Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Artificial heart valve wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
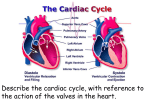
Cardiac Cycle-Chapter 9 • Beginning of one heart beat to the next. – Includes a cycle of contraction and relaxation • Systole: contraction • Diastole: relaxation (filling) • Blood will only move from one chamber to the next if the pressure in the first chamber exceeds the second! • Timing is EVERYTHING! Principles of Pressure and Flow • Measurement: compared to force generated by column of mercury (mmHg) – sphygmomanometer • Change in pressure gradient creates a change in volume (Boyle’s law) • Opposing pressures in atria/ventricles/ large arteries Phases of Cardiac Cycle-step by step800mSec- only 370mSec for Systoles • Quiescent period/ Diastasis– 430mSec – all chambers relaxed – AV valves open – blood flowing into ventricles • Atrial systole- 100mSec – SA node fires, atria depolarize – P wave appears on ECG – atria contract, force additional blood into ventricles – ventricles now contain enddiastolic volume (EDV) of about 120 ml of blood – Heart sound 4 occurs P Isovolumic Contraction of Ventricles • Atria repolarize and relax • Ventricles depolarize • QRS complex appears in ECG • Ventricles contract • Rising pressure closes AV valves • Heart sound S1 occurs • No ejection of blood yet (no change in volume) Ventricular Ejection • Rising pressure opens semilunar valves • Stroke volume: amount ejected, ~ 70 ml • Rapid and reduced ejection phases • SV/EDV= ejection fraction, – at rest ~ 60% – during vigorous exercise as high as 90% – diseased heart < 50% • End-systolic volume: amount left in heart (50ml) • Ventricular systole lasts 270mSec Isovolumic Relaxation of Ventricles • T wave appears in ECG • Ventricles repolarize and relax (begin to expand) • Semilunar valves close • AV valves remain closed • Ventricles expand but do not fill • Heart sound S2 occurs http://highered.mcgrawhill.com/sites/0072495855/student_view0/chapter22/animation__the_cardiac_c ycle__quiz_2_.html Ventricular Filling • AV valves open • Ventricles fill with blood - 3 phases – rapid ventricular filling - high pressure – diastasis - sustained lower pressure – filling completed by atrial systole • Heart sound S3 may occur Cardiac Cycle (cont’d) 4th Heart sounds are from turbulent blood! Figure 9-5; Guyton & Hall Cardiac Output (CO) • Amount ejected by a ventricle in 1 minute • CO = HR x SV • Resting values, usually about 4 to 6L/min • Vigorous exercise CO to 21 L/min for fit person and up to 35 L/min for world class athlete • Cardiac reserve: difference between maximum and resting CO Volumes and Fraction • • • • End diastolic volume = 120 ml End systolic volume = 50 ml Ejection volume (stroke volume) = 70 ml Ejection fraction = 70ml/120ml = 58% (normally 60%) • If heart rate (HR) is 70 beats/minute, what is cardiac output? • Cardiac output = HR * stroke volume = 70/min. * 70 ml = Factors that Affect Stroke volume • EDV- dependent on filling time (diastole) and venous return – Skeletal pumping – Respiratory pumping • ESV– Preload- degree of stretching • Frank-Starling Principle: more in, more out – Contractility of the ventricle • Availability of calcium; positive and negative inotropy – Afterload- amount of tension ventricle must exert to eject; affected by peripheral vasculature; if greater ESV then there was less stroke volume Frank-Starling Mechanism • Within physiological limits the heart pumps all the blood that comes to it without excessive damming in the veins. • Length-tension relationship of cardiocytes. • Extra stretch on cardiac myocytes makes actin and myosin filaments interdigitate to a more optimal degree for force generation. Autonomic Effects on Heart • • Sympathetic stimulation causes increased HR + increased contractility with HR = 180-200 and C.O. = 15-20 L/min. Parasympathetic stimulation decreases HR markedly and decreases cardiac contractility slightly. Vagal fibers go mainly to atria. Fast heart rate (tachycardia) can decrease C.O. because there is not enough time for heart to fill during diastole. Maximum sympathetic stimulation 25 Cardiac Output (L/min) • 20 sympathetic stimulation 15 No sympathetic and no parasympathetic stimulation 10 (Parasympathetic stimulation) 5 0 -4 0 +4 +8 Right Atrial Pressure (mmHg) So What Happens to the Cycle when the heart rate increases? • All phases are shortened • Diastole pays the biggest price! • Reduced by almost 75% at 200bpm • What does that mean? • Less Filling! Factors Influencing CO Figure 14-31: Factors that affect cardiac output Drugs Affecting CO • Atropine- parasympathetic blocking (blocks muscarinic AchR) agent, (+,+) • Pilocarpine- drug that causes cholinergic neurons to release ACH. Since Ach decreases heart rate, it causes (-, ) effect on heart. • Propranalol- Reversible, competitive blocker of Beta1 receptor. So blocks sympathetics effect of heart (-,-) Decrease heart rate and force of contraction, and lowers blood pressure. Drugs Affecting CO (2) • Digoxin (shorter ½ life) or Digitoxin- come from group of drugs derived from digitalis. Digitalis derived from foxglove plant. It has a (-,+) effect, neg chronotropic and positive inotropic effect; slows heart rate but increases force of contraction. Is only drug with this effect on heart. – increases intracellular concentration of Ca. – increase force of contraction by inhibiting Na+/K+ pump. So cells start to accumulate Na. – Disadvantage of using digitalis is that it’s extremely toxic. The optimal dose is very close to lethal dose- stops heart Q: How do cardiac glycosides increase cardiac contractility? • Glycosides (eg. digoxin) inhibit the Na/K ATPase… increase intracellular Na+ decrease Na+ gradient decrease Na+/Ca2+ counter-transport increase intracellular Ca2+ Digoxin has been a cornerstone for the treatment of heart failure for decades and is the only oral inotropic support agent currently used in clinical practice. Na+ Na+ K+ Na+ Ca++