Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Saturated fat and cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Jatene procedure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Electrocardiography wikipedia , lookup
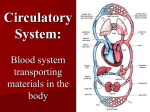
Circulatory System major connection between external and internal environment: everything going in or out of body must go through the circulatory system to get to where its going two major transport systems in body: circulatory (cardiovascular) system lymphatic system circulatory system works in conjunction with lymphatic system = an open system circulatory system consists of “plumbing” and “pumps”: 1. blood travels within a closed system of vessels; never leaves vessels 2. has muscular pump that helps to move it is one of first organ systems to appear in developing embryo heart is beating by 4th week The Heart about size and shape of closed fist beats >100,000 x’s/day (~103,680b/d) Histology of Heart cardiac muscle fibers: striated myofibrils are highly ordered 1 nucleus branched cells T tubules and SR less developed than skeletal mm separated by intercalated discs myocardium behaves as single unit but atrial muscles separated from ventricular muscles by conducting tissue sheath atria contract separately from ventricles mitochondria account for 25% of cardiac muscle cells (compared to 2% of skeletal muscle cells) Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 1 greater dependence on oxygen than skeletal muscles can’t build up much oxygen debt more adaptable in nutrient use; can use: glucose fatty acids (preferred) lactic acid long contraction phase and long refractory period almost as long as contraction phase (~250ms vs 1-2 ms in skeletal muscle) prevents tetanus Conducting System heart has some specialized fibers that are modified cardiac muscle cells don’t contract; fire impulses that coordinate contraction of heart muscle innervated by autonomic NS consists of: SA Node intrinsic rhythm 70-75 beats/min initiates stimulus that causes atria to contract (but not ventricles directly due to separation) AV Node picks up stimulus from SA Node if SA Node is not functioning it can act as a pacemaker =ectopic pacekmaker (usually slower intrinsic rhythm) AV Bundle (Bundle of His) connected to AV Node takes stimulus from AV Node to ventricles Purkinje Fibers takes impulse from AV Bundle out to cardiac mucscle fibers of ventricles causing ventricles to contract the heart conducting system generates a small electrical current that can be picked up by an electrocardiograph =electrocardiogram (ECG; EKG) ECG is a record of the electrical activity of the conducting system Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 2 body is a good conductor of electricity (lots of salts) potential changes at body’s surface are picked up by 12 leads ECG is NOT a record of heart contractions R P T Q S P wave = passage of current through atria from SA Node atrial depolarization QRS wave = passage of current through ventricles from AV Node – AV Bundle – Purkinje Fibers ventricular depolarization T wave = repolarization of ventricles (atrial repolarization is masked by QRS) by measuring intervals between these waves can get idea of how rapidly the impulses are being conducted amplitude of waves also gives info on condition of conducting system and myocardium Abnormalities of ECG’s = arrhythmias 1. bradycardia (<60 bpm) decrease in body temperature some drugs (eg digitalis) overactive parasympathetic system endurance athletes 2. tachycardia (>100 bpm) increased body temperature fever emergencies, stress activation of sympathetic NS some drugs may promote fibrillation Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 3 3. flutter short bursts of 200-300 bpm but coordinated 4. fibrillation rapid, uncoordinated contractions of individual muscle cells atrial fibrillation is OK (since it only contributes 20% of blood to heart beat) ventricular fibrillation is lethal electrical shock used to defibrillate and recoordinate contractions 5. AV Node Block normal P - Q interval = 0.12 – 0.20 seconds changes indicate damage to AV Node difficulty in signal getting past AV Node 1st º block: >0.20 seconds 2nd º block: AV Node damaged so only so wave passes through ventricles only after every 2-4 P waves rd 3 º block: (complete block) no atrial waves can pass through ventricle paced by different ectopic pacemaker therefore beat abnormally slow Cardiac Cycle 1 complete heartbeat (takes ~ 0.8 seconds) consists of: systole contraction of each chamber diastole relaxation of each chamber two atria contract simultaneously as they relax, ventricles contract ventricular systole (atrial diastole) = 0.3 sec ventricular diastole = 0.5 sec relation of ECG to cardiac cycle contraction and relaxation of ventricles produces characteristic heart sounds lub-dub lub = systolic sound contraction of ventricles and closing of AV valves dub = diastolic sound shorter, sharper sound Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 4 ventricles relax and SL valves close abnormal sounds: “murmurs” defective valves congenital rheumatic (strep antibodies) septal defects relationship of cardiac cycle, ECG, heart sounds, pressure and volume Cardiac Output CO = = = Heart RateX Stroke volume 75b/m X 70ml/b 5250 ml/min (=5.25 l/min) ~ normal blood volume A. Heart Rate: innervated by autonomic branches to SA and AV nodes control center in medulla (cardiac center) receives sensory info from: Baroreceptors (stretch) in aorta and carotid sinus increased stretch slower Chemoreceptors monitor carbon dioxide and pH more CO2 or lower pH faster Other Factors that Affect Heartrate: a. hormones epinephrin faster acetylcholine slower thyroxine faster b. drugs atropine (from belladonna) anticholinergic drug faster digitalis slows, but greater force c. ions low Calcium slower high Calcium faster Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 5 spastic heart contractions high Sodium blocks Ca++ slows high Potassium faster may cause cardiac arrest d. temperature heat increases heart rate e. age younger = faster, slows with age f. gender women = faster (72-80 bpm) men = slower (64-72 bpm) g. exercise increases during exercise also heart beats slower in physically fit h. emotions fear, anxiety, anger increase HR depression, grief reduce HR any marked, persistent changes in rate may signal cardiovascular disease B. Stroke Volume: healthy heart pumps ~60% of blood in it normal SV = ~70 ml SV = EDV (end diastolic vol) – ESV (end systolic vol) affected by: 1. mean blood (arterial)pressure back pressure 2. condition of heart tissue eg. heart contractility indicates amt of damage 3. venous return/ amount of stretch Starling’s Law: within physiological limits the heart pumps all the blood that returns to it without undue damming of blood in veins. intrinsic regulatory mechanisms permit adaptation of the Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 6 heart to varying rates of venous return. >stretch = >strength of contraction 4. blood viscosity (>RBC’s, dehydration, blood proteins) Human Anatomy & Physiology: Cardiovascular System; Ziser, 2004 7