews is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2008 by the American Academy of Pediatrics. All rights reserved. Online ISSN: 1526-9906. Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 Article cardiology Hypoplastic Left Heart Syndrome: Diagnosis and Early Management Frederick Jay Fricker, MD* Author Disclosure Dr Fricker has disclosed no financial Objectives After completing this article, readers should be able to: 1. Describe the morphology of hypoplastic left heart syndrome (HLHS). 2. Recognize clinical findings suggestive of patent ductus arteriosus-dependent systemic blood flow. 3. Delineate initial postnatal management of HLHS. 4. Describe surgical palliation of HLHS. relationships relevant to this article. This commentary does not contain a discussion of an unapproved/ investigative use of a commercial product/device. Abstract Hypoplastic left heart syndrome (HLHS) is the only congenital heart lesion that requires the talents of the neonatologist, pediatric cardiologist, and cardiovascular surgeon operating and communicating as a team to effect the desired outcome of survival with normal neurodevelopment. Prenatal diagnosis, initial resuscitation, and preoperative management are key elements that allow the best opportunity for low surgical morbidity and mortality in the affected infant. Physicians and nurses caring for such infants must understand the physiology of oxygen delivery and the response of the neonatal pulmonary and systemic vascular bed to interventions that affect the balance between systemic and pulmonary blood flow. Outcomes with current surgical management, including the Norwood procedure and the Sano modification, are equivalent to those associated with the arterial switch procedure and repair of neonatal tetralogy of Fallot. Families of infants born with HLHS should be encouraged by the current results of palliation and long-term outcome. Introduction HLHS is a common, potentially lethal congenital heart defect that accounts for a significant proportion of infant mortality from congenital heart disease in the first year after birth. This defect has morphologic variability and accounts for 7% to 9% of all infants born with congenital heart defects. Noonan and Nadas coined the term “hypoplastic left heart syndrome” in 1958, but Lev described the defect nearly a decade earlier. The defect was uniformly fatal until 25 years ago, when Norwood performed the first successful palliative procedure. A number of earlier palliation attempts involved establishing stable systemic blood flow and restricting pulmonary blood flow, but it was Norwood who persisted and reported the first survival in early 1980. Surgical modifications by the recent generation of pediatric congenital heart surgeons have resulted in excellent early survival after the first-stage Norwood procedure. Paramount to surgical success are early diagnosis and preoperative management strategies of the neonatologist and pediatric cardiologist. This review emphasizes findings that create suspicion that an infant has ductus arteriosusdependent systemic blood flow and highlights strategies to balance systemic and pulmonary blood flow until surgery is accomplished. Morphology The anatomic features of infants who have HLHS vary, but hypoplasia of the left ventricle is a consistent finding. The classic phenotype is left ventricular hypoplasia associated with mitral stenosis/atresia, aortic atresia, coarctation of the aorta, and an intact ventricular septum (Figs. 1, 2, and 3). Variations include common atrioventricular septal defect with *Chief of Pediatric Cardiology, University of Florida, Gainesville, Fla. NeoReviews Vol.9 No.6 June 2008 e253 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology hypoplastic left heart disease Figure 1. A cross-section of a heart specimen demonstrating the key features of hypoplasia of the left heart, including aortic atresia (A), mitral valve stenosis (MV), and large right heart. TVⴝtricuspid valve, PAⴝpulmonary valve, coronary arteriesⴝarrows. a dominant right ventricle and hypoplasia of the left ventricle. The ascending aorta and aortic arch have varying degrees of stenosis and hypoplasia (Fig. 3). The ascending aorta size is a risk factor for surgical palliation. Aortic atresia with less than 2 mm ascending aorta make reconstruction of the ascending aorta vulnerable to cor- Figure 3. Specimen demonstrating aortic atresia with tiny ascending aorta (Ao) and the presence of discrete coarctation (arrow) related to insertion of the ductus arteriosus. AAⴝaortic arch, DAⴝdescending aorta, PDAⴝpatent ductus arteriosus, RAⴝright atrium. onary artery obstruction because the ascending aorta is the only gateway to the coronary circulation (Fig. 1). Hypoplasia of the transverse aortic arch and isthmus always is present, with an associated discrete coarctation Figure 2. Heart specimens with degrees of left heart hypoplasia. Note the increased mass and small cavity of specimen A. In specimen B, the right ventricle (RV) is large and apex-forming. Note the small mitral valve and left ventricular (LV) cavity size. e254 NeoReviews Vol.9 No.6 June 2008 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology hypoplastic left heart disease (Fig. 3). An unrestricted interatrial communication is critical to survival. If interatrial communication is intact or restrictive, the infant will be in extremis shortly after birth unless the left atrium is decompressed through the levocardial vein (remnant of the left superior vena cava) or through coronary artery sinusoids from the left ventricle to the coronary sinus. The right ventricle and tricuspid valve represent the systemic ventricle and atrioventricular valve, and their functional status determines the approach to palliation. Diagnosis Neonatologists and pediatric cardiologists have witnessed the cardiovascular collapse of an infant who has patent ductus arteriosus (PDA)-dependent systemic blood flow. Recovery of end-organ function from the insult of severe metabolic acidosis and hypoxemia is, at best, slow and uncertain. Identifying affected infants in a newborn nursery can be challenging because the ductus arteriosus remains patent early after birth. Even though infants have complete admixture of systemic and pulmonary venous return, pulmonary blood flow relative to marginal systemic blood flow is increased, resulting in oxygen saturation greater than 85%. Cyanosis is difficult to recognize at this level. However, certain clues can increase suspicion of the presence of a critical heart lesion. Hyperdynamic precordial activity is a consistent finding that reflects right ventricular volume and pressure overload. Decrease in amplitude of peripheral pulses often is cited but is only evident after ductal constriction in a symptomatic infant. The second heart sound is single if aortic atresia is present. A heart murmur of tricuspid valve regurgitation or increased pulmonary blood flow may be audible. Newborn screening with pulse oximetry has been advocated. Oxygen saturations rarely are greater than 85% to 88% in affected infants, and decreased saturation is an indication for cardiology evaluation with echocardiography. Oxygen saturation screening should be undertaken in both the right arm (preductal saturation) and leg (postductal saturation). Electrocardiography (ECG) and chest radiography are not adequate ancillary screening methods if the neonatologist suspects a serious congenital heart lesion. Prenatal diagnosis avoids the early diagnostic and management problems incurred by affected infants and optimizes their outcome. Initial Postnatal Management The initial management of infants who have HLHs physiology focuses on safe transport and hemodynamic and respiratory stabilization. The principal goal is to return Figure 4. Anatomic heart specimen of aortic atresia demonstrating the course of blood flow from the main pulmonary artery (PA) through the patent ductus arteriosus (PDA) retrograde into the tiny ascending aorta (double arrows), DAⴝdescending aorta, RAⴝright atrium. the infant to the intrauterine state. Re-establishment of PDA patency and securing the airway is the priority to re-establish systemic blood flow (Fig. 4). Prostaglandin E1 (PGE1) is administered at 0.05 to 0.1 mcg/kg per minute. Because PGE1 can cause apnea initially, the neonatologist and transport physician should take precautions to secure the airway before transport. Balancing systemic and pulmonary blood flow to optimize peripheral organ perfusion and function is paramount for successful transition to surgery. PGE1 can decrease both pulmonary (PVR) and systemic vascular resistance (SVR); oxygen administration decreases PVR and increases SVR. Although oxygen administration while preparing the infant for surgery is potentially detrimental, administration during the resuscitation, stabilization, and transport period can be beneficial. Maintaining oxygen delivery to tissues can be approached by either decreasing SVR through use of inodilators such as milrinone or increasing PVR by manipulating the ambient oxygen environment by controlled hypoxia (FiO2 of NeoReviews Vol.9 No.6 June 2008 e255 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology hypoplastic left heart disease infant who has HLHS is necessary for survival. Restrictive interatrial communication is analogous to pulmonary venous obstruction because there is no exit from the left atrium. Pulmonary venous obstruction results in pulmonary edema, decreased lung compliance, and hypoxemia. Attempted high-risk interventional septostomy in the catheterization laboratory can be considered. Urgent surgery in this clinical setting rarely has a successful outcome. 100% 85% 75% Oxygen Saturation 50% 1:1 2:1 3:1 Qp/Qs Pulmonary blood/Systemic blood flow Figure 5. Effect of increasing oxygen saturation on the ratio of pulmonary blood flow to systemic blood flow. 17% to 20%) or by hypoventilation resulting in hypercarbia. Milrinone is both an inotropic drug and an effective systemic vasodilator agent (phosphodiesterase inhibitor) that is used in the preoperative management of infants who have HLHS. One other point should be emphasized regarding oxygen administration. The diagnosis should be confirmed before discontinuing oxygen because a missed diagnosis of persistent pulmonary hypertension of the newborn is lethal. The relationship between pulmonary blood flow and systemic blood flow is assessed by clinical examination and oxygen saturation/arterial blood gas determinations. The oxygen saturation trend is key to day-to-day management and to evaluating an acute change in the infant’s clinical condition. Because HLHS is a complete admixture lesion (complete mixing of systemic and pulmonary venous return), the relative pulmonary blood flow (QP)-to-systemic blood flow (QS) ratio is determined by assessing changes in systemic oxygen saturation through pulse oximetry or arterial blood gas changes. A balanced QP/QS saturation is 75% QP/QS 1:1. Because PVR is lower than SVR, the oxygen saturation for infant who has HLHS in a stable balanced hemodynamic state should range from 75% to 85%. As PVR decreases and the QP/QS ratio increases, the oxygen saturation/ arterial PO2 increases (Fig. 5). If PGE1 administration is interrupted and the ductus arteriosus constricts, QS relative to QP decreases, a marked increase in oxygen saturation and arterial PO2 occurs, and metabolic acidosis develops. Oxygen saturation falling below 70% should raise concern about lung atelectasis or restriction of the interatrial communication causing a decrease in QP relative to QS. Communication at the interatrial level in the e256 NeoReviews Vol.9 No.6 June 2008 HLHS Surgery In 1980, Norwood and colleagues were the first to describe neonatal palliation that eventually leads to the staged Fontan (atrial-to-pulmonary connection) approach for infants who have single-ventricle physiology. The conventional Norwood procedure must provide unrestricted systemic blood flow by reconstructing the aortic arch, a widely patent interatrial septum, and a source of pulmonary blood flow. Early favorable outcome depends on such preoperative variables as the size of the ascending aorta (preferable situation is prograde flow through the ascending aorta) and good right ventricular and tricuspid valve function. Reconstruction of the ascending aorta and aortic arch require incorporation of the main pulmonary artery and patch augmentation of the aortic arch with homograft material to relieve the associated coarctation completely. The new source of pulmonary blood flow in the modified Norwood operation was a 3.0 to 3.5 Gortex威 central shunt between the right innominate artery and the right pulmonary artery. Systemic-to-pulmonary shunt failure and postoperative difficulty managing pulmonary blood flow led to the resurgence of the Sano modification. This modification uses a right ventricle (RV)-to-pulmonary artery (PA) conduit instead of a central systemic-topulmonary artery shunt. The RV-to-PA conduit results in higher systemic diastolic pressure and better coronary artery perfusion. A multicenter trial is evaluating the central shunt versus Sano modification in terms of perioperative and late morbidity and mortality. The other evolving area of study is the management of cerebral perfusion during aortic arch reconstruction. This operation is performed during a period of deep hypothermic circulatory arrest. Concern for long-term neurologic sequelae has stimulated the development of techniques to eliminate deep hypothermic circulatory arrest. Techniques for maintaining continuous cerebral perfusion are now part of intraoperative management. Advances in critical care and postoperative management have played major roles in improving outcomes. Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology The availability of mechanical/oxygenation support (extracorporeal membrane oxygenation) is mandatory in centers that perform such procedures. The most important factor is the availability of a multidisciplinary team around the clock for these complex patients. HLHS Heart Transplant The Norwood procedure is offered to most patients who have HLHS. Neonatal heart transplant was pioneered by Bailey and Loma Linda University for infants who have HLHS. Although transplantation would be the preferred palliation, donor heart availability limits its use. Centers that recommended heart transplantation have reported a 30% mortality rate among infants waiting for donor hearts. This factor made it clear that the infants who have HLHS and are good Norwood candidates should be referred for a single-ventricle surgical approach. Infants who have tiny ascending aortas or right ventricular dysfunction and severe atrioventricular valve regurgitation should be referred for heart transplantation. hypoplastic left heart disease flow, and factors controlling initial formation of the left atrioventricular junction, have been inferred from chick model experiments. It is likely that multiple causes contribute to HLHS. Prenatal diagnosis has had a major favorable impact on both survival and neurologic outcome. In addition, prenatal diagnosis affords the opportunity for counseling with neonatology and cardiology. Finally, prenatal diagnosis has allowed attempts at in utero treatment of hypoplasia of the left ventricle by balloon dilatation of critical aortic stenosis. However, the group of infants amenable to this treatment represent only a small subset of those born with HLHS. ACKNOWLEDGMENT. Morphology photographs are from the Van Mierop Collection at University of Florida. Courtesy of Diane Spicer. Suggested Reading Comfort Care The offer of no intervention to a family for an infant who is a candidate for single-ventricle palliation remains controversial. Although neonatologists and pediatric cardiologists review with families the diagnosis, prognosis, and potential long-term issues related to single-ventricle palliation, it is the unusual family that chooses no intervention. The current surgical outcomes for infants who experience excellent hemodynamic repair and maintain normal developmental landmarks makes it difficult not to encourage families to pursue care in spite of an uncertain future. Advances in Understanding and Treatment Although congenital heart disease remains the leading cause of death from congenital malformations, advances in neonatal surgery, accurate fetal diagnosis, and improving neonatal management have resulted in increased survival. In fact, there are now more patients who have congenital heart disease older than age 18 years than there are younger patients. HLHS causes significant mortality from birth to age 3 years, when all of the palliative procedures are completed. The cause of HLHS still has not been identified. The condition is reported in families, and the diagnosis is associated with other genetic chromosomal abnormalities, including Turner syndrome. Hemodynamic causes, including abnormalities of atrial septum development, intrauterine cardiac blood Alsoufi B, Bennetts J, Verma S, Caldarome CA. New developments in the treatment of hypoplastic left heart syndrome. Pediatrics. 2007;119:109 –117 Bailey LL. Role of cardiac replacement in the neonate. J Heart Transplant. 1985;4:506 –509 Bailey L, Concepcion W, Shattuck BS, Huang L. Method of heart transplantation for treatment of hypoplastic left heart syndrome. J Thorac Cardiocasc Surg. 1986;92:1–5 Bove EL, Lloyd TR. Staged reconstruction for hypoplastic left heart syndrome: contemporary results. Ann Surg. 1996;224: 387–394 Bradley SM, Atz AM. Postoperative management: the role of mixed venous oxygen saturation monitoring. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2005;8:22–27 Chrisant MR, Naftel DC, Drummond-Webb J, et al; Pediatric Heart Transplant Study Group. Fate of infants with hypoplastic left heart syndrome listed for cardiac transplantation: a multicenter study. J Heart Lung Transplant. 2005;24:576 –582 DeOliveria NC, Van Arsdell GS. Practical use of alpha blockade strategy in the management of hypoplastic left heart syndrome following stage one palliation with Blalock Taussig shunt. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7: 11–15, Ghanayem NS, Cava JR, Jaquiss RD, Tweddell JS. Home monitoring of infants after stage one palliation for hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:32–38 Jenkins PC, Flanagan MF, Jenkins KJ. Survival analysis and risk factors for mortality in transplantation and staged surgery for hypoplastic left heart syndrome. J Am Coll Cardiol. 2000;36: 1178 –1185 Liske MR, Greeley CS, Law DJ, Reich JD, et al. Report of the Tennessee Task Force on Screening Newborn Infants for critical congenital heart disease. Pediatrics. 2006;118:e1250 – e1256 NeoReviews Vol.9 No.6 June 2008 e257 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology hypoplastic left heart disease Mahle WT, Spray TL, Gaynor JW, Clark BJ. Unexpected death after reconstructive surgery for hypoplastic left heart syndrome. Ann Thorac Surg. 1997;71:61– 65 Mahle WT, Wernovsky G. Neurodevelopmental outcomes in hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;127:490 – 497 Marshall AC, Tworetzky W, Bergersen L, et al. Aortic valvuloplasty in the fetus: technical characteristics of successful balloon dilatation. J Pediatr. 2005;147:535–539 Norwood WI, Kirklin JK, Sanders SP. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. 1980; 45:87–91 Norwood WI, Lang P, Hansen DD. Physiologic repair of aortic atresia-hypoplastic left heart syndrome. N Engl J Med. 1983; 308:23–26 Pigula FA, Nemoto EM, Griffith BP, Siewers RD. Regional lowflow perfusion provides cerebral circulatory support during neonatal aortic arch reconstruction. J Thorac Cardiovasc Surg. 2000;119:331–339 Reich JD, Miller S, Brogdon B, et al. The use of pulse oximetry to detect congenital heart disease. J Pediatr. 2003;142:268 –272 Sano S, Ishino K, Kawada M, Honjo O. Right ventricle-pulmonary artery shunt in first stage palliation of hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:22–31 Sedmera D, Cook AC, Shirali G, McQuinn TC. Current issues and perspectives in hypoplasia of the left heart. Cardiol Young. 2005;15:56 –72 Tabbutt S, Ramamoorthy C, Montenegro LM. Impact of inspired gas mixtures on preoperative management of infants with hypoplastic left heart syndrome during controlled ventilation. Circulation. 2001;104(suppl 1):I159 –I164 Tworetzky W, McElhinney DB, Reddy VM, Hanley FL, Silverman NH. Improved surgical outcome after fetal diagnosis of hypoplastic left heart syndrome. Circulation. 2001;103:1269 –1273 Vlahos AP, Lock JE, McElhinney DB, van der Velde ME. Hypoplastic left heart syndrome with intact or highly restrictive atrial septum: outcome after neonatal transcatheter atrial septostomy. Circulation. 2004;109:2326 –2330 NeoReviews Quiz 5. The classic phenotype of hypoplastic left heart syndrome (HLHS) includes left ventricular hypoplasia associated with mitral stenosis/atresia, aortic atresia, coarctation of aorta, and an intact ventricular septum. Of the following, the most accurate statement regarding HLHS is that: A. B. C. D. E. An intact interatrial septum is critical for survival. Functional status of the right ventricle determines the approach to palliation. HLHS accounts for approximately 25% of all cases of congenital heart disease. Left ventricular communication with coronary sinusoids worsens the prognosis. The size of the descending aorta is a risk factor for surgical palliation. 6. You suspect that a 6-hour-old term newborn has HLHS. Of the following, the most consistent clinical finding in this infant would be: A. B. C. D. E. Decreased amplitude of peripheral pulses. Ductal systolic heart murmur. Hyperdynamic precordial activity. Severe cyanosis. Split second heart sound. e258 NeoReviews Vol.9 No.6 June 2008 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 cardiology hypoplastic left heart disease 7. In the initial stabilization of a newborn who has HLHS, attention to balancing the systemic and pulmonary blood flow is critical for successful transition to surgery. Of the following, the initial step in the management of HLHS is the administration of: A. B. C. D. E. Inhaled nitric oxide. Mechanical hyperventilation. Phosphodiesterase inhibitor milrinone. Prostaglandin E1 infusion. Subatmospheric oxygen. 8. Management of HLHS has evolved over the last 3 decades. Of the following, the current approach to management of HLHS in most infants is: A. B. C. D. E. Blalock-Taussig shunt. Comfort care. Glenn shunt procedure. Neonatal heart transplantation. Norwood palliation. NeoReviews Vol.9 No.6 June 2008 e259 Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008 Hypoplastic Left Heart Syndrome: Diagnosis and Early Management Frederick Jay Fricker NeoReviews 2008;9;e253-e259 DOI: 10.1542/neo.9-6-e253 Updated Information & Services including high-resolution figures, can be found at: http://neoreviews.aappublications.org/cgi/content/full/neoreview s;9/6/e253 Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its entirety can be found online at: http://neoreviews.aappublications.org/misc/Permissions.shtml Reprints Information about ordering reprints can be found online: http://neoreviews.aappublications.org/misc/reprints.shtml Downloaded from http://neoreviews.aappublications.org by JoDee Anderson on June 20, 2008