Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Monoclonal antibody wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Gluten immunochemistry wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Autoimmunity wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Rheumatology 2003;42:716–731 doi:10.1093/rheumatology/keg262, available online at www.rheumatology.oupjournals.org Advance Access publication 31 March 2003 Review Exploring the reciprocal relationship between immunity and inflammation in chronic inflammatory arthritis A. P. Cope Experimental models seeking to explore how susceptible individuals develop rheumatoid arthritis (RA) propose that genetic and environmental factors shape a complex series of molecular and cellular interactions leading to a chronic inflammatory response. T lymphocytes and MHC class II genes have featured prominently in these models. More recent studies have suggested that perpetuation of inflammation in a disease-susceptible host might occur through failure to down-regulate the inflammatory process. One prediction from this model is that effective mechanisms of immunoregulation might be most easily investigated in non-susceptible individuals. However, this has been difficult to study in man. Based on the observation that extended MHC haplotypes are strongly associated with RA in different ethnic groups, I have explored the function of human MHC-encoded genes in transgenic mice using two different experimental approaches. First, by comparing the molecular interactions between disease-associated or non-associated HLA-DR4 molecules and CD4+ T lymphocytes, it has been possible to gain insight into how immune responses in non-susceptible individuals might differ from T-cell responses observed in a susceptible host. This has been achieved using transgenic mice expressing RA disease-associated and non-associated human HLA class II molecules. Secondly, the effects of prolonged exposure of T cells to the proinflammatory cytokine tumour necrosis factor a (TNF) have been studied in vitro and in vivo, focusing on T-cell receptor (TCR) signalling and effector responses. In studies of HLA class II transgenic mice, the major differences between disease-associated and non-associated alleles in terms of T-cell responses occur at the level of presentation of antigenic peptides, and the sustained expression of inflammatory cytokines such as TNF. Chronic exposure of T cells to inflammatory cytokines such as TNF induces a phenotype which resembles RA synovial T cells, including the induction of non-deletional and reversible hyporesponsiveness to TCR ligation and uncoupling of proximal TCR signal transduction pathways. The experimental findings are consistent with a model in which HLA class II-driven inflammatory cytokine expression uncouples TCR signalling pathways in the susceptible host in such a way as to profoundly suppress proliferative and immunoregulatory cytokine responses, while at the same time promoting cell survival and effector responses. KEY WORDS: Autoimmunity, Rheumatoid arthritis, T lymphocytes, HLA-DR4, Tumour necrosis factor, T-cell activation, T-cell hyporesponsiveness. Kennedy Institute of Rheumatology Division, Faculty of Medicine, Imperial College London, London, UK. Accepted 30 December 2002. Correspondence to: Kennedy Institute of Rheumatology Division, Faculty of Medicine, Imperial College London, Arthritis Research Campaign Building, 1 Aspenlea Road, Hammersmith, London W6 8LH, UK. E-mail: [email protected] 716 ß 2003 British Society for Rheumatology Immunity and inflammation in chronic inflammatory arthritis Protection against foreign pathogens is the primary function of the immune system. While the innate immune system provides the first line of defence, adaptive immunity and the acquisition of memory responses to foreign antigens is achieved through the generation of an extensive repertoire of lymphocyte antigen receptors. Because this repertoire is generated during thymic maturation and maintained in the periphery through recognition of complexes of self peptide and major histocompatibility complex (MHC) molecules, all peripheral T cells have the potential for autoreactivity. Whilst thymic maturation generates T lymphocytes expressing low-avidity T-cell receptors (TCR) at low precursor frequencies, this recognition mechanism cannot discriminate between self and foreign antigens. Therefore, protective immunity is provided to the host at the expense of a huge propensity for crossreactivity to self tissue antigens w1x. How is it that autoimmunity is very common while autoimmune disease is quite rare? Over the last few years, susceptibility to autoimmunity has been explored not so much in terms of a predisposition to generating autoaggressive effector cells, but more in terms of failure to regulate an autoimmune response wreviewed in 2x. If one considers current concepts of cognate immunity, a defect in immunoregulation could be acquired at multiple points during both early and later phases of an autoimmune response. For CD4+ T lymphocytes, the initial ligand–receptor interaction between MHC–peptide and the TCR is crucial, since this determines qualitative and quantitative aspects of the signals transduced through the TCR w3x. Seen through the eyes of an autoreactive T cell, the evolution of autoimmune disease could be envisaged as a series of checkpoints (Fig. 1). These checkpoints provide a theoretical framework for understanding not only how disease might progress in a susceptible host, but also for exploring how 717 the evolution of autoimmune responses might differ qualitatively in the non-susceptible host. Evolving concepts of disease mechanisms for rheumatoid arthritis (RA) have provided a paradigm for understanding the pathogenesis of autoimmune disease. Over the last 10 yr my research has focused on investigating the reciprocal relationship between the immune response and inflammation in the context of diseases such as RA. Studies have focused on specific questions that have to do with the initiation of the disease process as well as its progression. Specifically, I have addressed (i) the molecular nature of cognate immunity to cartilage antigens in the susceptible host, and how these initial interactions might contribute to autoimmune disease; (ii) how this process might differ in a non-susceptible individual; and (iii) how the chronic inflammatory process in turn influences the evolution of T-cell autoreactivity and effector responses. The experimental strategy is based upon the observation that the strongest disease associations are with genes that contribute to an extended haplotype encoded within the MHC w4x. I will describe experiments undertaken to explore these issues, emphasizing how the results contribute to an understanding of specific disease checkpoints (Fig. 1). I will then discuss how some unexpected results have influenced my own perceptions of how inflammatory arthritis evolves, and conclude by proposing a model of RA that reconciles my observations with current concepts of disease pathogenesis, and which hints at the possibility of new prospects for therapy. Exploring the function of disease-associated HLA-DRB1 genes in rheumatoid arthritis How do we begin to study in man the complex molecular interactions that contribute to the pathogenesis of RA? For many laboratories, the choice of experimental strategy FIG. 1. Immunopathological checkpoints implicated in the pathogenesis of chronic inflammatory arthritis. Activation and subsequent expansion of autoreactive CD4+ T cells lead to cell-to-cell interactions that initiate a cascade of effector responses. According to this model, immunoregulatory mechanisms may influence activation, expansion anduor effector responses. A. P. Cope 718 has been guided by genetic studies which have focused on defining gene polymorphisms which most clearly discriminate between patients with RA and the nonsusceptible host. Some of the strongest associations found in RA patients from different ethnic groups to date are with MHC class II genes w5, 6x. This association was first described by Stastny in the 1970s w7x, but a significant advance in our understanding of these associations was reported more than a decade later, when it was shown that susceptibility to RA across different ethnic populations correlated closely with the expression of a specific consensus amino acid sequence (the ‘shared epitope’) within the HLA-DRb chain w8x. This sequence was subsequently shown by several groups of investigators to be encoded by HLA-DRB1 alleles, including HLA-DR4 (*0401, *0404, *0405 and 0408), but also HLA-DR1 (*0101), DR6 (*1401) and DR10 (*1001) alleles w9–11x. Significantly, some of the key polymorphisms within non-associated DRB1*04 alleles mapped to the same region of the DRb chain a helix (Table 1). For example, DRab1*0402 carries negatively charged residues at b70 and 71, as opposed to the positively charged residues found at b71 in disease-associated DRB1 alleles, while DRab1*0403 (non-associated), which differs from *0404 (associated) by one amino acid, carries a negatively charged residue at codon 74. These associations, together with the finding of follicular aggregates of lymphocytes and antigen-presenting cells (APC) in the synovial tissue of patients with active RA, have provided perhaps the strongest evidence that the immune response contributes to disease chronicity. By studying these associations in patient cohorts that are clinically as well as genetically heterogeneous, it has been possible to identify genotypes that cosegregate with specific clinical features. For example, in population studies, different HLA-DRB1 alleles appear to influence the severity of disease, DRB1*0401 being found in patients with severe, seropositive, erosive RA (often with extraarticular features, such as vasculitis and Felty’s syndrome, in *0401-homozygous or *0401u*0404 compound homozygous individuals), while DRB1*0101 and *1001 are observed at a higher frequency in patients with less severe, seronegative, non-erosive disease w12x. Inheriting two copies of alleles expressing the consensus sequence greatly increases disease penetrance, time of onset and severity. These and other studies have suggested that genetic associations may contribute more to severity than to disease susceptibility wreviewed in 4x. Closer inspection suggests further that, rather than a hierarchy of phenotypes of a single disease, these genetic associations, which are by no means uniform, are reflected clinically as distinct disease entities. These distinct entities may be manifest at the level of synovial histomorphology w13x, somewhat analogously to the histological features that define different forms of B-cell lymphoma. A functional basis for the associations between HLA-DR and RA MHC class II molecules function by selecting and presenting immunogenic peptide fragments of protein antigens to CD4+ T cells. They also play a role in the selection of the TCR repertoire in the thymus. Because CD4+ T cells recognize linear stretches of about 9–20 amino acids derived from self or foreign protein antigens bound in the peptide-binding groove of polymorphic MHC class II molecules, it has been suggested that differences in the way that HLA-DR or -DQ molecules present selected peptides to T cells could be an important mechanism for susceptibility to autoimmune diseases such as RA. According to this model, RA might represent the sequelae of pathological T-cell responses initiated and maintained by antigens presented by disease-associated HLA class II molecules. On the basis of early observations, two principal models were proposed to account for the association between RA and the consensus DRb chain sequence. Both were based on the assumption that the shared epitope is the critical genetic element linked directly to disease. The first model proposed that the shared epitope determines specific peptide binding, and that ‘pathogenic’ peptides bind only to disease-associated HLA class II molecules w14, 15x. This model predicted that a gradient of affinities of disease-inducing peptide for MHC class II molecules might account for the differences in susceptibility anduor severity conferred by different HLA-DR molecules. The second model proposed that the shared epitope influences TCR recognition by binding and selecting autoreactive T cells during thymic maturation, and expanding these populations in the peripheral compartment w16, 17x. Although these models are not mutually exclusive, critical testing of the models in the context of RA has been the subject of intense research in many laboratories. TABLE 1. Amino acid composition of HLA-DR peptide-binding pockets and their associations with RA Pocket 4 HLA-DRB1 allele DRB*0101 DRB1*0401 DRB1*0402 DRB1*0403 DRB1*0404 DRB1*0405 Pocket 6 Pocket 7 Pocket 1 86 13 70 71 74 11 13 28 G G q V V V G F H H H H H Q Q q D Q Q Q R K q E R R R A A A E A A L V V V V V F H H H H H E D D D D D 67 L L q I L L L Pocket 9 71 9 57 RA R K q E R R R W E E E E E D D D D D S + +++ – – ++ + Circles denote amino acid residues in the DR1*0402 molecule that differ in DR1*0401. +++, strong association with RA; –, weak or no association with RA. Immunity and inflammation in chronic inflammatory arthritis Progress in this area has been hampered largely by the fact that, until recently, it has not been possible to compare the function of disease-associated and nonassociated HLA-DR4 molecules in isolation under experimental conditions where the remainder of the genome is fixed. Studying HLA-DR4-restricted T-cell responses in transgenic mice Conceptually, an experimental approach involving the generation of transgenic mice expressing human MHC class II molecules has proved attractive. Such an approach has been developed by a number of laboratories with the intention of studying the function of disease-associated HLA class II molecules in vivo in a way that had not been previously possible in human subjects w18–20x. Comprehensive reviews published recently have detailed the experimental approaches, highlighting the constraints of such models and discussing how these limitations have been resolved w21, 22x. This approach in mice has turned out to be enormously useful for probing in vivo the function of disease-associated and non-associated human MHC class II molecules, and their potential for contributing to the development of inflammatory arthritis w23, 24x. Generating a HLA-DR4-restricted TCR repertoire in transgenic mice Using DR4 transgenic mice that my colleagues and I had generated at Stanford University, it was first necessary to study in detail a CD4+ T-cell response specific for cognate antigen that was restricted to the HLA-DRB1*04 allele encoding HLA-DRab1*0401, and to characterize the immunogenic epitopes presented by these HLA-DR4 molecules in vivo. This allele was chosen because of its strong associations with RA in Caucasians w11x. To this end, it was necessary to generate a repertoire of CD4+ T cells whose TCR had been shaped by HLA-DR4 during thymic maturation. This was only achieved after a detailed analysis of the peripheral CD4+ T-cell compartment in transgenic mice expressing different genotypes w25x. For example, while I-Ab0u0 murine MHC class II-deficient mice have <0.5% mature CD4+ T cells in the peripheral blood w26x, introduction of a single copy of the HLA-DR4 transgene onto this mouse class II-deficient background increased this level to around 4%. After crossing to human CD4-transgenic mice, the peripheral CD4 compartment increased further to 13%, while homozygous HLA-DR4uhuman CD4-transgenic I-Ab0u0 mice had 719 peripheral mouse CD4+ T-cell numbers approaching those observed in mice expressing endogenous mouse MHC class II I-A molecules (;25–30%) w22, 25x. These observations, combined with the fact that HLA-DR4 had been shown to alter the repertoire of selected Vb TCR in I-A-expressing mice w18x, demonstrated that human HLA-DR4 can shape, both quantitatively and qualitatively, the TCR repertoire in mice. It also provided a molecular framework for exploring in depth the specificity of mature CD4+ T cells that had previously undergone maturation and selection through cognate interactions with self-peptideuHLA-DR4 complexes in the thymus of transgenic mice. What do HLA-DR4-restricted T cells really see? HLA-DR4-restricted T-cell responses were defined using human cartilage (HC) gp-39 as a model antigen w27x. Although HCgp-39 is expressed in many tissues, it is produced in abundance by chondrocytes, and protein is present in synovial membrane as well as synovial fluid and serum w28–30x. The finding that mRNA transcripts are not detectable in healthy cartilage explants but can be induced in tissue from arthritic joints, as well as by proinflammatory cytokines in vitro, made this an attractive candidate antigen for study w28, 29x. Through the generation of immortalized T-cell hybridomas, the specificities of literally thousands of T-cell responses were evaluated. From more than 250 HCgp-39-specific responses, nine immunogenic epitopes were identified, with frequencies of responses of T cells to specific peptides ranging from <1% to as high as 35% of the Tcell response, indicating that this was a sensitive as well as a specific method for studying HLA-DR4-restricted T-cell responses in vivo w27x. Epitopes 100–115, 262–277 and 322–337 contributed around 80% of the total peptide specificity (Table 2), but, surprisingly, not one of these peptides carried the predicted charged residue at position 4. More than 95% of all antigen-specific responses were restricted to HLA-DR4, the remainder being restricted to the DRauI-Eb cross-species heterodimer, which is also expressed in these mice, albeit at very low levels. All responses could be blocked with antiDR monoclonal antibodies, and each epitope identified was subsequently found to be processed and presented efficiently by human DRab1*0401-expressing APC. In a pilot study designed to validate the relevance of HCgp39 epitopes defined in mice, all immunogenic epitopes of HCgp-39 were capable of eliciting peripheral blood TABLE 2. Characteristics of immunodeficient epitopes of HCgp-39 defined in HLA-DR4-transgenic mice Frequency of HLA-DR4 restricted hybrids Peptide residue 100–114 (106–114) 262–277 (265–273) 322–337 (328–336) 22–37 (25–33) 298–313 (302–310) *0401 (n=250) 20 34 27 0 0 Core motif relative position *0402 (n=141) 1 2 3 4 5 6 7 8 9 <1 <1 0 32 54 F F Y V L S T D C R K L D Y G I A Q Y A A S E T T S S S S V N E V W H T T K S R Q G S Q T Adapted from reference 27 and reviewed in more detail in 22. 720 A. P. Cope T-cell proliferative responses in at least some patients with RA carrying HLA-DRB1*04 alleles encoding the shared epitope consensus sequence w27x. This approach made it possible to define precisely, for HLA-DR4-restricted T cells, the immunodominant epitopes of a cartilage antigen that elicited T-cell responses in patients with RA, and as such defined at the molecular level the first checkpoint, defined as cartilage antigen peptide-specific recognition by TCR (checkpoint 1, Fig. 1). According to these data, TCR recognition appeared to be highly specific for a large number of clones, because strict dependence on specific peptide for reactivity was demonstrated and TCR triggering did not occur in the absence of specific peptide. However, more detailed analyses indicated that seemingly monospecific T cells were also cross-reactive. Immunization with HCgp-39 promotes reactivity to self-peptide–self-MHC complexes While screening for positive responses to HCgp-39, a subset of hybrids (;15–20%) were found to be highly reactive to transgenic but not non-transgenic splenic APC in the absence of exogenous antigen w31x. Similar responses were observed when DRab1*0401-expressing Epstein–Barr virus-transformed B cells were used as APC. These responses were directed to complexes of self peptide and HLA-DR4, since they could be inhibited by anti-DR monoclonal antibodies. Detailed analysis of self-reactive T cells revealed great flexibility of TCR recognition at multiple levels w32x. Activation of a subset of clones was further enhanced by the addition of HCgp-39 or a panel of peptides derived from HCgp-39. These intramolecular peptide mimics, while carrying predicted HLA-DR-binding motifs, carried sequences which were quite distinct from each other at the amino acid level. These clones also responded to APC expressing closely related HLA-DRB1 alleles that encoded the shared epitope consensus sequence b67–74, with or without exogenous antigen. Responses to DRab1*0401 and to *0405 APC were particularly vigorous, while responses to DRab1*0402 and *0403 were never observed (Fig. 2). These data provided direct evidence for diversity and flexibility of TCR recognition early in the evolution of the immune response, and demonstrated that crossreactivity to self-peptide–self-MHC complexes following immunization with cognate antigen is frequent. For many responses, MHC-biased recognition by TCR predominated. For these T cells, one might predict charge complementarity between MHC shared epitope sequences and TCR complementarity-determining regions (Fig. 3B), as proposed recently w33x, rather than between MHC and cognate peptide (Fig. 3A). This cross-reactivity would also provide a mechanism through which critical precursor frequencies of autoreactive T cells could be achieved, and, because of MHC-directed recognition, could evolve by propagation through interactions largely independent of specific antigen. According to this model, the peptide is permissive for TCR recognition (checkpoint 2, Fig. 1). While the fact that the repertoire of TCR is shaped on self-peptide–self-MHC complexes during thymic maturation provides the most plausible explanation for this, the model provides further evidence that cross-reactivity of peripheral T cells is universal w1x. In the light of these observations, it should be possible to demonstrate broad self-reactivity for all TCR, including populations of peptide-specific T cells that are apparently monospecific, seemingly lacking the broad flexibility of other T-cell subsets. Because immune responses to foreign antigens are generated from the same pool of potentially selfreactive TCR, it follows from this that immunization of HLA-DR4-transgenic mice with proteins derived from foreign pathogens would activate and expand populations of autoreactive T cells. FIG. 2. Flexibility of TCR recognition by HCgp-39-specific T cells. (A) T cells were stimulated with APC plus HCgp-39 peptides or native antigen. Note high background counts (>100 000 IL-2 fluorescence units) in the absence of antigen. (B) T cells were stimulated with a panel of DRB1-expressing APC in the absence of exogenous antigen. Data are shown for clones 4A10 and 1A2, both specific for peptide 262–277. Results are expressed as arbitrary IL-2 fluorescence units. Immunity and inflammation in chronic inflammatory arthritis FIG. 3. Schematic representation of the amino acid charge complementarity that could exist between (A) residue b71 of the DRb-chain shared epitope sequence and position 4 (P4) of the specific peptide, or (B) residue b71 of the DRb-chain shared epitope sequence and residues encoded by the complementaritydetermining region (CDR) of the TCRb chain. Analysis of HCgp-39-specific T-cell responses indicates that the charge complementarity illustrated in scheme B may predominate, as immunodominant peptide epitopes carry neutral amino acids at P4. Self-reactivity following immune responses to foreign pathogens In collaboration with the Kamradt laboratory, this hypothesis was tested directly by repeating the immunization strategy outlined above, but this time substituting OspA for HCgp-39, the outer surface protein A derived from the tick-borne spirochete Borrelia burgdorferi, the causative organism of Lyme disease w34x. This was a relevant model antigen to study because CD4+ T-cell responses to OspA have been implicated in chronic treatment-resistant Lyme arthritis, and the disease is also associated with HLA-DR4 w35–37x. Large numbers of HLA-DR4-restricted, OspA-specific T-cell hybridomas were generated, and the immunodominant epitopes were identified as before w38x. Two strategies were employed for identifying selfpeptide mimics of immunodominant OspA epitopes capable of stimulating OspA-specific T cell-hybridomas. An example is shown in Fig. 4 for OspA peptide 235– 246. In the first strategy, the SwissproteinuTREMBL database was used to define mimics of OspA peptides on the basis of conventional sequence alignment. In the second, a systematic amino acid analysis was undertaken, replacing each residue of the core 9-mer OspA epitope with all naturally occurring amino acids and testing responses of OspA peptide-specific T cells to these synthetic derivative peptides. On the basis of the amino acid substitutions permissive for T-cell responsiveness, a structural ‘supertope’ motif was defined and used to scan the same database. Mimics were identified and synthesized prior to testing on a panel of OspA-specific T-cell hybridomas. The results were remarkable in several respects w38x. When responses to the ‘best fit’ peptides, identified by 721 FIG. 4. Schematic for demonstrating cross-reactivity of OspAspecific T cells to self-peptide mimics. Candidate peptide mimics were identified by sequential substitution analysis of each amino acid residue of the core epitope, or by a database search for sequence alignment. Peptide mimics were identified and the best-fit peptides synthesized and tested on panels of OspA-specific T-cell hybridomas. Mimics that carried the ‘supertope’ motif were identified, and these were capable of stimulating OspA-specific T cells. either alignment or substitution analyses, were compared on the panel of T cells that responded to the original peptide, reactivity was most frequently observed with peptide mimics fulfilling the supermotif. Intriguingly, many of these peptide mimics, derived from both mouse and human proteins, bore little or no resemblance to the wild-type sequence. Indeed, for some there existed no homologies at any residue. By contrast, few if any peptides identified by conventional sequence alignment stimulated OspA-specific T cells (Fig. 4). This lack of reactivity was analogous to that which I had observed for human HCgp-39 specific T cells when tested on the closely homologous but not identical mouse peptides w22x. These findings support data from other laboratories w39–41x, and predict that multiple cross-reactive selfligands can be identified between immunodominant epitopes of autoantigens and any protein derived from infectious pathogens. They provide direct evidence that T cells apparently highly specific for a given peptide ligand are also broadly cross-reactive to self-peptide ligands, and illustrate that recognition of MHCupeptide complexes by TCR is degenerate w41x. The model also indicates that progression across checkpoints 1 and 2 (Fig. 1), namely T-cell activation by cognate antigen and expansion of cross-reactive clones, is almost simultaneous. Studying the progression through disease checkpoints in the non-susceptible host The experiments outlined above provided an experimental framework for exploring in the laboratory how the immune system of an RA-non-susceptible host could function in ways that might attenuate inflammatory 722 A. P. Cope responses in synovial joints. The generation of transgenic mice identical to HLA-DRab1*0401-expressing mice, with the exception that they express an allele of HLADRB1*04 that is not associated with RA (DRab1*0402), made it possible to address this w27x. A comparative analysis between transgenic lines would also make it possible to examine whether just four amino acid differences, which distinguish DRB1*0401 from *0402 at codons 86, 69, 70 and 71 (Table 1), were sufficient to alter the molecular interactions between APC and antigen-specific T cells. Closer scrutiny of the sequence and molecular models indicate that these four amino acid changes would have several effects, including a reduction in the size of the P1 peptide-binding pocket (which may influence TCR recognition), and changing the charge preference for peptide residues sitting in pocket 4 from negative to positive w42x. Molecular modelling predicts that gp-39 epitopes presented by DRab1*0402 should carry small aliphatic hydrophobic residues at P1, and would exclude positively charged residues at P4 w15x. As well as studying the molecular nature of immunodominant peptides processed and presented by DRab1*0402-expressing APC in vivo, it would also be possible to evaluate whether there was evidence of an attenuated effector response in T cells from transgenic mice carrying the non-associated DRab1*0402 genotype, and what immunoregulatory mechanisms were in evidence, if any. Do HLA-DRab1*0402 molecules present different epitopes to CD4+ T cells in vivo? Using HCgp-39 as the model antigen, immunization of HLA-DR4-transgenic lines expressing DRab1*0402 revealed that this molecule, differing from DRab1*0401 by only four amino acids, presents quite distinct sets of immunodominant peptides of HCgp-39 to CD4+ T cells in vivo w27x (Table 2). As observed for DRab1*0401 epitopes, these peptides did not carry the expected charged residues at P4. On the other hand, DRab1*0402, which has a smaller P1 pocket, bound by Val rather than Gly at position b86, favoured binding of peptides with smaller aliphatic residues at P1 (Val or Leu), as predicted from the algorithm of Sinigaglia and Hammer w15x. Because experiments have revealed that there exists in DRab1*0401 mice a repertoire of T cells capable of recognizing 298–313 peptide w27x, one possible explanation for these findings could relate to differences in antigen processing and presentation of this peptide between DRab1*0401 and *0402-expressing APC. Indeed, collaborative studies with the laboratory of Dr E. Mellins suggest that dependence on HLA-DM for processing of HCgp-39 peptides may explain some of these differences, at least in part w43x. For example, data published by Hall and colleagues w44x since this essay was first submitted have confirmed a relationship between immunogenicity of HCgp-39 peptides and MHC–peptide stability, dictated by the relative sensitivity to HLA-DM editing at pH5.5, the pH of the peptide loading compartment. Regardless of the mechanisms, these data provided evidence that non-associated alleles of HLA-DRB1 profoundly influence the molecular nature of the interactions between TCR and peptide–MHC complexes. Is the cytokine effector response different for HLA-DRab1*0402-restricted T cells? The effects of HLA-DRab1*0402 on this particular disease checkpoint were addressed by comparing cytokine expression of draining lymph-node T cells from DRab1*0401 and *0402 mice immunized with HCgp-39, following restimulation with native antigen or the relevant pool of immunodominant epitopes w27x. The results were interesting in several respects. While T-cell proliferation was no different for DRab1*0401 and *0402-restricted responses, HCgp-39-specific lymphnode T cells from DRab1*0402-transgenic mice produced significantly less interferon c (IFN-c) w27x. On the other hand, DRab1*0402 T cells specific for OspA produced abundant IFN-c, indicating that DRab1*0402 mice did not have an intrinsic defect of IFN-c production. These data provided the first real clues that one of the consequences of DRab1*0402 presenting different peptides was to induce a very different profile of proinflammatory cytokine production. The finding of substantially reduced TNF-a levels in DRab1*0402 cultures is also consistent with this model w27x. The results are also compatible with models which suggest that, unlike disease-associated HLA-DR4 molecules, non-associated HLA-DR4 molecules, such as DRab1*0402, could provide disease-protective effects by altering the peptides presented to T cells and the cytokines produced as a consequence of these molecular changes (checkpoint 4, Fig. 1). Such a notion was proposed many years ago to account for the sequence differences in diabetessusceptible and non-susceptible alleles w45x. The data also substantiate the view that overproduction of proinflammatory cytokines early in the evolution of an immune response may be central to the subsequent progression of the inflammatory process (checkpoint 3, Fig. 1). They are consistent with the hypothesis that the proinflammatory cascade is attenuated in the non-susceptible host through the expression of a subset of HLA-DRB1 genes which profoundly influence the molecular nature of CD4+ T cell–APC interactions and immune effector responses (checkpoint 4, Fig. 1). The chronic phase of inflammation Much attention has focused on the role of cytokines in the pathogenic events that ultimately result in cartilage destruction and bone erosion wreviewed in 46x. The experiments described above demonstrated that the initial stimulation of T cells by complexes of antigenic peptide and disease-associated, but not non-associated, MHC class II molecules could profoundly influence the expression of proinflammatory cytokines. This cytokine drive may well be central to sustaining the chronic phase of disease, because in mutant mouse models it is possible to induce chronic inflammatory disease in the absence Immunity and inflammation in chronic inflammatory arthritis of functional T and B lymphocytes by sustained overexpression of proinflammatory cytokines in vivo. These mouse models have been highly informative. Nonetheless, for RA patients with an intact adaptive immune system, studying the reciprocal relationship between inflammation and immunity and exploring how chronic overexpression of cytokines might promote T-cell effector responses became a priority. T cells are chronically exposed to TNF in synovial joints My own studies of how the inflammatory milieu influences the function of chronically activated T cells were undertaken during my PhD studentship in the Feldmann laboratory at the Kennedy Institute of Rheumatology. I began to explore how the chronic inflammatory process influenced the differentiation and effector functions of chronically activated T cells in the belief that the inflammatory environment in established chronic inflammation might be quite different from that which influences the very earliest events of T-helper cell differentiation. At the time, I set out to test the hypothesis that the inflammatory milieu promotes the inflammatory response by enhancing T-cell proliferative and cytokine responses. The results were unexpected, and were partly a consequence of the experimental design. The approach I chose was based on three fundamental experimental observations. First, proinflammatory cytokines, such as TNF and interleukin 1 (IL-1), were expressed and up-regulated at the protein and mRNA levels in synovial tissue from RA patients w47–49x. Secondly, experiments in the laboratory had confirmed that infiltrating mononuclear cells expressed cognate cytokine receptors w50x, which were preferentially up-regulated on synovial compared with peripheral blood cells w51x, and that ligand colocalized with cells expressing the cognate receptor w52x. This was most comprehensively documented for the prototypic inflammatory cytokine TNF, at a time when the possibility that TNF could be implicated in the chronic phase of RA pathogenesis was only beginning to emerge w53x. Thirdly, I demonstrated for the first time that expression of the naturally occurring TNF inhibitors, the soluble TNF receptor (TNF-R; p55 and p75 sTNF-R), were also substantially increased at the site of inflammation w54x. However, despite levels 3- to 5-fold higher in the synovial joint fluid compared with serum, levels were insufficient to neutralize completely the biological effects of TNF in the joint. Thus, the possibility that activated mononuclear cells, including T cells, were exposed to cytokines such as TNF for prolonged periods at sites of inflammation in vivo was beyond doubt. Chronic TNF induces reversible, non-deletional T-cell hyporesponsiveness I then set about trying to mimic chronic TNF exposure in an in vitro model, and subsequently in vivo. The results, summarized in Table 3, are derived from an extensive analysis of human and murine T-cell lines and clones in vitro, and from experiments in vivo undertaken 723 TABLE 3. TNF induces non-deletional and reversible T-cell hyporesponsiveness in vitro and in vivo Chronic exposure to TNF suppresses T-cell activation Proliferation and cytokine production (Th1 and Th2 cytokines) Dose- and time-dependent Observed at non-toxic concentrations of TNF IL-2 and mitogen responses are spared Inducible over days Shedding of soluble TNF-R is impaired Rapid reversibility in vitro and in vivo on withdrawing TNF Data are derived from an extensive analysis of T-cell responses in man and transgenic and mutant mice. For more detailed review see reference 75. in TCR-transgenic mice treated with recombinant TNF or anti-TNF, or after intercrossing to human TNF (hTNF)–globin-transgenic mice, as well as in p55 and p75 TNF-R deficient mice w55–57x. The principle finding—that chronic TNF suppressed T-cell activation—was unambiguous, and could not have been predicted from published data at that time, which suggested that TNF was costimulatory and a growth factor for T cells w58x. Moreover, the p55 TNF-R appeared to be necessary and sufficient for sustained TNF signalling to induce T-cell hyporesponsiveness. T cells from patients with RA are hyporesponsive to TCR engagement While histological and flow-cytometric analysis of RA synovial T cells and knowledge of the HLA class II associations discussed above have done much to perpetuate the notion that a chronic antigen-driven immune response is central to the disease process w13, 59x, functional studies of synovial T cells have continued to perplex workers in this field. The laboratory of Panayi was one of the first to appreciate the potential importance of the finding that proliferative T-cell responses to recall antigens, such as purified protein derivative (PPD), or to mitogens or following cross-linking of the TCR, were dramatically attenuated w60x. Since then a hierarchy has been documented from peripheral blood to synovial tissue, in increasing order of hyporesponsiveness, suggesting not only that loss of T-cell reactivity is acquired, but also that this phenotype may be induced by the inflammatory process itself w61, 62x. According to the results described above, chronic exposure to TNF could provide one possible mechanism for this effect. Chronic TNF exposure uncouples proximal TCR signal transduction pathways To explore this at the molecular level, a mouse T-cell hybridoma model has been studied in my laboratory, because with this model it is possible to reproduce many of the functional T-cell defects of primary T cells chronically exposed to TNF in vivo, but in the absence of accessory cells w63x. Several lines of experimental evidence suggested that chronic TNF exposure impairs T-cell activation by attenuating TCR signalling pathways w63x. First, T cells chronically exposed to TNF required more peptide for longer periods to commit to IL-2 production, suggesting that the threshold of activation 724 A. P. Cope was dramatically altered. Secondly, cell surface TCR expression was reduced, indicating that not only did chronic TNF uncouple TCR signalling pathways, but also that TNF interrupted assembly of the TCR–CD3 complex and its transport to the cell surface. Thirdly, a detailed biochemical analysis of proximal TCR signalling pathways in TNF-treated T cells confirmed that, through persistent expression and signalling of inflammatory mediators such as TNF, the chronic inflammatory process was capable of uncoupling antigen receptor signalling directly. In the light of this, it became imperative to explore how chronic TNF targeted the expression of the TCR– CD3 complex, and what effect this might have on downstream signalling pathways (for a schematic of TCR–CD3 assembly and signalling pathways, see references 64 and 65 and Fig. 5). TCR-z was one possible target of TNF. Indeed, following closely the kinetics of IL-2 down-regulation, western blotting analysis of whole-cell lysates revealed that chronic TNF exposure suppressed the expression of TCR-z in a dose- and timedependent fashion, while levels of CD3-e, -c and -d, as well as the protein tyrosine kinases ZAP-70, p56Lck and p59Fyn, were not altered w63x. By immunoprecipitation analysis it was possible to demonstrate that cell surface CD3-e was in fact reduced compared with levels in immunoprecipitates derived from whole cell lysates. This was consistent with a model in which TNF appeared to disrupt the assembly anduor cell surface stability of TCR–CD3 complexes through its effects on TCR-z expression w63x. A second unexpected experimental observation provided further evidence that persistent TNF signalling in T cells influenced TCR–CD3 complex assembly and stability at the T-cell surface. Immunoblotting analysis of unstimulated and TNF-stimulated T cells revealed that the expression of the novel transmembrane adapter TRIM (T-cell receptor interacting molecule) was markedly down-regulated by TNF treatment. Closer examination demonstrated that TRIM expression was reduced by TNF before changes in TCR-z expression could be detected, and that reconstitution of both TRIM and TCR-z expression was required to fully restore TCR responsiveness in TNF-treated cells. The implications of these findings have only recently become apparent, through studies of TRIM expression in human peripheral blood and Jurkat T cells w66, 67x. In collaboration with Dr Burkhart Schraven, we demonstrated that FIG. 5. TCR signal transduction pathways. Polymorphic TCR-ab chains associate with the invariant chains (CD3-c, - d and -e and TCR-z), consisting of non-covalently linked ce and de heterodimers and disulphide linked z–z homodimers, which transmit signals inside the cell. TCR ligation leads to the phosphorylation of tandemly arranged tyrosine residues within immunoreceptor tyrosinebased activation motifs (ITAMs) of TCR-z chain and CD3-c, -d and -e chains by src family kinases, notably Lck and Fyn. The phosphorylation of adapter proteins, such as p36LAT by ZAP-70 and src kinases, serves as a crucial link between membrane proximal phosphorylation events and the activation of downstream RasuMAPK (ERK) and calcium signalling pathways. Sustained activation of these pathways is required for transactivation of the transcription factor AP-1 complex and NFAT, leading to IL-2 production, T-cell proliferation and effector responses. LAT, linker for activation of T cells; MAPK, mitogen-activated protein kinase; AP-1, activating protein 1; NFAT, nuclear factor of activated T cells; PLC, phospholipase C; PIP, phosphoinositol phosphate; InsP3, inositol triphosphate; DAG, diacylglycerol; PKC, protein kinase C; SLP-76, SH2-domain containing leucocyte protein of 76 kDa; Vav, a Rac/Rho-specific guanine nucleotide exchange factor; SOS, son of sevenless. Immunity and inflammation in chronic inflammatory arthritis TRIM plays a role in regulating the cycling of TCR– CD3 complexes at the cell surface w67x. For example, the half-life of TCR–CD3 complexes in stable Jurkat clones overexpressing TRIM is increased. This in turn leads to increased cell surface expression of TCR and enhanced signalling responses, as determined by intracellular calcium mobilization w67x. We can speculate from these experiments that sustained TNF signals in T cells could impair TCR–CD3 assembly not only through its effects on TCR-z expression, but also by reducing the half-life of assembled complexes at the cell surface by downregulating the expression of TRIM. The kinetics of these changes, as well as the precise interactions between TCR-z and TRIM, are currently under investigation. Nevertheless, the findings provided a molecular basis for the profound hyporesponsiveness of T cells following TNF stimulation, and predicted that downstream TCR signalling pathways might be significantly attenuated as a result. Selective uncoupling of downstream TCR signalling pathways by TNF A comprehensive analysis of signalling pathways in control and TNF-treated T cells has been undertaken to establish to what extent distal TCR signal transduction pathways were attenuated as a consequence of the proximal defects outlined above. As a direct consequence of TCR-z phosphorylation being reduced in TNF-treated T cells, downstream signalling events, such as recruitment of ZAP-70 to phospho-TCR-z through its SH2 domains and its subsequent phosphorylation, were also impaired w63x. The transmembrane adapter protein linker for activation of T cells (LAT) is an in vivo substrate for ZAP-70 kinase, and plays a key role in linking membrane proximal events with both calcium and RasuMAPK (mitogen-activated protein kinase) pathways w68, 69x (Fig. 5x. LAT and PLCc1 phosphorylation were substantially reduced in TNF-treated cells, and as predicted intracellular calcium mobilization was also dramatically attenuated w63x. On the other hand, Rasdriven pathways, including activation of the MAPK ERK activation, c-Fos induction and TCR-induced CD69 expression, were preserved (J. Clark, K. Aleksiyadis and A. Cope, unpublished data). These findings identify a novel molecular basis for T-cell hyporesponsiveness. They are of interest because attenuation of intracellular calcium mobilization and preservation of RasuERK (extracellular signal-regulated kinase) signalling is the reverse of the aberrant TCR signalling pathways defined in anergic T cells by other laboratories, whereby calcium responses are spared and RasuERK signals are attenuated w70, 71x. TCR signalling is also defective in RA synovial T cells Impaired TCR signalling has been well documented in RA synovial T cells. Down-regulation of TCR-z chain expression and abnormal recruitment and phosphorylation of p36 LAT have also been documented w72, 73x. Significantly, calcium mobilization is also reduced in 725 peripheral blood as well as synovial T cells from patients with RA w74, 75x, while unpublished data indicate that Ras activation is up-regulated in synovial T cells (C. Verweij, personal communication). On the basis of our own studies, TNF could be one of several factors, including other cytokines or reactive oxygen species, responsible for the uncoupling of TCR signals in chronic inflammatory diseases such as RA in man w55, 76x. Studying T-cell hyporesponsiveness in the mouse: lessons from in vivo models The precise significance of T-cell hyporesponsiveness in the context of chronic inflammatory disease in vivo is not clear. Nevertheless, the distinctive cell phenotypes shared by RA synovial T cells and T cells chronically exposed to TNF in vitro or in vivo (summarized in Table 4) have made it possible to draw some tentative conclusions based upon results derived from experiments in the mouse. I have recently reviewed the possible contributions that hyporesponsive T cells could make to the pathogenesis of autoimmune disease w32, 76, 77x; these are illustrated in Fig. 6. Several points are worthy of note. Jacob and McDevitt w78x first demonstrated that TNF therapy was beneficial in a murine model of lupus. Similar results followed in the NOD mouse w79, 80x, a model of spontaneous type I diabetes, and subsequently TABLE 4. Chronic exposure of T cells to TNF induces a phenotype resembling CD4+ T cells derived from inflamed RA synovial joints Up-regulation of activation antigens Induction of proliferative hyporesponsiveness Suppression of T-cell cytokine production Repression of CD28 gene transcription Uncoupling of proximal TCR signal transduction FIG. 6. Possible mechanisms through which hyporesponsive T cells could contribute to the pathogenesis of chronic inflammatory arthritis. Hyporesponsive T cells could reflect an adaptive response aimed at suppressing T-cell autoreactivity. According to this model, T cells would play little or no role in promoting disease, since hyporesponsiveness constitutes a protective response (left panel). Alternatively, impaired T-cell activation could promote and perpetuate the chronic inflammatory response, through loss of tolerance mechanisms that require intact TCR signalling pathways (right panel). Host defence would be compromised through similar mechanisms. 726 A. P. Cope in studies of experimental autoimmune encephalomyelitis w81x, the murine counterpart of multiple sclerosis in man. My own studies using similar treatment protocols, but in a TCR-transgenic mouse model, demonstrated conclusively that TNF could suppress T-cell effector responses in vivo, either when TNF was administered intraperitoneally or when TCR-transgenic mice were crossed to human TNF–globin transgenic mice w57x. The finding that neutralizing TNF in healthy TCR-transgenic mice enhanced T-cell responses provided the first evidence that physiological expression of this cytokine could suppress T-cell responses in vivo. More recently, the outcome of disease progression in autoimmune-prone mice carrying null mouse TNF or TNF-R (knockout) genes has substantiated the view that TNF has potent immunomodulatory effects in vivo w81–84x. These data point to the possibility that the suppressive effects of chronic TNF are protective, perhaps reflecting an adaptive response to inflammatory signals which attenuate pathogenic T-cell effector responses w57, 76x (Fig. 6, left panel). Studying T-cell hyporesponsiveness in man: lessons from the clinic Back in 1992, I was provided with a unique opportunity to test in patients whether TNF could suppress T-cell activation in man. At this time, a cohort of RA patients with active disease had been recruited to an open-label trial of anti-TNF monoclonal antibody therapy winfliximab (Remicade2)x for the first time. By studying peripheral blood T-cell proliferative responses to recall antigens and mitogens before and after treatment, I found that T-cell responses were dramatically restored w55x. These findings were entirely in keeping with the in vitro data w55x, and have since been reproduced by several groups w85–87x, including a more recent study of T-cell responses to influenza haemagglutinin peptide and collagen II in RA patients treated with the p75 TNF-R– Fc fusion protein etanercept (Enbrel2) w88x. Despite this enhanced T-cell reactivity, multicentre trials of anti-TNF have demonstrated conclusively a consistent and rapid improvement in clinical parameters in ;70% of RA patients w89–91x. Equally striking clinical responses to anti-TNF have been documented in inflammatory bowel disease, particularly Crohn’s disease w92, 93x. These therapeutic responses have prompted an evaluation of TNF blockade in psoriatic arthritis, ankylosing spondylitis and vasculitis. While it has been postulated that the clinical response reflects the potent anti-inflammatory properties of antiTNF, including effects on cell trafficking and angiogenesis w94, 95x, the sustained clinical response to a single infusion of anti-TNF for periods that extend far beyond the time point at which antibody is cleared from the body w89x suggests that anti-TNF may induce lasting immunomodulatory effects (Fig. 6, right panel). We are currently exploring in the laboratory the possibility that, through restoring thresholds of T-cell activation, the immune system is reset, regaining the regulatory functions of T cells which in the non-susceptible host effectively suppress inflammatory responses. By restoring the integrity of TCR signal transduction pathways, autoreactive T cells would also acquire the capacity to undergo activation-induced cell death. The finding that gut CD4+ lymphocytes from patients with Crohn’s disease undergo apoptosis following anti-TNF therapy is consistent with this model w96x. This sudden increase in apoptosis might also explain, at least in part, the development of antinuclear antibodies in ;8% of patients treated with anti-TNF w97x. On the other hand, the concept that restoring T-cell responses would enhance host responses to foreign pathogens, as well as anti-tumour immunity, is more obvious. In diseasesusceptible individuals, therefore, sustained overexpression of TNF could contribute to disease pathogenesis through effects which include attenuation of TCR signalling. This might lead to the failure of immunoregulatory mechanisms critical for maintaining peripheral tolerance, such as activation-induced cell death and immune deviation (Fig. 6, right panel). According to the proposed model, TCR signalling and, by inference, immunoregulation would be predicted to be intact in non-susceptible individuals (checkpoint 4, Fig. 1). Is a shift from ‘antigen mode’ to ‘inflammation mode’ characteristic of effector T cells in chronic inflammatory disease? As TCR hyporesponsiveness in chronic inflammation appears to correlate with disease severity anduor chronicity regardless of immunosuppressive therapy w55, 61x, it is difficult to reconcile the long-held belief that T-cell effector responses in inflamed joints are exclusively antigendriven. Rather, data suggest that during the chronic phase of the disease process it may be the cytokine milieu that sustains and maintains pathogenic T cells w98, 99x. According to this model there is a gradual decline of antigen-induced proliferative responsiveness as cytokine drive increases (Fig. 7). Nevertheless, antigen drive and cytokine drive are inextricably linked in the sense that the initial antigen response initiates both a cytokine cascade and the acquisition of cytokine responsiveness through up-regulation of cytokine receptors, while T-cell hyporesponsiveness arises through subsequent sustained expression of inflammatory cytokines (Fig. 7). How could hyporesponsive T cells contribute to the effector phase of inflammation? Or are they passive bystanders? One possible explanation lies in the observation that depletion of hyporesponsive T cells from RA synovial mononuclear cell cultures significantly reduces the expression of proinflammatory cytokines w100x. Evidence suggests that this process of activation may be mediated by cell-to-cell contact, by as yet poorly defined receptor–ligand interactions w101–103x. Failure of synovial joint T cells from RA patients to undergo apoptosis could further facilitate cell-to-cell signals and perpetuate the inflammatory response w98x. Perhaps B-cell help and autoantibody production is enhanced through similar cell-to-cell mechanisms wreviewed in 104x. In order to Immunity and inflammation in chronic inflammatory arthritis FIG. 7. A model for the role of CD4+ T cells in the pathogenesis of chronic inflammation. Antigen drive may predominate during the early phase of inflammatory responses. T cells could be recruited through bystander activation, or by stimulation with self antigens released from inflamed tissues. As the inflammatory process progresses, chronic cytokine production induces profound non-deletional T-cell hyporesponsiveness. Hyporesponsive T cells function as effector cells and sustain the chronic inflammatory process through mechanisms less dependent on antigen signals (see text). It is proposed that, by reversing T-cell hyporesponsiveness, antigen-dependent responses that serve to regulate the inflammatory process (e.g. through expression of immunoregulatory cytokines) are restored. address this issue specifically, we have recently undertaken gene expression profiling of control and TNFtreated mouse T cells. Preliminary data suggest there is a TNF-induced gene expression signature which, in vivo, would be predicted to favour Th1 cell differentiation [induction of interferon regulatory factor-1 (IRF-1), IL12Rb1 and IFN-cR genes], recruitment of T cells to inflamed joints wfucosyltransferase VII, interferongamma-inducible protein 10 (IP-10) and RANTES (regulated upon activation, normal T-cell expressed and secreted cytokine)x, effector responses initiated through cell surface ligands such as RANK (receptor activator of nuclear factor kB) ligand and cell survival (induction of anti-apoptotic genes cIAP-2, A20 and Bis). These may turn out to be important results because if the data can be reproduced in vivo they imply that hyporesponsive synovial T cells are not inert, but have the potential to become potent effector cells through dominant cytokinedriven signal transduction pathways. Selective uncoupling of TCR signalling and sparing of antigen-specific RasuERK activation would contribute significantly to this phenotype by promoting cell survival and the persistence of activated cells in inflamed joints. Concluding remarks Confirming unequivocally that hyporesponsive T cells are capable of promoting the inflammatory process in RA is a priority because an understanding of the precise mechanisms involved could provide a molecular basis for testing hitherto unexplored immunotherapeutic 727 strategies. Studying the effects of suppressing the Rasu ERK pathway is just one example. To date, the assumption has been that T cells in RA are harmful, because effector responses are sustained by chronic activation by tissue-specific antigens presented by disease-associated HLA class II molecules (Fig. 1). The assumption that synovial T cells are harmful is probably correct, but perhaps for the wrong reasons. For example, T-celltargeted strategies have focused almost exclusively on depressing T-cell function further. The results have been disappointing w105, 106x, perhaps because the calciumucalcineurin pathway and transactivation of nuclear factor of activated T cells (NFAT) are already profoundly depressed in cytokine-activated T cells. However, results from several laboratories, including my own, suggest that therapeutic strategies aimed at restoring the function of subsets of T cells should now be considered. A major challenge will be to identify which specific T-cell subsets in vivo are hyporesponsive. For example, if these subsets include regulatory T cells, such as IL-10producing Tr1-like CD4+ cells or IL-16-producing CD8+ T cells w107, 108x, restoring TCR responsiveness could suppress the inflammatory activities of offending effector T-helper cell subsets, macrophages and fibroblasts. This therapeutic approach is entirely in line with the thesis proposing that susceptibility to autoimmunity arises through failure of the adaptive immune system to regulate the inflammatory response. In the short term, restoring T-cell responsiveness towards ‘normal’ (but not beyond) could be achieved by a combination of immunotherapeutic approaches targeting the peptide or altered peptide ligand specificities of regulatory T cells (which could be determined in HLA class II-transgenic mice as described above) together with anti-TNF. This approach would provide anti-inflammatory cover, while at the same time enhancing responsiveness to the therapeutic peptide by restoring TCR signalling pathways. A detailed knowledge of the specific TCR signalling defects could provide clues as to how best to monitor such therapy, and how to avoid rebound T-cell hyper-reactivity and its inevitable consequences, systemic autoimmune disease and acute cytokine release syndromes. Anti-TNF in combination with non-depleting anti-CD4 or anti-CD3 monoclonal antibody could have similar beneficial therapeutic effects w109x. If, on the other hand, this hypothesis is incorrect and T-cell hyporesponsiveness turns out to be beneficial to the disease process, then a more precise understanding of how the inflammatory process uncouples signalling pathways in cytokine-activated T cells would greatly facilitate the development of novel immunosuppressive agents. Acknowledgements I gratefully acknowledge Professors Marc Feldmann, David Wallach and Hugh McDevitt, in whose laboratories 728 A. P. Cope much of the work was undertaken, my mentor Professor Sir Ravinder Maini for continued support, and members of the Cope Laboratory who are continuing with this work. These studies would not have been possible without the support of the Wellcome Trust over the last 12 years, and the Arthritis Research Campaign. References 1. Mason D. A very high level of crossreactivity is an essential feature of the T-cell receptor. Immunol Today 1998; 19:395–404. 2. Mason D, Powrie F. Control of immune pathology by regulatory T cells. Curr Opin Immunol 1998;10:649–55. 3. Germain RN, Stefanova I. The dynamics of T cell receptor signaling: complex orchestration and the key roles of tempo and cooperation. Annu Rev Immunol 1999; 17:467–522. 4. Winchester R. The molecular basis of susceptibility to rheumatoid arthritis. Adv Immunol 1994;56:389–466. 5. Deighton CM, Walker DJ, Griffiths ID, Roberts DF. The contribution of HLA to rheumatoid arthritis. Clin Genet 1989;36:178–82. 6. Nepom GT. Major histocompatibility complex-directed susceptibility to rheumatoid arthritis. Adv Immunol 1998;68:315–52. 7. Stastny P. Association of the B-cell alloantigen DRw4 with rheumatoid arthritis. N Engl J Med 1978;298:869–71. 8. Gregerson PK, Silver J, Winchester RJ. The shared epitope hypothesis: an approach to understanding the molecular genetics of susceptibility to rheumatoid arthritis. Arthritis Rheum 1987;30:1205–13. 9. Wordsworth BP, Lanchbury JS, Sakkas LI, Welsh KI, Panayi GS, Bell JI. HLA-DR4 subtype frequencies in rheumatoid arthritis indicate that DRB1 is the major susceptibility locus within the HLA class II region. Proc Natl Acad Sci USA 1989;86:10049–53. 10. Nepom GT, Byers P, Seyfried C et al. HLA genes associated with rheumatoid arthritis. Identification of susceptibility alleles using specific oligonucleotide probes. Arthritis Rheum 1989;32:15–21. 11. Ollier W, Thomson W. Population genetics of rheumatoid arthritis. Rheum Dis Clin North Am 1992;18:741–59. 12. Weyand CM, McCarthy TG, Goronzy JJ. Correlation between disease phenotype and genetic heterogeneity in rheumatoid arthritis. J Clin Invest 1995;95:2120–6. 13. Young CL, Adamson TC, Vaughan JH, Fox RI. Immunohistologic characterization of synovial membrane lymphocytes in rheumatoid arthritis. Arthritis Rheum 1984;27:32–9. 14. Wucherpfennig KW, Strominger JL. Selective binding of self peptides to disease-associated major histocompatibility complex (MHC) molecules: a mechanism for MHClinked susceptibility to human autoimmune diseases. J Exp Med 1995;181:1597–601. 15. Hammer J, Gallazzi F, Bono E et al. Peptide binding specificity of HLA-DR4 molecules: correlation with rheumatoid arthritis association. J Exp Med 1995;181:1847–55. 16. Penzotti JE, Nepom GT, Lybrand TP. Use of T cell receptoruHLA-DRB1*04 molecular modeling to predict site-specific interactions for the DR shared epitope associated with rheumatoid arthritis. Arthritis Rheum 1997;40:1316–26. 17. Walser-Kuntz DR, Weyand CM, Weaver AJ, O’Fallon WM, Goronzy JJ. Mechanisms underlying the formation of the T cell receptor repertoire in rheumatoid arthritis. Immunity 1995;2:597–605. 18. Fugger L, Michie SA, Rulifson I, Lock CB, SønderstrupMcDevitt G. Expression of HLA-DR4 and human CD4 transgenes in mice determines the variable region b-chain T-cell repertoire and mediates an HLA-DR-restricted immune response. Proc Natl Acad Sci USA 1994;91:6151–5. 19. Woods A, Chen HY, Trumbauer ME, Sirotina A, Cummings R, Zaller DM. Human major histocompatibility complex class II-restricted T cell responses in transgenic mice. J Exp Med 1994;180:173–81. 20. Yeung RSM, Penninger JM, Kundig TM et al. Human CD4–major histocompatibility complex class II (DQw6) transgenic mice in an endogenous CD4uCD8-deficient background: reconstitution of phenotype and humanrestricted function. J Exp Med 1994;180:1911–20. 21. Taneja V, David CS. HLA transgenic mice as humanized mouse models of disease and immunity. J Clin Invest 1998;101:921–6. 22. Sonderstrup G, Cope AP, Patel S et al. HLA class II transgenic mice: models of the human CD4+ T-cell immune response. Immunol Rev 1999;172:335–43. 23. Nabozny GH, Baisch JM, Cheng S et al. HLA-DQ8 transgenic mice are highly susceptible to collagen-induced arthritis: a novel model for human polyarthritis. J Exp Med 1996;183:27–37. 24. Rosloniec EF, Brand DD, Myers LK et al. Induction of autoimmune arthritis in HLA-DR4 (DRB1*0401) transgenic mice by immunization with human and bovine type II collagen. J Immunol 1998;160:2573–8. 25. Patel SD, Cope AP, Congia M et al. Identification of immunodominant T cell epitopes of human glutamic acid decarboxylase 65 using HLA-DR(a1*0101, b1*0401) transgenic mice. Proc Natl Acad Sci USA 1997;95:8082–7. 26. Cosgrove D, Gray D, Dierich A et al. Mice lacking MHC class II molecules. Cell 1991;66:1051–66. 27. Cope AP, Patel SD, Hall FC et al. T cell responses to a human cartilage autoantigen in the context of rheumatoid arthritis associated and non-associated HLA-DR4 alleles. Arthritis Rheum 1999;42:1497–507. 28. Hakala BE, White C, Recklies AD. Human cartilage gp-39, a major secretory product of articular chondrocytes and synovial cells, is a mammalian member of a chitinase protein family. J Biol Chem 1993;268:25803–10. 29. Hu B, Trinh K, Figueira WF, Price PA. Isolation and sequence of a novel human chondrocyte protein related to mammalian members of the chitinase protein family. J Biol Chem 1996;271:19415–20. 30. Johansen JS, Jensen HS, Price PA. A new biochemical marker for joint injury. Analysis of YKL-40 in serum and synovial fluid. Br J Rheumatol 1993;32:949–55. 31. Cope AP, Sonderstrup G. Evaluating candidate autoantigens in rheumatoid arthritis. Springer Semin Immunopathol 1998;20:23–39. 32. Cope AP. Exploring the pathogenesis of rheumatoid arthritis in transgenic and mutant mice. In: Theofilopoulos A, ed. Current directions in autoimmunity. San Diego: Scripps Research Institute, 2001. pp. 64–93. 33. Penzotti JE, Doherty D, Lybrand TP, Nepom GT. A structural model for TCR recognition of the HLA class II shared epitope sequence implicated in susceptibility to rheumatoid arthritis. J Autoimmun 1996;9:287–93. Immunity and inflammation in chronic inflammatory arthritis 34. Steere AC, Grodzicki RL, Kornblatt AN et al. The spirochaetal etiology of Lyme disease. N Engl J Med 1993;308:733–40. 35. Steere AC, Dwyer ED, Winchester R. Association of chronic Lyme arthritis with HLA-DR4 and HLA-DR2 alleles. N Engl J Med 1990;323:219–23. 36. Lengl-Janssen B, Strauss AF, Steere AC, Kamradt T. The T helper cell response in Lyme arthritis: Differential recognition of Borrelia burgdorferi outer surface protein A (OspA) in patients with treatment-resistant or treatmentresponsive Lyme arthritis. J Exp Med 1994;180:2069–78. 37. Kamradt T, Lengl-Janssen B, Strauss AF, Bansal G, Steere AC. Dominant recognition of a Borrelia burgdorferi outer surface protein A-peptide by T helper cells in patients with treatment-resistant Lyme arthritis. Infect Immun 1996;64:1284–9. 38. Maier B, Molinger M, Cope AP et al. Multiple crossreactive self-ligands for Borrelia burgdorferi-specific HLADR4-restricted T cells. Eur J Immunol 2000;30:448–57. 39. Wucherpfennig KW, Strominger JL. Molecular mimicry in T cell-mediated autoimmunity: viral peptides activate human T cell clones specific for myelin basic protein. Cell 1995;80:695–705. 40. Hemmer B, Vergelli M, Gran B et al. Predictable TCR antigen recognition based on peptide scans leads to the identification of agonist ligands with no sequence homology. J Immunol 1998;160:3631–6. 41. Grogan JL, Kramer A, Nogai A et al. Cross-reactivity of myelin basic protein-specific T cells with multiple microbial peptides: experimental autoimmune encephalomyelitis induction in TCR transgenic mice. J Immunol 1999;163:3764–70. 42. Dessen A, Lawrence CM, Cupo S, Zaller DM, Wiley DC. X-ray crystal structure of HLA-DR4 (DRA*0101, DRB1*0401) complexed with a peptide from human collagen II. Immunity 1997;7:473–81. 43. Patil NS, Hall FC, Drover S et al. Autoantigenic HCgp39 epitopes are presented by the HLA-DM-dependent presentation pathway in human B cells. J Immunol 2001; 166:33–4. 44. Hall FC, Rabinowitz JD, Busch R et al. Relationship between kinetic stability and immunogenicity of HLADR4/peptide complexes. Eur J lmmunol 2002;32:662–70. 45. Todd JA, Bell JI, McDevitt HO. HLA-DQ beta gene contributes to susceptibility and resistance to insulindependent diabetes mellitus. Nature 1987;329:599–604. 46. Feldmann M, Brennan FM, Maini RN. Role of cytokines in rheumatoid arthritis. Annu Rev Immunol 1996;14:397–440. 47. Buchan G, Barrett K, Turner M, Chantry D, Maini RN, Feldmann M. Interleukin-1 and tumour necrosis factor mRNA expression in rheumatoid arthritis: prolonged production of IL-1a. Clin Exp Immunol 1988;73:449–55. 48. Saxne T, Palladino MA Jr, Heinegard D, Talal N, Wollheim FA. Detection of tumor necrosis factor alpha but not tumor necrosis factor beta in rheumatoid arthritis synovial fluid and serum. Arthritis Rheum 1988;31:1041–5. 49. Hopkins SJ, Humphreys M, Jayson MI. Cytokines in synovial fluid. I. The presence of biologically active and immunoreactive IL-1. Clin Exp Immunol 1988;72:422–7. 50. Deleuran BW, Chu CQ, Field M et al. Localization of tumor necrosis factor receptors in the synovial tissue and cartilage–pannus junction in patients with rheumatoid arthritis. Implications for local actions of tumor necrosis factor alpha. Arthritis Rheum 1992;35:1170–8. 51. Brennan FM, Gibbons DL, Mitchell T, Cope AP, Maini RN, Feldmann M. Enhanced expression of tumor 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 729 necrosis factor receptor mRNA and protein in mononuclear cells isolated from rheumatoid arthritis synovial joints. Eur J Immunol 1992;22:1907–12. Chu CQ, Field M, Feldmann M, Maini RN. Localization of tumor necrosis factor alpha in synovial tissues and at the cartilage–pannus junction in patients with rheumatoid arthritis. Arthritis Rheum 1991;34:1125–32. Brennan FM, Chantry D, Jackson A, Maini R, Feldmann M. Inhibitory effect of TNF alpha antibodies on synovial cell interleukin-1 production in rheumatoid arthritis. Lancet 1989;2:244–7. Cope AP, Aderka D, Doherty M et al. Increased levels of soluble tumor necrosis factor receptors in the sera and synovial fluid of patients with rheumatic diseases. Arthritis Rheum 1992;35:1160–9. Cope AP, Londei M, Chu NR et al. Chronic exposure to tumor necrosis factor (TNF) in vitro impairs the activation of T cells through the T cell receptoruCD3 complex: reversal in vivo by anti-TNF antibodies in patients with rheumatoid arthritis. J Clin Invest 1994;94:749–60. Cope AP, Aderka D, Wallach D et al. Soluble TNF receptor production by activated T lymphocytes: differential effects of acute and chronic exposure to TNF. Immunology 1995;84:21–30. Cope AP, Liblau RS, Yang XD et al. Chronic tumor necrosis factor alters T cell responses by attenuating T cell receptor signaling. J Exp Med 1997;185:1573–84. Yokota S, Geppert T, Lipsky P. Enhancement of antigenand mitogen-induced human T lymphocyte proliferation by tumor necrosis factor-a. J Immunol 1988;140:531–6. Cush JJ, Lipsky PE. Phenotypic analysis of synovial tissue and peripheral blood lymphocytes isolated from patients with rheumatoid arthritis. Arthritis Rheum 1988;31:1230–8. Emery P, Panayi GS, Nouri AME. Interleukin-2 reverses deficient cell-mediated immune responses in rheumatoid arthritis. Clin Exp Immunol 1984 1984;57:123–9. Malone DG, Wahl SM, Tsokos M, Cattell H, Decker JL, Wilder RL. Immune function in severe, active rheumatoid arthritis. A relationship between peripheral blood mononuclear cell proliferation to soluble antigens and synovial tissue immunohistologic characteristics. J Clin Invest 1984;74:1173–85. Maurice MM, Nakamura H, van der Voort EA et al. Evidence for the role of an altered redox state in hyporesponsiveness of synovial T cells in rheumatoid arthritis. J Immunol 1997;158:1458–65. Isomäki P, Panesar M, Annenkov A et al. Prolonged exposure to TNF induces reversible and non-deletional T cell hyporesponsiveness by targeting TCRz and expression of the TCRuCD3 complex. J Immunol 2001;166:5495–507. Klausner RD, Lippincott-Schwartz J, Bonifacino JS. The T cell antigen receptor: insights into organelle biology. Annu Rev Cell Biol 1990;6:403–31. Weiss A, Littman DR. Signal transduction by lymphocyte antigen receptors. Cell 1994;76:263–74. Bruyns E, Marie-Cardine A, Kirchgessner H et al. T cell receptor (TCR) interacting molecule (TRIM), a novel disulfide-linked dimer associated with the TCR-CD3-zeta complex, recruits intracellular signaling proteins to the plasma membrane. J Exp Med 1998;188:561–75. Kirchgessner H, Dietrich J, Scherer J et al. The transmembrane adaptor protein TRIM regulates T cell receptor (TCR) expression and TCR-mediated signaling via an association with the TCR zeta chain. J Exp Med 2001;193:1269–84. 730 A. P. Cope 68. Zhang W, Sloan-Lancaster J, Kitchen J, Trible RP, Samelson LE. LAT: the ZAP-70 tyrosine kinase substrate that links T cell receptor to cellular activation. Cell 1998;92:83–92. 69. Finco TS, Kadlecek T, Zhang W, Samelson LE, Weiss A. LAT is required for TCR-mediated activation of PLCgamma1 and the Ras pathway. Immunity 1998;9:617–26. 70. Kang SM, Beverly B, Tran AC, Brorson K, Schwartz RH, Lenardo MJ. Transactivation by AP-1 is a molecular target of T cell clonal anergy. Science 1992;257:1134–8. 71. Schwartz RH. T cell clonal anergy. Curr Opin Immunol 1997;9:351–7. 72. Maurice MM, Lankester AC, Bezemer AC et al. Defective TCR-mediated signaling in synovial T cells in rheumatoid arthritis. J Immunol 1997;159:2973–8. 73. Gringhuis SI, Leow A, Papendrecht-Van Der Voort EA, Remans PH, Breedveld FC, Verweij CL. Displacement of linker for activation of T cells from the plasma membrane due to redox balance alterations results in hyporesponsiveness of synovial fluid T lymphocytes in rheumatoid arthritis. J Immunol 2000;164:2170–9. 74. Allen ME, Young SP, Michell RH, Bacon PA. Altered T lymphocyte signaling in rheumatoid arthritis. Eur J Immunol 1995;25:1547–54. 75. Carruthers DM, Arrol HP, Bacon PA, Young SP. Dysregulated intracellular Ca2+ stores and Ca2+ signaling in synovial fluid T lymphocytes from patients with chronic inflammatory arthritis. Arthritis Rheum 2000;43:1257–65. 76. Cope AP. Regulation of autoimmunity by proinflammatory cytokines. Curr Opin Immunol 1998;10:669–76. 77. Cope AP, Ettinger R, McDevitt HO. The role of TNFa and related cytokines in the development and function of the autoreactive T cell repertoire. Res Immunol 1997; 148:307–12. 78. Jacob CO, McDevitt HO. Tumour necrosis factor-a in murine autoimmune ‘lupus’ nephritis. Nature 1988; 331:356–8. 79. Satoh J, Seino H, Abo T et al. Recombinant human tumor necrosis factor a suppresses autoimmune diabetes in non-obese diabetic mice. J Clin Invest 1989;84:1345–8. 80. Jacob CO, Aiso S, Michie SA, McDevitt HO, AchaOrbea H. Prevention of diabetes in nonobese diabetic mice by tumor necrosis factor (TNF): similarities between TNF-alpha and interleukin 1. Proc Natl Acad Sci USA 1990;87:968–72. 81. Liu J, Marino MW, Wong G et al. TNF is a potent anti-inflammatory cytokine in autoimmune-mediated demyelination. Nat Med 1998;4:78–83. 82. Zhou T, Edwards CK, Yang P, Wang Z, Bluethmann H, Mountz JD. Greatly accelerated lymphadenopathy and autoimmune disease in lpr mice lacking tumor necrosis factor receptor 1. J Immunol 1996;156:2661–5. 83. Probert L, Eugster HP, Akassoglou K et al. TNFR1 signalling is critical for the development of demyelination and the limitation of T-cell responses during immunemediated CNS disease. Brain 2000;123:2005–19. 84. Kassiotis G, Kollias G. Uncoupling the proinflammatory from the immunosuppressive properties of tumor necrosis factor (TNF) at the p55 TNF receptor level: implications for pathogenesis and therapy of autoimmune demyelination. J Exp Med 2001;193:427–34. 85. Lai N-S, Lan J-L, Yu C-L, Lin R-H. Role of tumor necrosis factor-a in the regulation of activated synovial T cell growth: downregulation of synovial T cells in rheumatoid arthritis. Eur J Immunol 1995;25:3243–8. 86. Lorenz HM, Antoni C, Valerius T et al. In vivo blockade of TNF-alpha by intravenous infusion of a chimeric monoclonal TNF-alpha antibody in patients with rheumatoid arthritis. Short term cellular and molecular effects. J Immunol 1996;156:1646–53. 87. Maurice MM, van der Graaff WL, Leow A, Breedveld FC, van Lier RA, Verweij CL. Treatment with monoclonal anti-tumor necrosis factor alpha antibody results in an accumulation of Th1 CD4+ T cells in the peripheral blood of patients with rheumatoid arthritis. Arthritis Rheum 1999;42:2166–73. 88. Berg L, Lampa J, Rogberg S, van Vollenhoven R, Klareskog L. Increased peripheral T-cell reactivity to microbial antigens and collagen type II in rheumatoid arthritis after treatment with soluble TNF-a receptors. Ann Rheum Dis 2001;60:133–9. 89. Elliott MJ, Maini RN, Feldmann M et al. Randomised double-blind comparison of chimeric monoclonal antibody to tumour necrosis factor alpha (cA2) versus placebo in rheumatoid arthritis. Lancet 1994;344:1105–10. 90. Moreland LW, Baumgartner SW, Schiff MH et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)–Fc fusion protein. N Engl J Med 1997;337:141–7. 91. Lipsky PE, van der Heijde DM, St Clair EW et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study Group. N Engl J Med 2000;343:1594–602. 92. Targan SR, Hanauer SB, van Deventer SJ et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s Disease cA2 Study Group. N Engl J Med 1997;337:1029–35. 93. Present DH, Rutgeerts P, Targan S et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med 1999;340:1398–405. 94. Taylor PC, Peters AM, Paleolog E et al. Reduction of chemokine levels and leukocyte traffic to joints by tumor necrosis factor alpha blockade in patients with rheumatoid arthritis. Arthritis Rheum 2000;43:38–47. 95. Paleolog EM, Young S, Stark AC, McCloskey RV, Feldmann M, Maini RN. Modulation of angiogenic vascular endothelial growth factor by tumor necrosis factor alpha and interleukin-1 in rheumatoid arthritis. Arthritis Rheum 1998;41:1258–65. 96. Hommes DW, van Deventer SJ. Anti- and proinflammatory cytokines in the pathogenesis of tissue damage in Crohn’s disease. Curr Opin Clin Nutr Metab Care 2000;3:191–5. 97. Charles PJ, Smeenk RJ, De Jong J, Feldmann M, Maini RN. Assessment of antibodies to double-stranded DNA induced in rheumatoid arthritis patients following treatment with infliximab, a monoclonal antibody to tumor necrosis factor alpha: findings in open-label and randomized placebo-controlled trials. Arthritis Rheum 2000;43:2383–90. 98. Salmon M, Scheel-Toellner D, Huissoon AP et al. Inhibition of T cell apoptosis in the rheumatoid synovium. J Clin Invest 1997;99:439–46. 99. Lombardi G, Dunne PJ, Scheel-Toellner D et al. Type 1 IFN maintains the survival of anergic CD4+ T cells. J Immunol 2000;165:3782–9. 100. Sebbag M, Parry SL, Brennan FM, Feldmann M. Cytokine stimulation of T lymphocytes regulates their capacity to induce monocyte production of tumor Immunity and inflammation in chronic inflammatory arthritis 101. 102. 103. 104. necrosis factor-alpha, but not interleukin-10: possible relevance to pathophysiology of rheumatoid arthritis. Eur J Immunol 1997;27:624–32. Isler P, Vey E, Zhang JH, Dayer JM. Cell surface glycoproteins expressed on activated human T cells induce production of interleukin-1 beta by monocytic cells: a possible role of CD69. Eur Cytokine Netw 1993;4:15–23. Lacraz S, Isler P, Vey E, Welgus HG, Dayer JM. Direct contact between T lymphocytes and monocytes is a major pathway for induction of metalloproteinase expression. J Biol Chem 1994;269:22027–33. McInnes IB, Leung BP, Sturrock RD, Field M, Liew FY. Interleukin-15 mediates T cell-dependent regulation of tumor necrosis factor-alpha production in rheumatoid arthritis. Nat Med 1997;3:189–95. Weyand CM, Goronzy JJ, Takemura S, Kurtin PJ. Interactions between T cells and B cells in rheumatoid arthritis. Arthritis Res 2000;2:457–63. 731 105. Breedfeld FC. Monoclonal antibodies to CD4. Rheum Dis Clin North Am 1998;24:567–78. 106. Rep MH, van Oosten BW, Roos MT. Treatment with CD4 depleting antibodies results in preferential loss of circulating naı̈ve T cells but does not affect IFN gammasecreting Th1 cells in humans. J Clin Invest 1997;99:2225–31. 107. Morita Y, Yamamura M, Kawashima M et al. Flow cytometry single-cell analysis of cytokine production by CD4+ T cells in synovial tissue and peripheral blood from patients with rheumatoid arthritis. Arthritis Rheum 1998;41:1660–76. 108. Klimiuk PA, Goronzy JJ, Weyand CM. IL-16 as an anti-inflammatory cytokine in rheumatoid arthritis. J Immunol 1999;162:4293–9. 109. Williams RO, Mason LJ, Feldmann M, Maini RN. Synergy between anti-CD4 and anti-tumor necrosis factor in the amelioration of established collagen-induced arthritis. Proc Natl Acad Sci USA 1994;91:2762–6.



















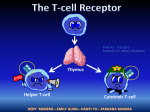
![item[`#file`]](http://s1.studyres.com/store/data/010648307_1-07b372d948ab0500f7fd02abfa5f4701-150x150.png)






