Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Molecular mimicry wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Innate immune system wikipedia , lookup
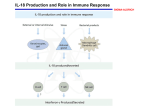
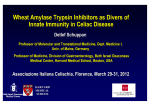
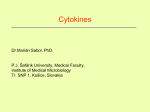
Rheumatology 2008;47:1269–1277 Advance Access publication 10 July 2008 doi:10.1093/rheumatology/ken257 Signalling, inflammation and arthritis Crossed signals: the role of interleukin-15 and -18 in autoimmunity H. P. Carroll1, V. Paunović1 and M. Gadina1 Several cytokines are involved in the complex processes ultimately leading to autoimmune diseases. In a preceding review, we have already discussed the role of the IL-12 and -17 families of cytokines. This review is focused on IL-15 and -18. Both these molecules have pro-inflammatory activity and act on many cell types and because of their broad spectrum of activity they play an important role in autoimmunity and disease pathogenesis. Their biological activity is ultimately regulated by the signalling cascades set into motion within their target cells. In this second review, we will, once again, describe the signal transduction pathways activated by these two cytokines and focus on how this relates to the pathogenesis of autoimmune diseases. We will also describe some of the therapeutic approaches that are being investigated to curtail the pro-inflammatory activities of these two molecules. KEY WORDS: Inflammation, Cytokines, Autoimmunity, Rheumatoid arthritis, Signal transduction, Janus Kinase–Signal Transducers and Activators of Transcription pathway, Nuclear factor-B. exists as two alternatively spliced isoforms, which encode for two forms of IL-15 protein, a secreted form (48aa) [3] and an intracellular form (non-secretable form) (21aa) which is localized to both cytoplasmic and nuclear compartments [14]. IL-15 production is induced by a variety of exogenous factors, including double-stranded RNA, Type I IFN, lipopolysaccharide, UV irradation, a number of viruses including, herpes simplex virus and respiratory syncitial virus, and fungal and bacterial agents such as Candida albicans, Escherichia coli and Staphylococcus aureus [15–18]. Introduction The inflammatory reaction observed in autoimmune disease involves both cellular and soluble players. Pro-inflammatory cytokines such as the members of the IL-12 and -17 families, which we have discussed in our previous review [1], are undoubtedly at the centre of the processes which result in unregulated activation of immune cells. On the other hand, other immunoregulatory cytokines have been demonstrated to have a very important role. In particular, IL-15, which is critical for the regulation of lymphocyte homeostasis as well as NK cell development, and IL-18, a potent inducer of IFN- and TNF have also been shown to have a major role in the events leading to an excessive inflammatory response. In this review, we have focused our attention to IL-15 and -18 discussing their complex biological activity and their signalling cascades in the normal immune response and in diseases, as well as some of the current therapeutic approaches targeting these two cytokines. IL-15: receptor and signalling IL-15 binds to a heterotrimeric receptor that comprises the same chain (IL-2R, -15R and CD122) and the common chain ( c; CD132) as the IL-2 receptor. The IL-15 receptor also includes a cytokine-specific chain, IL-15R chain. IL-15R complex is expressed on monocytes, DCs, NK, T cells and fibroblasts [19, 20] (Fig. 1). IL-15R mRNA is expressed in a number of cell types and tissues, including T, B cells, macrophages, kidney and heart [21]. IL-15R binds IL-15 with high affinity [22]. It has a short cytoplasmic domain and an extracellular region containing one sushi domain (a highly conserved protein binding domain also known as a glycoprotein 1 motif), which is critical for IL-15 binding [23–25]. IL-15R not only exists as a membrane-bound receptor but also in soluble form [26, 27]. The transmembrane IL-15R undergoes specific proteolytic cleavage to generate a soluble 26 kDa protein in mouse and 42 kDa protein in humans [26, 27]. In mice, the generation of soluble form of IL-15R (sIL-15R) is produced by cleavage of transmembrane IL-15R by TNFconverting enzyme [26]. Shedding of the soluble form of the receptor may act as a further checkpoint for IL-15 activity. IL-15 has only a single binding site for interaction with IL-15R. Therefore, the availability of free IL-15 will be reduced by the presence of this high-affinity, soluble receptor [28]. Competition with the membrane-bound receptor could result in reduced IL-15R signalling and therefore reduced biological activity of IL-15. This is supported by in vivo evidence which suggests that administration of sIL-15R results in the inhibition of NK cell proliferation [29] and antigen-specific T-cell responses [30]. Conversely, it has recently been reported that sIL-15R can convert IL-15 to a superagonist that enhances the IL-15 responses in CD8þ and NK cells both in vivo and in vitro [28]. It is speculated that upon sIL-15R binding to IL-15 a conformational change IL-15 IL-15: structure and production IL-15 is a 14–15 kDa member of the four -helix cytokine family with structural similarities to IL-2 [2, 3]. Like IL-2, IL-15 stimulates the proliferation of CD4þ and CD8þ T cells, immunoglobulin M (IgM) or CD40L-treated B cells, as well as the generation and persistence of NK cells [4–9]. However, IL-2 and -15 exhibit major differences in the control of their synthesis and secretion [5, 10]. IL-2 production is tightly regulated during transcription, whereas, IL-15 mRNA is constitutively expressed by a wide variety of human tissues and cell types, including activated monocytes, macrophages, dendritic cells (DCs), osteoclasts and fibroblasts of the spleen, gingiva and skin [3, 5, 11–13]. Interestingly, the patterns of IL-15 protein and mRNA expression differ greatly, indicating tight control of protein production at both translational and post-translational levels. IL-15 mRNA 1 Centre for Cancer Research and Cell Biology, Queen’s University Belfast, Belfast, UK. Submitted 1 February 2008; revised version accepted 13 June 2008. Correspondence to: H. P. Carroll, Centre for Cancer Research and Cell Biology, Queen’s University Belfast, Belfast BT9 7BL, Northern Ireland, UK. E-mail: [email protected] 1269 ß The Author 2008. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: [email protected] 1270 H. P. Carroll et al. FIG. 1. Schematic representation of the IL-15 receptor and IL-18 receptor complexes and summary of the signal transduction events following ligand binding. The IL-15R complex consists of IL-2R, -2R and -15R. Upon ligand binding JAK1 and JAK3 are recruited to the - and -cchains, respectively. STAT3 and STAT5 dock to phosphorylated IL-2R via the SH2 domains are tyrosine phosphorylated, form homo/heterodimers and translocate to the nucleus where they activate gene transcription. The IL-15R chain recruits TRAF 2 leading to the activation of NF-B. The sIL-15R binds to IL-15 with high affinity. In mast cells, IL-15RX binds with high affinity to IL-15 and results in the activation of JAK2 or Tyk2 even in the absence of the IL-2R and -2R chains leading to the activation of STAT5 or STAT6 and up-regulation of Bcl-XL and c-Myc expression. IL-18 binds to the IL-18R bringing the two chains of the IL-18 in close proximity. The TIR domains recruit various kinases ultimately leading to the activation of NF-B and the p38 MAP kinase pathway. IL-18 binding may be inhibited by the presence of IL-18BP that binds to IL-18 with high affinity. occurs in the cytokine, which enhances its interaction with the c receptor. Although IL-15 was originally identified as a soluble cytokine in tissue culture supernatant of a simian renal epithelial cell line CV-1/EBNA [3], it has proven difficult to detect in biological fluids from healthy individuals despite widespread mRNA expression. In fact, evidence now indicates that IL-15 is not normally secreted but forms stable high-affinity complexes with IL-15R on the cell surface of antigen presenting cells (APCs) [20]. IL-15, bound to cell surface IL-15R on APCs, is then presented in trans to T cells and NK cells expressing the c receptor dimer [20]. IL15 then induces signalling at the interface of the immunological synapse and contributes to co-stimulatory signals that modify the cell response [31]. Since the IL-2R and -15R contain the same - and -subunits, subsequent signal transduction is mediated by the same molecules, Janus kinases 1 and 3 (JAKs1/3) and Signal Transducer and Activator of Transcription 3 and 5 (STATs 3/5) [4, 32, 33]. JAK1 is recruited to the IL-2R chain, whereas JAK3 is recruited to the IL-2R chain (Fig. 1). Additionally, IL-15 triggers several other signalling pathways, including phosphorylation of the Src-family of protein tyrosine kinases Lck and Syk, stimulation of the phosphatidylinositol-3-kinase (PI3-K)/AKT pathway, and stimulation of the Ras/Raf/MAPK pathway leading to the activation of Fos- and Jun-containing transcription factor complexes [34]. IL-15-mediated T-cell proliferation is also regulated through FK506-binding protein 12 (FKBP12) activation of p70-S6 kinase. Moreover, FKBP12 is involved in the pathway leading to the activation of ERK MAPK downstream of IL-15 [35]. Notably, signalling pathways can also be triggered through IL-15R. Membrane-associated IL-15R has a short cytoplasmic tail with no obvious signalling motifs or docking sites, and therefore was thought to have no signalling capabilities. However, the cytoplasmic domain of IL-15R can recruit TNF receptorassociated factor (TRAF) 2 following IL-15 binding resulting in nuclear factor-B (NF-B) activation. NF-B is one of the most FIG. 2. Schematic representation of the target cells of IL-15. IL-15 acts on a wide range of both immune and non-immune cell types. It is important for protection against apoptosis, supporting proliferation and functional activity of several immune cells. It is critical for Th1 and Th17 polarization; it induces effector functions in mast cells, neutrophils, NK cells, B cells, macrophages and DCs. In non-immune cells, it not only confers protection from apoptosis but it also induces angiogenesis of endothelial cells. important regulators of pro-inflammatory gene expression, resulting in the synthesis of cytokines, such as TNF-, IL-1, -6 and -8 [36]. Syk kinase has also been shown to be critical for IL-15R signalling [37, 38]. IL-15: biological activity IL-15 is a broad spectrum immune-regulatory cytokine that supports the survival, proliferation and functional activity of a number of immune cell types (Fig. 2 and Table 1). Indeed, mice deficient in IL-15 exhibit depleted NK, NKT, T, CD8þ and Role of Il-15 and -18 in autoimmunity TABLE 1. The functional effects of IL-15 on cells of the immune system Cell type Th17 cells CD8 cells NK cells B cells Neutrophils DCs Monocytes Macrophages Mast cells Functional Effects Enhances TCR-mediated proliferation Critical for development and maintenance of effector memory cells Protects from apoptosis Protects from apoptosis Promotes cytotoxic activity Protects from apoptosis Enhances Ig production by activated B cells Enhances proliferation and differentiation Protects from apoptosis Enhances phagocytosis Protects from apoptosis Stimulates functional maturation Enhances T- and NK-cell simulation by up-regulating expression of co-stimulatory molecules and IFN- Enhances phagocytic activity Stimulates the production of pro-inflammatory cytokines Supports proliferation Protects from apoptosis 1271 of IFN- [58]. IL-15 also inhibits apoptosis of neutrophils by decreasing expression of pro-apoptotic protein Bax [59] and increasing expression of anti-apoptotic myeloid cell differentiation factor-1 [59, 60]. IL-15 can act as a growth factor for mast cells, supporting their proliferation and preventing their apoptosis through the up-regulation of Bcl-xL expression [61]. Mast cells use a unique high-affinity receptor for IL-15 known as IL-15RX (Fig. 1) and the signalling events following IL-15 binding to this receptor are different to other cell types. Upon IL-15 binding to IL-15RX JAK2/STAT5 or Tyk2/STAT6 are activated and this signalling cascade does not require the presence of the IL-2R- or -chains [61–63]. Interestingly, mast cells not only express IL-15RX but also a number of functional isoforms of IL-15R; however, the relevance of these two high-affinity receptors on mast cells is still unclear. IL-15 is also a major modulator of non-immune target cells inducing angiogenesis in endothelial cells and conferring protection from apoptosis in endothelial cells, fibroblasts, epithelial cells, as well as oesteoclasts (Table 1). IL-15: role in autoimmunity memory phenotype T-cell numbers, emphasizing the important role of IL-15 in lymphocyte subset development [39]. Numerous reports have shown that IL-15 is critical for the maintenance of long-lasting, high-avidity T-cell responses by sustaining the survival of CD8þCD44hi memory T cells [6, 40–44]. A recent study has identified a subset of effector memory CD8þ T cells (IL-7RlowCCR7), which proliferate weakly in response to TCR stimulation but proliferate in response to IL-15 resulting in the non-specific expansion of a polyclonal population of effector memory cells [45]. IL-15-induced proliferation and expansion of autoantigen-specific CD8þ effector memory T cells could promote autoimmune responses leading to enhanced pathogenesis of the disease. Indeed, patients with SLE show increased IL-15 levels and an expanded CD8þ effector memory T-cell population correlating with disease severity [46]. IL-15 also enhances the TCR-dependent proliferation of IL-17-secreting Th cells (Th17) and Th17/Th1 (IL-17 and IFN- producing) cells [47], which are known to play a role in the development of a number of autoimmune diseases [1, 48]. Therefore, IL-15-induced expansion of IL-17-producing T-cell populations may result in enhanced autoimmune activity. As already mentioned earlier, gene-targeting studies in mice have demonstrated that IL-15 is essential for the survival, activation and functional activity of NK cells. Mice over-expressing IL-15 have an expanded NK cell population, which results in enhanced innate immune reactions [42]. Furthermore, efficient NK cell killing has recently been shown to be mediated through the formation of a regulatory synapse with DCs to which IL-15R on the NK cells accumulates [49]. IL-15 is also critical for the functional maturation of both macrophages and DCs [50]. IL-15 enhances the phagocytic activity of monocytes and macrophages and induces the production of pro-inflammatory factors such as IL-8 and MCP-1 [51]. In DCs, IL-15 up-regulates the expression of co-stimulatory molecules and IFN-, enhancing the ability of DCs to activate CD8þ cells and NK cells [15, 52]. In addition, reduced numbers of peripheral DCs have been observed in IL-15/ and IL-15R/ mice suggesting a role for IL-15 in DC survival [53]. Interestingly, IL-15/ and -15R/ mice do not present with any defects in B-cell responses [54, 55]. However, activated B-cell functions are greatly influenced by IL-15. Activated B cells proliferate in response to IL-15 and in combination with CD40L produce IgA, IgG1 and IgM [56]. IL-15 also acts as a survival factor for activated B cells [57]. In neutrophils, IL-15 is critical for their influx into inflammatory foci during antigen-induced inflammation. In vivo administration of IL-15 can induce the production of IL-18 within 90 min, resulting in neutrophil influx that is independent IL-15 is a potent pro-inflammatory cytokine and it has been demonstrated to play a role in the pathogenesis of a number of autoimmune diseases. IL-15 is detectable in the serum of patients with ulcerative colitis [64]. The inflamed mucosa from patients with IBD expresses increased levels of IL-15 mRNA [65] and T cells from the lamina propria are more responsive to IL-15 than control T cells leading to enhanced production of the proinflammatory cytokines TNF- and IFN- [66]. Psoriatic lesions express high levels of IL-15 [67]. In a human psoriasis xenograft model, the administration of an antibody that inhibited IL-15 binding to IL-15R resulted in reduced severity of signs of the disease [68]. Indeed, Zhang et al. [69] report a genetic association between IL-15 and psoriasis. A haplotype of the 30 UTR region of IL-15 is associated with an increased risk of psoriasis and increased activity of IL-15. Patients with multiple sclerosis (MS) have increased numbers of peripheral blood mononuclear cells (PBMCs) expressing IL-15 mRNA compared with healthy controls [70] and enhanced expression of IL-15 mRNA has been found in MS-active plaques [71]. In addition, monocytes from relapsing–remitting patients have an increased level of membrane-bound IL-15 and their T cells express high levels of IL-15R, which may contribute to enhanced IFN- release during MS [72]. Studies have shown that IL-15 can be detected in the serum and synovial membrane of patients with RA [73–76]. In association with IL-18, -12 and IFN-, IL-15 has also been detected in synovial membrane derived from patients with JRA [77]. In addition, IL-15 expressed by fibroblast-like synoviocytes and endothelial cells, has been shown to cause a marked increase in transendothelial migration of both CD4þ and CD8þ T cells [78]. These data were supported by the observation that the expression of IL-15 leads to the accumulation of T cells in RA synovial tissues engrafted into mice with severe combined immunodeficiency [78]. IL-15 enhances synovial T-cell proliferation and cytokine release. Synovial neutrophils are also activated by IL-15 [5, 79]. Indeed, upon stimulation with IL-15, neutrophils from patients with RA, but not from healthy donors, produce significant amounts of IL-18 and other chemotactic factors that may help to promote chronic inflammation [58]. As mentioned earlier, IL-15 is a potent growth and survival factor for mast cells. Mast cells make a major contribution to the pathogenesis of arthritis and are found in abundance in synovial sections from patients with RA [80]. Studies in mast cell-deficient mice have highlighted their importance for disease onset as these mice do not develop joint inflammation and are resistant to arthritis [81]. It has been proposed that mast cells may be a cellular link between autoantibodies, the complement system and the 1272 H. P. Carroll et al. onset of inflammatory arthritis [81]. Interestingly, mouse mast cells have been shown to express constitutive and LPS-inducible IL-15 that is stored intracellularly [82]. Intracellular IL-15 has been shown to suppress the activity of chymase in mast cells resulting in decreased production of neutrophil-recruiting chemokines [82]. It is therefore possible that extracellular and intracellular sources of IL-15 play distinct roles in mast cell function and consequently in disease pathology. Targeting IL-15 Several approaches have been used to antagonize the activity of IL-15 in vivo. These include the administration of soluble murine IL-15R, neutralizing antibodies and mutated forms of IL-15, all of which have been successful for the prevention and treatment of CIA in mice [83, 84]. Two antibodies that inhibit IL-15 activity have been developed and tested in clinical trials. MikI is a mAb raised against IL-2/IL-15R subunit that blocks trans-presentation of IL-15 by APC to target NK and CD8þ T cells [85]. It prolongs primate cardiac allograft survival [86] and it has also been tested in Phase I clinical trials in patients with MS, RA, refractory coeliac disease and HTLV-1-associated tropical spastic paraparesis. However, it has been argued whether the administration of this antibody will be effective since its effects are mediated via IL-15 and partial IL-2 blockade. Indeed, the possibility of inducing autoimmune phenotype similar to that observed in IL-2-deficient mice has been suggested as a possible obstacle to the success of this therapy [87]. AMG14 (also known as HuMax-IL-15), a human IgG1 mAb that binds and neutralizes the activity of both soluble and membrane-bound IL-15 in vitro has also been tested in humans [88]. Preliminary results have shown that IL-15 neutralization was well tolerated and resulted in marked improvements in disease activity [88]. However, this initial study was not placebo controlled and consequently another multi-centre, randomized, doubleblind, placebo trail was conducted, which reported no significant alterations in the levels of NK and CD8þ memory T cells [88]. The two major signalling pathways activated by IL-15 are the NF-B and the JAK–STAT pathways and they have been the subject of intense research in the search for possible therapeutic interventions. Activation of NF-B is the major event in the signalling cascade downstream of the IL-18 receptor and will be discussed subsequently. IL-15, like all the c-utilizing cytokine activates JAK3, and a JAK3 antagonist, CP690 550 has now been developed. This inhibitor shows nanomolar potency, and has demonstrated good immunosuppressant activity in a primate model of transplantation [89]. IL-2 signalling was effectively blocked in animals treated with this inhibitor, with minimal effects on the number of NK cell suggesting that IL-15 signalling was possibly only mildly affected. Nonetheless, clinical studies using CP690 550 are now ongoing in RA patients and patients with psoriatic lesions [90–92]. In both these pathologies, good remission rates and dose-dependent improvements were observed. However, inhibition of JAK2, which is also non-specifically inhibited by CP690 550, has been suggested to be the cause of the anaemia observed in patients in the pre-clinical studies. In conclusion, IL-15 is an immunoregulatory cytokine which exhibits pro-inflammatory activity by acting on a wide variety of cell types. Some of these effects are direct and include Th1 and Th17 polarization as well as activation of effector cells such as B, NK, mast cells and neutrophils. Other effects are indirect and involve the production of other pro-inflammatory cytokines such as IFN- and IL-17 as well as IL-18. In particular, the induction of IL-18 in neutrophils is of primary importance for the initial stages of the inflammatory process and we will now discuss in detail the effects of this other immunoregulatory cytokine. IL-18 IL-18: structure and production IL-18 is a member of the IL-1 superfamily of cytokines and was initially discovered as an IFN--inducing factor produced by macrophages stimulated with microbes or microbial products [93]. IL-18 is produced as an inactive 23 kDa precursor that is cleaved by caspase 1 to form the biologically active 18 kDa species [94]. Proteinase-3, caspase-3, cathepsins and elastase can also cleave the precursor polypeptide, but this can result in the production of inactive forms of IL-18 [95–97]. The IL-18 promoter does not contain a TATA sequence and is constitutively active upstream of exon 2, resulting in the continuous expression of IL-18 mRNA [98]. Control of IL-18 expression occurs primarily through processing of the procytokine into the active form and its subsequent release. Not only is IL-18 controlled by cleavage of the pro-cytokine to the active form, the biological activity of IL-18 is also controlled by IL-18 binding protein (IL-18BP). IL-18BP has a high affinity for IL-18 and neutralizes its biological activity [99, 100]. There are four human isoforms of IL-18BP, which are specific for the mature active form of IL-18 and their expression is localized to the spleen and intestinal tract [101]. Interestingly, IL-18BP expression in keratinocytes and intestinal cell lines is up-regulated in response to IFN- [102]. Therefore, a negative feedback loop exists for IL-18-induced IFN- production by Th1 cells. The IL-1 homologue, IL-1F7, also binds to IL-18BP and it has been proposed that it plays a role as a negative regulator of IL-18 activity. When bound to IL-18BP, IL-1F7 can form a complex with IL-18R chain preventing the formation of a functional receptor complex [101]. IL-18: receptor and signalling IL-18 signals through the IL-18 receptor complex (IL-18R), which is a heterodimer consisting of IL-18R and -18R subunits. The extracellular domains of both IL-18R chains contain three Ig-like domains and an intracellular region comprising a Toll/IL-1 receptor (TIR) domain (Fig. 1). The IL-18R subunit is responsible for ligand binding, whereas the IL-18R subunit is a nonbinding signalling chain. The IL-18R complex is expressed on lymphocytes and other cells such as plasmacytoid DCs [103] and is up-regulated by IL-12, -2, [104, 105] and inhibited by IL-4 [106]. Following binding of IL-18 to the low-affinity IL-18R, the IL-18R chain is recruited forming the high-affinity heterodimeric receptor complex that brings the TIR domains within the intracellular regions of each receptor chain into close proximity. Once the TIR domains of the IL-18R- and -chains are engaged the adaptor protein myeloid differentiation factor 88 (MyD88) then docks to the IL-18R complex resulting in the phosphorylation of IL-1 receptor-associated kinases (IRAKs) [107]. IRAK1 and IRAK4 have both been implicated in IL-18 signalling in NK and Th1 cells, since IRAK1/, and in particular IRAK4/, mice display impaired responses to IL-18 stimulation [108, 109]. IRAK activation results in the recruitment of TRAF6. IB kinase (IKK) is then activated and degrades IB, allowing NF-B to translocate to the nucleus activating gene transcription [36]. IL-18 signal transduction is thought to be primarily mediated through this MyD88-dependent pathway. Indeed, MyD88 is an essential component of IL-18R signalling, since Th1 cells from MyD88/ mice are unresponsive to IL-18 [110]. In addition, the inhibitory receptors Toll IL-1R 8/single Ig IL-1-related receptor (TIR8/SIGIRR), which contain TIR domains in their intracellular region, compete with the IL-18R complex for MyD88 and TRAF6 inhibiting IL-18 activity. Moreover, TIR8/SIGIRR-deficient mice are more susceptible to IL-18 stimulation, whereas, cells overexpressing TIR8/SIGIRR are less susceptible to IL-18 stimulation [111]. However, IL-18 has also been shown to induce the production of MCP-1 through the PI3K/AKT and MEK/ERK1/2 Role of Il-15 and -18 in autoimmunity FIG. 3. Schematic representation of the functional activities of IL-18. IL-18 is produced by many cell types including, macrophages, dendritic cells, oesteoblasts and chondrocytes. In synergy with IL-12, IL-18 can induce the production of IFN- by Th1 cells and NK cells, whereas it synergizes with IL-23, -18 to enhance IL-17 production by Th17 cells. IL-18 also enhances the production of pro-inflammatory cytokines and chemokines by macrophages and synoviocytes. In basophils and mast cells, IL-18, in the presence of IL-3, induces the production of IL-4 and -13, which support Th2 responses. In B cells, IL-18 also induces the production of IL-4 and -13 and maintains IgE expression. TABLE 2. The functional effects of IL-18 on cells of the immune system Cell type Th1 cells Th17 cells NK cells B cells Mast cells/Basophils Functional Effects In combination with IL-12, induces IFN- production In combination with IL-23, enhances IL-17 production Promotes functional development and cytotoxic activity Enhances IL-4, IL-13 and IgE production In combination with IL-3, induces IL-4 and IL-13 production pathways. Inhibition of both of these pathways results in the complete abrogation of IL-18-induced MCP-1 production [112, 113]. A soluble form of IL-18R (sIL-18R) has recently been identified, which is produced by differential splicing [114]. In vitro studies reveal that the novel soluble receptor can inhibit IL-18induced IFN- production. A number of spliced variants of sIL-18R have been identified. Indeed, it has been previously observed that IL-18R exists as heterogenous molecules ranging from 60 to 110 kDa [93]. It is therefore possible that IL-18Rspliced variants may each have distinct functions in the regulation of IL-18 activity. IL-18: biological activity IL-18 acts synergistically with IL-12 to induce IFN- production by several types of cells. IL-18 can induce IFN- production from T cells independently of TCR activation, a property unique to IL-18 [104] (Fig. 3 and Table 2). Considering the importance of IFN- for pathogen clearance, IL-18 has been shown, using animal models, to be required for the IFN--dependent eradication of several microbial infections. However, its biological role extends beyond IFN- production and Th1 polarization. IL-18 induces both T- and NK-cell maturation and potentiates cytotoxicity. In fact, IL-18-deficient mice show reduced NK cytolytic activity [113]. IL-18 is also involved in Th17 cell responses and, in synergy with IL-23, can amplify IL-17 production by Th17polarized cells in a TCR-independent manner [115]. IL-18 can also induce TNF- production both in vitro and in vivo, an effect that links this cytokine to the development of the inflammatory response and the pathogenesis of several autoimmune diseases. Chemokines such as CXCL8, CXCL5 and CCL20 as well as adhesion molecule (ICAM-1, VCAM-1) 1273 expressions are also induced by IL-18 in isolated synovial tissue fibroblasts and endothelial cells [116, 117]. On the other hand, IL-18 has been shown to have an indirect role in inducing Th2 responses. IL-18 directly induces IL-4 and -13 secretion, as well as high IgE expression by B cells. The capacity of IL-18 to induce a Th2 response depends on CD4þ T cells, NK-T cells and IL-4. In fact, IL-18-induced IgE production is abrogated in CD4þ T cell-depleted and in IL-4/ mice [118]. IL-18 can induce the production of IL-4 and -13 even in the absence of Fc"RI engagement if IL-3 is present in the milieu. Interestingly, IL-12 and IFN- are incapable of blocking this IL-18-driven activation suggesting that IL-18 involvement in the Th2 response can occur in parallel with a Th1 response [119]. Along with macrophages, IL-18 is also secreted by DCs, Langerhans cells, osteoblasts and chondrocytes [120–122]. Moreover, IL-18 enhances the production of angiogenic and chemotactic factors such as VEGF, CXCL12 and CCL2 in synovial fibroblasts [123]. Altogether, it is clear that, by regulating Th differentiation, B-cell activation and Ig production as well as its activity on DCs, NK and neutrophils, IL-18 is a cytokine that has an important role in both the innate as well as the adaptive immune response (Table 2). IL-18: role in autoimmunity and allergy Like IL-15, IL-18 exerts its effects on a wide array of cell types. Consequently, this has implications for the pathogenicity of several inflammatory diseases. Patients with Crohn’s disease have high serum levels of IL-18 [124]. Accordingly, a correlation between the level of IL-18 and severity of the disease has been shown in animal models, whereas IL-18-deficient mice or mice treated with IL-18BP can escape this disease. IL-18 also promotes the onset of insulindependent diabetes mellitus, through the Th1-mediated destruction of pancreatic -cells [125]. Transgenic expression of IL-18 in murine keratinocytes results in the development of spontaneous atopic dermatitis. Moreover, in several studies, patients have shown a correlation between serum IL-18 and IgE levels and severity of atopic dermatitis. A role for IL-18 has also been postulated in bronchial asthma with elevated serum levels of IL-18, which correlate with the severity of the disease [126]. In mice, IL-18 exacerbates airway inflammation and infiltration possibly through the induction of chemokine release [126]. Increased serum IL-18 levels have also been observed in allergic rhinitis and, interestingly, a single nucleotide polymorphism in the IL18 gene has recently been associated with this disease [127, 128]. IL-18 has also been shown to be up-regulated in RA [129]. Elevated levels of IL-18 are found in the synovial tissue, synovial fluid and sera of patients with RA. The administration of IL-18 to mice with CIA significantly increases the severity of the disease that is reduced following IL-18 blockade [130, 131]. Furthermore, the expression of IL-18 in rheumatoid synovium has been found to correlate with IL-1 expression, macrophage infiltration and inflammation. In addition, the bioactivity of IL-18 from affected joints of patients with RA correlates with disease severity. Notably, elevated IL-18BP levels have also been described in RA [132]. Joint inflammation induced by IL-18 is partly TNF- dependent. Mice deficient in TNF- display reduced lymphocyte infiltration and joint inflammation in response to IL-18 [133]. Indeed, RA patients receiving the anti-TNF- antibody infliximab show reduced IL-18 production and disease symptoms were ameliorated [134]. As mentioned earlier, IL-18, in synergy with IL-23, amplifies IL-17 production, which has been shown to play a pathogenic role in autoimmune diseases, in particular RA, by promoting cartilage destruction and osteoclastogenesis [135]. Targeting IL-18 Antagonizing the biological activity of pro-inflammatory cytokines such as IL-18 has the potential to improve symptoms and 1274 H. P. Carroll et al. the pathological features associated with the inflammatory processes in which they are involved. To this end several therapeutic approaches have been developed and are currently under investigation. The naturally occurring IL-18BP was first investigated as a therapeutic approach in animals, with very promising results [136–138] and is currently being tested in humans. As with all naturally occurring inhibitors there are no problems related to their possible immunogenicity; however, issues regarding their pharmacokinetics still need to be addressed. From this point of view, the use of mAbs specific for IL-18 and -18R may offer a better solution. Indeed, animal models testing the efficacy of mAbs against IL-18 and -18R have given results that warrant further exploration in humans [139]. Considering the role of IL-18 in the normal immune response, it is possible that anti-IL-18 therapy may result in increased mycobacterial infections that have previously been observed as a side-effect of anti-TNF therapy. Furthermore, interfering with Th1 responses may alter the normal anti-tumour immune response [140]. These and other possible problems need to be taken into account in any therapeutic approach directed towards IL-18 or its receptor. IL-18 activity could be prevented by blocking caspase-1mediated cleavage of the cytokine into its mature form. This approach would also prevent the formation of the mature form of the pro-inflammatory cytokine IL-1. Agents capable of blocking caspase-1 have already showed promising results in humans and clinical trials are currently ongoing for the treatment of RA [141]. As mentioned earlier, the main downstream event in IL-18 signalling is the activation of NF-B. NF-B target genes are involved in cellular events ranging from proliferation to inflammation and include genes for cytokines and chemokines as well as cyclins and anti-apoptotic genes and it is through this transcription factor that IL-18 exerts its pro-inflammatory activity. Historically, inhibition of NF-B has been found to be one of the key mechanisms by which steroids, NSAIDs as well as some natural and synthetic compounds act. Despite the prediction that blocking NF-B may result in immunosuppression and increased susceptibility to tumour development, several therapeutic strategies that target this pathway have been pursued. These include inhibition of IkB phosphorylation and degradation as well as inhibition of NF-B nuclear translocation. Compounds targeting IKK molecules such as IMD-0560, SC-514, TPCA-1, BMS345541 and ML120B have shown promising activity in vitro and in pre-clinical studies with block of the secretion and release of metalloproteinase as well as cytokines and prevention of bone erosion [142–146]. Among the drugs known to affect IB degradation, the boronic acid peptide bortezomib, which has already been approved for the treatment of human malignancies, is possibly the most interesting. In pre-clinical studies in rats, bortezomib has been shown to effectively reduce the severity of experimental autoimmune encephalomyelitis (EAE) reducing the incidence of clinical relapses, central nervous system (CNS) histopathology, and Tcell responses [147]. A plant-derived compound with a mechanism of action similar to glucocorticoids has been recently described to be able to block the inflammatory response [148]. This transrepression activity is also shared by some ligands of peroxisiome proliferator-activated receptors (PPAR) and PPAR agonists have shown efficacy in several pre-clinical models [110, 149–151]. Conclusions In the past 15 yrs, our understanding of the complex cytokine network, which is central to the pathogenesis of autoimmune disease, is increased dramatically. In these two reviews, we have aimed at highlighting the basic biology of a number of cytokines, which we believe play a key role in the events that lead to chronic inflammation and eventually, in the case of RA, articular inflammation and bone erosion. We have focused on the signalling cascades and we have pointed out the therapeutic approaches that are currently being developed to target such pathways. In the case of IL-15 and especially IL-18, some of these approaches have already moved from in vitro and pre-clinical studies to clinical trials suggesting that this is indeed a way forward. It is now time to move even further forward and an integration of the different approaches, such as targeting multiple cytokines and multiple pathways simultaneously, should result in greater therapeutic efficacy with a reduction in side-effects as some of the in vitro and in vivo work seems to suggest. Rheumatology key messages Among the complex network of pro-inflammatory cytokines involved in the development of autoimmune diseases, IL-15 and -18 have both been shown to be of great importance. The targeting of IL-15 and -18 for therapeutic purposes is already a reality with a novel approach focussed on blocking their receptor binding. The intracellular pathways that these two cytokines activate appear to be an exciting area of research, which may result in novel drugs for the treatment of inflammatory diseases. Disclosure statement: The authors have declared no conflicts of interest. References 1 Paunovic V, Carroll HP, Vandenbroek K, Gadina M. Crossed signals: the role of interleukin (IL)-12, 17, 23, and 27 in autoimmunity. Rheumatology 2008;47:771–6. 2 Bamford RN, Grant AJ, Burton JD et al. The interleukin (IL) 2 receptor beta chain is shared by IL-2 and a cytokine, provisionally designated IL-T, that stimulates T-cell proliferation and the induction of lymphokine-activated killer cells. Proc Natl Acad Sci USA 1994;91:4940–4. 3 Grabstein KH, Eisenman J, Shanebeck K et al. Cloning of a T cell growth factor that interacts with the beta chain of the interleukin-2 receptor. Science 1994;264:965–8. 4 Waldmann TA, Dubois S, Tagaya Y. Contrasting roles of IL-2 and IL-15 in the life and death of lymphocytes: implications for immunotherapy. Immunity 2001;14:105–10. 5 Waldmann TA, Tagaya Y. The multifaceted regulation of interleukin-15 expression and the role of this cytokine in NK cell differentiation and host response to intracellular pathogens. Annu Rev Immunol 1999;17:19–49. 6 Fehniger TA, Cooper MA, Caligiuri MA. Interleukin-2 and interleukin-15: immunotherapy for cancer. Cytokine Growth Factor Rev 2002;13:169–83. 7 Fehniger TA, Caligiuri MA. Ontogeny and expansion of human natural killer cells: clinical implications. Int Rev Immunol 2001;20:503–34. 8 Carson WE, Fehniger TA, Caligiuri MA. CD56bright natural killer cell subsets: characterization of distinct functional responses to interleukin-2 and the c-kit ligand. Eur J Immunol 1997;27:354–60. 9 Waldmann TA. Targeting the interleukin-15 system in rheumatoid arthritis. Arthritis Rheum 2005;52:2585–8. 10 Bamford RN, DeFilippis AP, Azimi N, Kurys G, Waldmann TA. The 50 untranslated region, signal peptide, and the coding sequence of the carboxyl terminus of IL-15 participate in its multifaceted translational control. J Immunol 1998;160:4418–26. 11 Briard D, Brouty-Boye D, Azzarone B, Jasmin C. Fibroblasts from human spleen regulate NK cell differentiation from blood CD34(þ) progenitors via cell surface IL-15. J Immunol 2002;168:4326–32. 12 Ozawa A, Tada H, Sugawara Y et al. Endogenous IL-15 sustains recruitment of IL-2Rbeta and common gamma and IL-2-mediated chemokine production in normal and inflamed human gingival fibroblasts. J Immunol 2004;173:5180–8. 13 Rappl G, Kapsokefalou A, Heuser C et al. Dermal fibroblasts sustain proliferation of activated T cells via membrane-bound interleukin-15 upon long-term stimulation with tumor necrosis factor-alpha. J Invest Dermatol 2001;116:102–9. 14 Tagaya Y, Kurys G, Thies TA et al. Generation of secretable and nonsecretable interleukin 15 isoforms through alternate usage of signal peptides. Proc Natl Acad Sci USA 1997;94:14444–9. 15 Mattei F, Schiavoni G, Belardelli F, Tough DF. IL-15 is expressed by dendritic cells in response to type I IFN, double-stranded RNA, or lipopolysaccharide and promotes dendritic cell activation. J Immunol 2001;167:1179–87. 16 Mohamadzadeh M, McGuire MJ, Dougherty I, Cruz PD Jr. Interleukin-15 expression by human endothelial cells: up-regulation by ultraviolet B and psoralen plus ultraviolet A treatment. Photodermatol Photoimmunol Photomed 1996;12:17–21. 17 Fawaz LM, Sharif-Askari E, Menezes J. Up-regulation of NK cytotoxic activity via IL-15 induction by different viruses: a comparative study. J Immunol 1999;163: 4473–80. 18 Tran P, Ahmad R, Xu J, Ahmad A, Menezes J. Host’s innate immune response to fungal and bacterial agents in vitro: up-regulation of interleukin-15 gene expression resulting in enhanced natural killer cell activity. Immunology 2003;109:263–70. 19 Kurowska M, Rudnicka W, Kontny E et al. Fibroblast-like synoviocytes from rheumatoid arthritis patients express functional IL-15 receptor complex: endogenous Role of Il-15 and -18 in autoimmunity 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 IL-15 in autocrine fashion enhances cell proliferation and expression of Bcl-x(L) and Bcl-2. J Immunol 2002;169:1760–7. Dubois S, Mariner J, Waldmann TA, Tagaya Y. IL-15Ralpha recycles and presents IL-15 in trans to neighboring cells. Immunity 2002;17:537–47. Anderson DM, Kumaki S, Ahdieh M et al. Functional characterization of the human interleukin-15 receptor alpha chain and close linkage of IL15RA and IL2RA genes. J Biol Chem 1995;270:29862–9. Wang X, Rickert M, Garcia KC. Structure of the quaternary complex of interleukin-2 with its alpha, beta, and gammac receptors. Science 2005;310:1159–63. Giri JG, Kumaki S, Ahdieh M et al. Identification and cloning of a novel IL-15 binding protein that is structurally related to the alpha chain of the IL-2 receptor. EMBO J 1995;14:3654–63. Lorenzen I, Dingley AJ, Jacques Y, Grotzinger J. The structure of the interleukin-15 alpha receptor and its implications for ligand binding. J Biol Chem 2006;281:6642–7. Chirifu M, Hayashi C, Nakamura T et al. Crystal structure of the IL-15-IL-15Ralpha complex, a cytokine-receptor unit presented in trans. Nat Immunol 2007;8:1001–7. Budagian V, Bulanova E, Orinska Z et al. Natural soluble interleukin-15Ralpha is generated by cleavage that involves the tumor necrosis factor-alpha-converting enzyme (TACE/ADAM17). J Biol Chem 2004;279:40368–75. Mortier E, Bernard J, Plet A, Jacques Y. Natural, proteolytic release of a soluble form of human IL-15 receptor alpha-chain that behaves as a specific, high affinity IL-15 antagonist. J Immunol 2004;173:1681–8. Rubinstein MP, Kovar M, Purton JF et al. Converting IL-15 to a superagonist by binding to soluble IL-15R{alpha}. Proc Natl Acad Sci USA 2006;103:9166–71. Nguyen KB, Salazar-Mather TP, Dalod MY et al. Coordinated and distinct roles for IFN-alpha beta, IL-12, and IL-15 regulation of NK cell responses to viral infection. J Immunol 2002;169:4279–87. Ruckert R, Brandt K, Braun A et al. Blocking IL-15 prevents the induction of allergenspecific T cells and allergic inflammation in vivo. J Immunol 2005;174:5507–15. Schluns KS, Stoklasek T, Lefrancois L. The roles of interleukin-15 receptor alpha: trans-presentation, receptor component, or both? Int J Biochem Cell Biol 2005;37: 1567–71. Fehniger TA, Caligiuri MA. Interleukin 15: biology and relevance to human disease. Blood 2001;97:14–32. Sugamura K, Takeshita T, Asao H et al. The IL-2/IL-2 receptor system: involvement of a novel receptor subunit, gamma chain, in growth signal transduction. Tohoku J Exp Med 1992;168:231–7. Miyazaki T, Liu ZJ, Kawahara A et al. Three distinct IL-2 signaling pathways mediated by bcl-2, c-myc, and lck cooperate in hematopoietic cell proliferation. Cell 1995;81:223–31. Dubois S, Shou W, Haneline LS, Fleischer S, Waldmann TA, Muller JR. Distinct pathways involving the FK506-binding proteins 12 and 12.6 underlie IL-2-versus IL-15-mediated proliferation of T cells. Proc Natl Acad Sci USA 2003;100:14169–74. Andreakos E, Sacre S, Foxwell BM, Feldmann M. The toll-like receptor-nuclear factor kappaB pathway in rheumatoid arthritis. Front Biosci 2005;10:2478–88. Bulanova E, Budagian V, Pohl T et al. The IL-15R alpha chain signals through association with Syk in human B cells. J Immunol 2001;167:6292–302. Ratthe C, Girard D. Interleukin-15 enhances human neutrophil phagocytosis by a Syk-dependent mechanism: importance of the IL-15Ralpha chain. J Leukoc Biol 2004;76:162–8. Lodolce JP, Burkett PR, Koka RM, Boone DL, Ma A. Regulation of lymphoid homeostasis by interleukin-15. Cytokine Growth Factor Rev 2002;13:429–39. Zhang X, Sun S, Hwang I, Tough DF, Sprent J. Potent and selective stimulation of memory-phenotype CD8þ T cells in vivo by IL-15. Immunity 1998;8:591–9. Ku CC, Murakami M, Sakamoto A, Kappler J, Marrack P. Control of homeostasis of CD8þ memory T cells by opposing cytokines. Science 2000;288:675–8. Marks-Konczalik J, Dubois S, Losi JM et al. IL-2-induced activation-induced cell death is inhibited in IL-15 transgenic mice. Proc Natl Acad Sci USA 2000;97: 11445–50. Schluns KS, Klonowski KD, Lefrancois L. Transregulation of memory CD8 T-cell proliferation by IL-15Ralphaþ bone marrow-derived cells. Blood 2004;103:988–94. Becker TC, Wherry EJ, Boone D et al. Interleukin 15 is required for proliferative renewal of virus-specific memory CD8 T cells. J Exp Med 2002;195:1541–8. Kim HR, Hwang KA, Kang I. Dual roles of IL-15 in maintaining IL-7RalphalowCCR7memory CD8þ T cells in humans via recovering the phosphatidylinositol 3-kinase/ AKT pathway. J Immunol 2007;179:6734–40. Blanco P, Pitard V, Viallard JF, Taupin JL, Pellegrin JL, Moreau JF. Increase in activated CD8þ T lymphocytes expressing perforin and granzyme B correlates with disease activity in patients with systemic lupus erythematosus. Arthritis Rheum 2005;52:201–11. Annunziato F, Cosmi L, Santarlasci V et al. Phenotypic and functional features of human Th17 cells. J Exp Med 2007;204:1849–61. Kikly K, Liu L, Na S, Sedgwick JD. The IL-23/Th(17) axis: therapeutic targets for autoimmune inflammation. Curr Opin Immunol 2006;18:670–5. Brilot F, Strowig T, Roberts SM, Arrey F, Munz C. NK cell survival mediated through the regulatory synapse with human DCs requires IL-15Ralpha. J Clin Invest 2007;117:3316–29. Ohteki T, Suzue K, Maki C, Ota T, Koyasu S. Critical role of IL-15-IL-15R for antigenpresenting cell functions in the innate immune response. Nat Immunol 2001;2: 1138–43. Badolato R, Ponzi AN, Millesimo M, Notarangelo LD, Musso T. Interleukin-15 (IL-15) induces IL-8 and monocyte chemotactic protein 1 production in human monocytes. Blood 1997;90:2804–9. Jinushi M, Takehara T, Tatsumi T et al. Autocrine/paracrine IL-15 that is required for type I IFN-mediated dendritic cell expression of MHC class I-related chain A and B is impaired in hepatitis C virus infection. J Immunol 2003;171:5423–9. 1275 53 Dubois SP, Waldmann TA, Muller JR. Survival adjustment of mature dendritic cells by IL-15. Proc Natl Acad Sci USA 2005;102:8662–7. 54 Lodolce JP, Boone DL, Chai S et al. IL-15 receptor maintains lymphoid homeostasis by supporting lymphocyte homing and proliferation. Immunity 1998;9:669–76. 55 Kennedy MK, Glaccum M, Brown SN et al. Reversible defects in natural killer and memory CD8 T cell lineages in interleukin 15-deficient mice. J Exp Med 2000;191:771–80. 56 Armitage RJ, Macduff BM, Eisenman J, Paxton R, Grabstein KH. IL-15 has stimulatory activity for the induction of B cell proliferation and differentiation. J Immunol 1995;154:483–90. 57 Bulfone-Paus S, Ungureanu D, Pohl T et al. Interleukin-15 protects from lethal apoptosis in vivo. Nat Med 1997;3:1124–8. 58 Verri WA Jr, Cunha TM, Ferreira SH et al. IL-15 mediates antigen-induced neutrophil migration by triggering IL-18 production. Eur J Immunol 2007;37:3373–80. 59 Ottonello L, Frumento G, Arduino N et al. Differential regulation of spontaneous and immune complex-induced neutrophil apoptosis by proinflammatory cytokines. Role of oxidants, Bax and caspase-3. J Leukoc Biol 2002;72:125–32. 60 Pelletier M, Ratthe C, Girard D. Mechanisms involved in interleukin-15-induced suppression of human neutrophil apoptosis: role of the anti-apoptotic Mcl-1 protein and several kinases including Janus kinase-2, p38 mitogen-activated protein kinase and extracellular signal-regulated kinases-1/2. FEBS Lett 2002;532:164–70. 61 Masuda A, Matsuguchi T, Yamaki K, Hayakawa T, Yoshikai Y. Interleukin-15 prevents mouse mast cell apoptosis through STAT6-mediated Bcl-xL expression. J Biol Chem 2001;276:26107–13. 62 Masuda A, Matsuguchi T, Yamaki K et al. Interleukin-15 induces rapid tyrosine phosphorylation of STAT6 and the expression of interleukin-4 in mouse mast cells. J Biol Chem 2000;275:29331–7. 63 Tagaya Y, Burton JD, Miyamoto Y, Waldmann TA. Identification of a novel receptor/ signal transduction pathway for IL-15/T in mast cells. EMBO J 1996;15:4928–39. 64 Kirman I, Nielsen OH. Increased numbers of interleukin-15-expressing cells in active ulcerative colitis. Am J Gastroenterol 1996;91:1789–94. 65 Sakai T, Kusugami K, Nishimura H et al. Interleukin 15 activity in the rectal mucosa of inflammatory bowel disease. Gastroenterology 1998;114:1237–43. 66 Liu Z, Geboes K, Colpaert S, D’Haens GR, Rutgeerts P, Ceuppens JL. IL-15 is highly expressed in inflammatory bowel disease and regulates local T cell-dependent cytokine production. J Immunol 2000;164:3608–15. 67 Ruckert R, Asadullah K, Seifert M et al. Inhibition of keratinocyte apoptosis by IL-15: a new parameter in the pathogenesis of psoriasis? J Immunol 2000;165:2240–50. 68 Villadsen LS, Schuurman J, Beurskens F et al. Resolution of psoriasis upon blockade of IL-15 biological activity in a xenograft mouse model. J Clin Invest 2003;112:1571–80. 69 Zhang XJ, Yan KL, Wang ZM et al. Polymorphisms in interleukin-15 gene on chromosome 4q31.2 are associated with psoriasis vulgaris in Chinese population. J Invest Dermatol 2007;127:2544–51. 70 Kivisakk P, Matusevicius D, He B, Soderstrom M, Fredrikson S, Link H. IL-15 mRNA expression is up-regulated in blood and cerebrospinal fluid mononuclear cells in multiple sclerosis (MS). Clin Exp Immunol 1998;111:193–7. 71 Baranzini SE, Elfstrom C, Chang SY et al. Transcriptional analysis of multiple sclerosis brain lesions reveals a complex pattern of cytokine expression. J Immunol 2000;165:6576–82. 72 Vaknin-Dembinsky A, Brass S, Gandhi R, Weiner HL. Membrane bound IL-15 is increased on CD14 monocytes in early stages of MS. J Neuroimmunol 2008;195:135–9. 73 McInnes IB, Liew FY. Interleukin 15: a proinflammatory role in rheumatoid arthritis synovitis. Immunol Today 1998;19:75–9. 74 Liew FY, McInnes IB. The role of innate mediators in inflammatory response. Mol Immunol 2002;38:887–90. 75 Kotake S, Schumacher HR Jr, Yarboro CH et al. In vivo gene expression of type 1 and type 2 cytokines in synovial tissues from patients in early stages of rheumatoid, reactive, and undifferentiated arthritis. Proc Assoc Am Physicians 1997;109: 286–301. 76 McInnes IB, al-Mughales J, Field M et al. The role of interleukin-15 in T-cell migration and activation in rheumatoid arthritis. Nat Med 1996;2:175–82. 77 Scola MP, Thompson SD, Brunner HI et al. Interferon-gamma:interleukin 4 ratios and associated type 1 cytokine expression in juvenile rheumatoid arthritis synovial tissue. J Rheumatol 2002;29:369–78. 78 Oppenheimer-Marks N, Brezinschek RI, Mohamadzadeh M, Vita R, Lipsky PE. Interleukin 15 is produced by endothelial cells and increases the transendothelial migration of T cells in vitro and in the SCID mouse-human rheumatoid arthritis model in vivo. J Clin Invest 1998;101:1261–72. 79 McInnes IB, Gracie JA, Harnett M, Harnett W, Liew FY. New strategies to control inflammatory synovitis: interleukin 15 and beyond. Ann Rheum Dis 2003;62 (Suppl 2):ii51–4. 80 Kiener HP, Baghestanian M, Dominkus M et al. Expression of the C5a receptor (CD88) on synovial mast cells in patients with rheumatoid arthritis. Arthritis Rheum 1998;41:233–45. 81 Lee DM, Friend DS, Gurish MF, Benoist C, Mathis D, Brenner MB. Mast cells: a cellular link between autoantibodies and inflammatory arthritis. Science 2002;297: 1689–92. 82 Orinska Z, Maurer M, Mirghomizadeh F et al. IL-15 constrains mast celldependent antibacterial defenses by suppressing chymase activities. Nat Med 2007;13:927–34. 83 Ribbens C, Dayer JM, Chizzolini C. CD40-CD40 ligand (CD154) engagement is required but may not be sufficient for human T helper 1 cell induction of interleukin-2or interleukin-15-driven, contact-dependent, interleukin-1beta production by monocytes. Immunology 2000;99:279–86. 1276 H. P. Carroll et al. 84 Ferrari-Lacraz S, Zanelli E, Neuberg M et al. Targeting IL-15 receptor-bearing cells with an antagonist mutant IL-15/Fc protein prevents disease development and progression in murine collagen-induced arthritis. J Immunol 2004;173:5818–26. 85 Morris JC, Janik JE, White JD et al. Preclinical and phase I clinical trial of blockade of IL-15 using Mikbeta1 monoclonal antibody in T cell large granular lymphocyte leukemia. Proc Natl Acad Sci USA 2006;103:401–6. 86 Tinubu SA, Hakimi J, Kondas JA et al. Humanized antibody directed to the IL-2 receptor beta-chain prolongs primate cardiac allograft survival. J Immunol 1994;153:4330–8. 87 Connell L, McInnes IB. New cytokine targets in inflammatory rheumatic diseases. Best Pract Res Clin Rheumatol 2006;20:865–78. 88 Baslund B, Tvede N, Danneskiold-Samsoe B et al. Targeting interleukin-15 in patients with rheumatoid arthritis: a proof-of-concept study. Arthritis Rheum 2005;52:2686–92. 89 Changelian PS, Flanagan ME, Ball DJ et al. Prevention of organ allograft rejection by a specific Janus kinase 3 inhibitor. Science 2003;302:875–8. 90 Breedveld FC, Bloom BJ, Coombs J et al. 6 Weeks of treatment of active rheumatoid arthritis with an orally active inhibitor of Janus Kinase 3, CP-690,550, is associated with dose-dependent increases in remission rates and improvement in the CDAI and SDAI. Ann Rheum Dis 2007;66(Suppl 2):441. 91 Coombs JH, Bloom BJ, Breedveld FC et al. Improvements in pain, function, and health status in patients taking CP-690,550, an orally active inhibitor of Janus kinase 3 (JAK3I): results from a randomized, double-blind, placebo-controlled trial in the treatment of active rheumatoid arthritis. Ann Rheum Dis 2007;66(Suppl 2):257. 92 Wilkinson B, Gaweco A, Changelian P et al. Improvement in psoriatic lesions during a 14-day trial of CP-690,550 (CP), an orally active inhibitor of Janus kinase 3 (JAK3). Ann Rheum Dis 2007;66(Suppl 2):155. 93 Nakamura S, Otani T, Okura R et al. Expression and responsiveness of human interleukin-18 receptor (IL-18R) on hematopoietic cell lines. Leukemia 2000;14: 1052–9. 94 Gu Y, Kuida K, Tsutsui H et al. Activation of interferon-gamma inducing factor mediated by interleukin-1beta converting enzyme. Science 1997;275:206–9. 95 Akita K, Ohtsuki T, Nukada Y et al. Involvement of caspase-1 and caspase-3 in the production and processing of mature human interleukin 18 in monocytic THP.1 cells. J Biol Chem 1997;272:26595–603. 96 Robertson SE, Young JD, Kitson S et al. Expression and alternative processing of IL-18 in human neutrophils. Eur J Immunol 2006;36:722–31. 97 Sugawara S, Uehara A, Nochi T et al. Neutrophil proteinase 3-mediated induction of bioactive IL-18 secretion by human oral epithelial cells. J Immunol 2001;167: 6568–75. 98 Tone M, Thompson SA, Tone Y, Fairchild PJ, Waldmann H. Regulation of IL-18 (IFN-gamma-inducing factor) gene expression. J Immunol 1997;159:6156–63. 99 Novick D, Kim SH, Fantuzzi G, Reznikov LL, Dinarello CA, Rubinstein M. Interleukin-18 binding protein: a novel modulator of the Th1 cytokine response. Immunity 1999;10:127–36. 100 Kim SH, Eisenstein M, Reznikov L et al. Structural requirements of six naturally occurring isoforms of the IL-18 binding protein to inhibit IL-18. Proc Natl Acad Sci USA 2000;97:1190–5. 101 Bufler P, Azam T, Gamboni-Robertson F et al. A complex of the IL-1 homologue IL-1F7b and IL-18-binding protein reduces IL-18 activity. Proc Natl Acad Sci USA 2002;99:13723–8. 102 Paulukat J, Bosmann M, Nold M et al. Expression and release of IL-18 binding protein in response to IFN-gamma. J Immunol 2001;167:7038–43. 103 Gutcher I, Urich E, Wolter K, Prinz M, Becher B. Interleukin 18-independent engagement of interleukin 18 receptor-alpha is required for autoimmune inflammation. Nat Immunol 2006;7:946–53. 104 Yoshimoto T, Takeda K, Tanaka T et al. IL-12 up-regulates IL-18 receptor expression on T cells, Th1 cells, and B cells: synergism with IL-18 for IFN-gamma production. J Immunol 1998;161:3400–7. 105 Nakahira M, Tomura M, Iwasaki M et al. An absolute requirement for STAT4 and a role for IFN-gamma as an amplifying factor in IL-12 induction of the functional IL-18 receptor complex. J Immunol 2001;167:1306–12. 106 Smeltz RB, Chen J, Ehrhardt R, Shevach EM. Role of IFN-gamma in Th1 differentiation: IFN-gamma regulates IL-18R alpha expression by preventing the negative effects of IL-4 and by inducing/maintaining IL-12 receptor beta 2 expression. J Immunol 2002;168:6165–72. 107 Kojima H, Takeuchi M, Ohta T et al. Interleukin-18 activates the IRAKTRAF6 pathway in mouse EL-4 cells. Biochem Biophys Res Commun 1998;244:183–6. 108 Kanakaraj P, Ngo K, Wu Y et al. Defective interleukin (IL)-18-mediated natural killer and T helper cell type 1 responses in IL-1 receptor-associated kinase (IRAK)deficient mice. J Exp Med 1999;189:1129–38. 109 Suzuki N, Chen NJ, Millar DG et al. IL-1 receptor-associated kinase 4 is essential for IL-18-mediated NK and Th1 cell responses. J Immunol 2003;170:4031–5. 110 Adachi M, Kurotani R, Morimura K et al. Peroxisome proliferator activated receptor gamma in colonic epithelial cells protects against experimental inflammatory bowel disease. Gut 2006;55:1104–13. 111 Wald D, Qin J, Zhao Z et al. SIGIRR, a negative regulator of Toll-like receptorinterleukin 1 receptor signaling. Nat Immunol 2003;4:920–7. 112 Yoo JK, Kwon H, Khil LY, Zhang L, Jun HS, Yoon JW. IL-18 induces monocyte chemotactic protein-1 production in macrophages through the phosphatidylinositol 3-kinase/Akt and MEK/ERK1/2 pathways. J Immunol 2005;175:8280–6. 113 Dinarello CA, Fantuzzi G. Interleukin-18 and host defense against infection. J Infect Dis 2003;187(Suppl 2):S370–84. 114 Liew FY, Wei XQ, McInnes IB. Role of interleukin 18 in rheumatoid arthritis. Ann Rheum Dis 2003;62(Suppl 2):ii48–50. 115 Harrington LE, Mangan PR, Weaver CT. Expanding the effector CD4 T-cell repertoire: the Th17 lineage. Curr Opin Immunol 2006;18:349–56. 116 Morel JC, Park CC, Kumar P, Koch AE. Interleukin-18 induces rheumatoid arthritis synovial fibroblast CXC chemokine production through NFkappaB activation. Lab Invest 2001;81:1371–83. 117 Morel JC, Park CC, Woods JM, Koch AE. A novel role for interleukin-18 in adhesion molecule induction through NF kappa B and phosphatidylinositol (PI) 3-kinase-dependent signal transduction pathways. J Biol Chem 2001;276:37069–75. 118 Yoshimoto T, Mizutani H, Tsutsui H et al. IL-18 induction of IgE: dependence on CD4þ T cells, IL-4 and STAT6. Nat Immunol 2000;1:132–7. 119 Yoshimoto T, Tsutsui H, Tominaga K et al. IL-18, although antiallergic when administered with IL-12, stimulates IL-4 and histamine release by basophils. Proc Natl Acad Sci USA 1999;96:13962–6. 120 Stoll S, Jonuleit H, Schmitt E et al. Production of functional IL-18 by different subtypes of murine and human dendritic cells (DC): DC-derived IL-18 enhances IL-12-dependent Th1 development. Eur J Immunol 1998;28:3231–9. 121 Brossart P, Grunebach F, Stuhler G et al. Generation of functional human dendritic cells from adherent peripheral blood monocytes by CD40 ligation in the absence of granulocyte-macrophage colony-stimulating factor. Blood 1998;92:4238–47. 122 Udagawa N, Horwood NJ, Elliott J et al. Interleukin-18 (interferon-gamma-inducing factor) is produced by osteoblasts and acts via granulocyte/macrophage colonystimulating factor and not via interferon-gamma to inhibit osteoclast formation. J Exp Med 1997;185:1005–12. 123 Amin MA, Mansfield PJ, Pakozdi A et al. Interleukin-18 induces angiogenic factors in rheumatoid arthritis synovial tissue fibroblasts via distinct signaling pathways. Arthritis Rheum 2007;56:1787–97. 124 Kanai T, Uraushihara K, Totsuka T et al. Macrophage-derived IL-18 targeting for the treatment of Crohn’s disease. Curr Drug Targets Inflamm Allergy 2003;2:131–6. 125 Oikawa Y, Shimada A, Kasuga A et al. Systemic administration of IL-18 promotes diabetes development in young nonobese diabetic mice. J Immunol 2003;171: 5865–75. 126 Tanaka H, Miyazaki N, Oashi K et al. IL-18 might reflect disease activity in mild and moderate asthma exacerbation. J Allergy Clin Immunol 2001;107:331–6. 127 Verhaeghe B, Gevaert P, Holtappels G et al. Up-regulation of IL-18 in allergic rhinitis. Allergy 2002;57:825–30. 128 Kruse S, Kuehr J, Moseler M et al. Polymorphisms in the IL 18 gene are associated with specific sensitization to common allergens and allergic rhinitis. J Allergy Clin Immunol 2003;111:117–22. 129 Muhl H, Pfeilschifter J. Interleukin-18 bioactivity: a novel target for immunopharmacological anti-inflammatory intervention. Eur J Pharmacol 2004;500:63–71. 130 Smeets RL, van de Loo FA, Arntz OJ, Bennink MB, Joosten LA, van den Berg WB. Adenoviral delivery of IL-18 binding protein C ameliorates collagen-induced arthritis in mice. Gene Ther 2003;10:1004–11. 131 Gracie JA, Forsey RJ, Chan WL et al. A proinflammatory role for IL-18 in rheumatoid arthritis. J Clin Invest 1999;104:1393–401. 132 Bresnihan B, Roux-Lombard P, Murphy E, Kane D, FitzGerald O, Dayer JM. Serum interleukin 18 and interleukin 18 binding protein in rheumatoid arthritis. Ann Rheum Dis 2002;61:726–9. 133 Joosten LA, Smeets RL, Koenders MI et al. Interleukin-18 promotes joint inflammation and induces interleukin-1-driven cartilage destruction. Am J Pathol 2004;165:959–67. 134 Pittoni V, Bombardieri M, Spinelli FR et al. Anti-tumour necrosis factor (TNF) alpha treatment of rheumatoid arthritis (infliximab) selectively down regulates the production of interleukin (IL) 18 but not of IL12 and IL13. Ann Rheum Dis 2002;61:723–5. 135 Yago T, Nanke Y, Kawamoto M et al. IL-23 induces human osteoclastogenesis via IL-17 in vitro, and anti-IL-23 antibody attenuates collagen-induced arthritis in rats. Arthritis Res Ther 2007;9:R96. 136 Plater-Zyberk C, Joosten LA, Helsen MM et al. Therapeutic effect of neutralizing endogenous IL-18 activity in the collagen-induced model of arthritis. J Clin Invest 2001;108:1825–32. 137 Banda NK, Vondracek A, Kraus D et al. Mechanisms of inhibition of collageninduced arthritis by murine IL-18 binding protein. J Immunol 2003;170:2100–5. 138 Ten Hove T, Corbaz A, Amitai H et al. Blockade of endogenous IL-18 ameliorates TNBS-induced colitis by decreasing local TNF-alpha production in mice. Gastroenterology 2001;121:1372–9. 139 Siegmund B, Fantuzzi G, Rieder F et al. Neutralization of interleukin-18 reduces severity in murine colitis and intestinal IFN-gamma and TNF-alpha production. Am J Physiol Regul Integr Comp Physiol 2001;281:R1264–73. 140 Koebel CM, Vermi W, Swann JB et al. Adaptive immunity maintains occult cancer in an equilibrium state. Nature 2007;450:903–7. 141 Pomerantz BJ, Reznikov LL, Harken AH, Dinarello CA. Inhibition of caspase 1 reduces human myocardial ischemic dysfunction via inhibition of IL-18 and IL-1beta. Proc Natl Acad Sci USA 2001;98:2871–6. 142 McIntyre KW, Shuster DJ, Gillooly KM et al. A highly selective inhibitor of I kappa B kinase, BMS-345541, blocks both joint inflammation and destruction in collageninduced arthritis in mice. Arthritis Rheum 2003;48:2652–9. Role of Il-15 and -18 in autoimmunity 143 Kishore N, Sommers C, Mathialagan S et al. A selective IKK-2 inhibitor blocks NF-kappa B-dependent gene expression in interleukin-1 beta-stimulated synovial fibroblasts. J Biol Chem 2003;278:32861–71. 144 Okazaki Y, Sawada T, Nagatani K et al. Effect of nuclear factor-kappaB inhibition on rheumatoid fibroblast-like synoviocytes and collagen induced arthritis. J Rheumatol 2005;32:1440–7. 145 Podolin PL, Callahan JF, Bolognese BJ et al. Attenuation of murine collageninduced arthritis by a novel, potent, selective small molecule inhibitor of IkappaB Kinase 2, TPCA-1 (2-[(aminocarbonyl)amino]-5-(4-fluorophenyl)-3thiophenecarboxamide), occurs via reduction of proinflammatory cytokines and antigen-induced T cell Proliferation. J Pharmacol Exp Ther 2005;312:373–81. 146 Wen D, Nong Y, Morgan JG et al. A selective small molecule IkappaB Kinase beta inhibitor blocks nuclear factor kappaB-mediated inflammatory responses in human fibroblast-like synoviocytes, chondrocytes, and mast cells. J Pharmacol Exp Ther 2006;317:989–1001. Clinical Vignette 1277 147 Vanderlugt CL, Rahbe SM, Elliott PJ, Dal Canto MC, Miller SD. Treatment of established relapsing experimental autoimmune encephalomyelitis with the proteasome inhibitor PS-519. J Autoimmun 2000;14:205–11. 148 De Bosscher K, Vanden Berghe W, Beck IM et al. A fully dissociated compound of plant origin for inflammatory gene repression. Proc Natl Acad Sci USA 2005;102:15827–32. 149 Kawahito Y, Kondo M, Tsubouchi Y et al. 15-deoxy-delta(12,14)-PGJ(2) induces synoviocyte apoptosis and suppresses adjuvant-induced arthritis in rats. J Clin Invest 2000;106:189–97. 150 Diab A, Deng C, Smith JD et al. Peroxisome proliferator-activated receptorgamma agonist 15-deoxy-Delta(12,14)-prostaglandin J(2) ameliorates experimental autoimmune encephalomyelitis. J Immunol 2002;168:2508–15. 151 Lovett-Racke AE, Hussain RZ, Northrop S et al. Peroxisome proliferator-activated receptor alpha agonists as therapy for autoimmune disease. J Immunol 2004;172:5790–8. doi:10.1093/rheumatology/ken235 Advance Access publication 28 June 2008 Hypertrophic osteoarthropathy associated with a left ventricular tumour The patient, a 36-yr-old Polynesian man, presented with a 3-month history of swelling of his extremities with clubbing of the fingers and toes and polyarthritis affecting his hands, feet and knees. Plain radiographs revealed extensive periosteal reaction along the shafts of the metacarpals (arrow in A). Axial proton density fat saturated sequence on MRI shows periosteal new bone (short arrow in B) involving the shafts of the metacarpals giving a ‘halo’ appearance. There is also associated periosteal oedema showing high signal (long arrow). The patient was eventually diagnosed with a high-grade undifferentiated pleomorphic sarcoma of his left ventricle (C, D). The hematoxylin and eosin (H&E) section taken from the resected tumour (C) shows pleomorphic spindle cell proliferation, bizarre nuclei and atypical mitoses. Vascular endothelial growth factor (VEGF), a cytokine normally inactivated in the lungs, has been implicated in the pathogenesis of hypertrophic osteoarthropathy [1]. Disclosure statement: The authors have declared no conflicts of interest. R. SUPPIAH1, F. MCQUEEN2 1 Department of Rheumatology, Auckland District Health Board, Greenlane Clinical Centre and 2Department of Molecular Medicine and Pathology, Faculty of Medicine and Health Sciences, University of Auckland, Auckland, New Zealand Accepted 28 May 2008 Correspondence to: R. Suppiah, Rheumatology Registrar, Department of Rheumatology, Auckland District Health Board, Greenlane Clinical Centre, Private Bag 92189, Auckland Mail Centre, Auckland 1142, New Zealand. E-mail: [email protected] 1 Olan F, Portela M, Navarro C et al. Circulating vascular endothelial growth factor concentrations in a case of pulmonary hypertrophic osteoarthropathy. Correlation with disease activity. J Rheumatol 2004;31:614–6.