Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
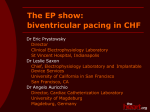
Europace (2007) 9, 1163–1170 doi:10.1093/europace/eum218 Single-site ventricular and biventricular pacing: investigation of latest depolarization strategy Michael W. Kimmel1, Nicholas D. Skadsberg2, Charles L. Byrd3, David J. Wright4, Timothy G. Laske5, and Paul A. Iaizzo6* Received 30 April 2007; accepted after revision 3 September 2007; online publish-ahead-of-print 11 October 2007 KEYWORDS Cardiac resynchronization therapy; Electrophysiology; Haemodynamics; Non-contact mapping Aims Cardiac resynchronization therapy with biventricular pacing has proved beneficial in symptomatic heart failure patients, yet the effects in patients with structurally normal hearts remain unknown. We hypothesized that, in an acute swine model with normal anatomy and function, single-site right ventricular (RV) pacing would better preserve haemodynamic function and electrical activation compared to biventricular pacing. Methods Endocardial single-site pacing was performed in anesthetized swine (n ¼ 7) from the RV septum and RV apex. Biventricular pacing was performed using an epicardial left ventricular (LV) lead and a RV lead. High-resolution, non-contact mapping was employed to record LV activation sequences simultaneously with haemodynamic data after 5 min of consistent capture. Results All pacing interventions significantly prolonged QRS and total endocardial activation durations (P , 0.05) compared to intrinsic activation. Biventricular pacing with the RV apex lead significantly impaired LV systolic mechanics (dP/dtmax, max LV pressure; P , 0.05), and reduced LV relaxation to the greatest extent (dP/dtmin, P ¼ ns). Right ventricular septal pacing conserved function better than other pacing interventions (P ¼ ns) and elicited an intrinsic electrical activation sequence. Conclusion In intact, synchronous hearts, acute biventricular pacing resulted in systolic dysfunction and abnormal LV electrical activation. Introduction Heart failure (HF) affects over 22 million people worldwide and more than 5 million individuals in the US alone and contributes to over 300 000 deaths annually.1,2 Despite advancements in HF therapy, developed resistance to pharmacologic treatments remains a major concern for cardiologists when treating late-stage HF patients.3,4 Device-based treatments such as cardiac resynchronization therapy (CRT) with biventricular (BiV) pacing have been shown to contribute considerably to improving the HF patient’s haemodynamic performance, functional status, and survival probability.2,4–12 With the increased evidence of the long-term deleterious effects of conventional right ventricular apical (RVA) pacing, there has been a growing interest in the investigation of alternative pacing sites that preserve haemodynamic * Corresponding author. Tel: þ1 612 624 7912; fax: þ1 612 624 2002. E-mail address: [email protected] function and the sequence of ventricular activation. With technologies such as robotic-assisted and minimally invasive surgeries, there are also renewed efforts examining the potential advantages of epicardial placement of left ventricular (LV) leads allowing the clinician almost unlimited access to the entire LV anterior and lateral freewall.13,14 Advances in pacing therapies, specifically BiV pacing, have resulted in significant acute haemodynamic benefits in symptomatic HF patients when stimulating late activating (lateral) regions of the LV in hearts with substantial intraventricular conduction delay.15–18 Again, pacing site (LV lead) plays a critical role in determining the degree of cardiac functional improvement and is believed to be patient dependent as was shown recently by Lambiase and coworkers.19–21 Through the use of high-resolution non-contact mapping (NCM), Lambiase demonstrated that ‘anatomically optimally placed’ transvenous leads may in fact be positioned within regions of slower conduction, Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please email: [email protected]. Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 1 Departments of Surgery and Biomedical Engineering, University of Minnesota, B172 Mayo, MMC 107, 420 Delaware Street SE, Minneapolis, MN 55455, USA; 2Medtronic, Inc., 7000 Central Avenue NE, Minneapolis, MN 55432-3576, USA; 3Broward General Medical Center, 1625 SE 3rd Avenue, Suite 610, Fort Lauderdale, FL 33316, USA; 4CardioThoracic Centre, Liverpool NHS Trust, Thomas Drive, Liverpool L14 3PE, UK; 5Medtronic, Inc., 8299 Central Avenue NE, MS P120, Minneapolis, MN 55432, USA; and 6 Department of Surgery, University of Minnesota, B172 Mayo, MMC 107, 420 Delaware Street SE, Minneapolis, MN 55455, USA 1164 thereby prolonging LV depolarization and influencing LV synchronization. To date, CRT has focused mainly on HF patients without the indication for anti-bradycardia pacing; therefore, in hearts with preserved conduction systems, the influence of pacing site and BiV therapy on cardiac function and electrophysiologic performance remains unknown. To better understand the influence of ventricular activation sequence on pump function, we employed high-resolution NCM to study the LV endocardial activation sequence. To that end, we tested the hypothesis that atrio-ventricular, single-site pacing would acutely preserve haemodynamic function and electrical activation better when compared with BiV pacing in a normal swine model. M.W. Kimmel et al. Total endocardial activation durations (TAD), local activation durations (LAD), endocardial breakout(s) (BO), and endocardial activation sequences were analysed for each of several pacing configurations (see Pacing protocol). The BO location was identified as the site on the LV endocardium where depolarization first appeared. This was defined as the instant where the time-derivative of the virtual unipolar electrogram (dV/dt) was maximally negative (maximum negative slope) at the BO location.35–40 The TAD was defined as the interval from endocardial BO to the latest observed LV electrical activation (based on virtual unipolar electrogram recordings). The LAD was defined as the time interval between pacing initiation and LV endocardial BO. Methods Overall experiment durations were on the order of 5–6 h. This research protocol was reviewed and approved by the University of Minnesota Institutional Animal Care and Use Committee, and was designed to ensure the humane treatment of all animals as indicated by the ‘Guide for the Care and Use of Laboratory Animals’ (NIH). All animals (n ¼ 7; 80.8 + 7.3 kg) were initially anesthetized using midazolam (2–3 mg/kg) administered via an ear vein, then intubated and mechanically ventilated to allow administration of isoflurane to maintain a surgical depth of anaesthesia (.1.0 MAC).22 Catheter access to the right ventricle (RV) and LV of the heart was achieved via incisions made in the isolated external jugular veins and right common carotid arteries, respectively. Separate Millar Mikro-Tipw pressure catheters (5 French (Fr), MPC 500, Millar, Houston, TX, USA) were inserted into each ventricle to allow for continuous assessment of ventricular pressures. The derivative of the LV pressure signal was calculated during post-collection data analysis. Maximum positive rate of pressure increase (max þdP/dt) and maximum rate of pressure decrease (max 2dP/dt) values were determined. A Swan-Ganz catheter (7.5 Fr, 93A-931H, American Edwards Laboratories, Irvine, CA, USA) was also inserted via the jugular vein and passed through the RV, placing the catheter’s distal end within a lumen of the pulmonary artery, thus allowing monitoring of pulmonary artery and left atrial (wedge) pressures as well as right atrial pressure. Baseline haemodynamic data were recorded prior to performing a sternotomy. The pericardial fat was removed and the pericardium cut to form a pericardial cradle. After the chest was opened, 7–9 piezoelectric sonomicrometry crystals (SonoMetrics, London, ON, Canada) were individually implanted into the midmyocardium, arranged into pairs septally, anteriorly, and laterally.23–26 Non-contact mapping protocol Using methods similar to those previously published, NCM (EnSite 3000, St Jude Medical, St Paul, MN, USA) was used to record and analyse endocardial electrical activation patterns in the LV.27–35 A 9 Fr multielectrode array was inserted via the left coronary artery, and a 7 Fr steerable electrophysiology catheter (Conductr MC 6022, Medtronic, Inc., Minneapolis, MN, USA) was introduced via the left carotid artery. Catheters were visualized using fluoroscopy to monitor and verify position within the heart. Under fluoroscopic guidance, endocardial pacing leads were fixed in the right atrial appendage (RAA-intrins; CapsureSense 4574, Medtronic, Inc.), RV apex (RVA; CapsureFix Novus 5076, Medtronic, Inc.), and mid-RV septum (RVS; CapsureFix Novus 5076, Medtronic, Inc.). The LV epicardial lead (LV-epi; Streamline 6495, Medtronic, Inc.) was placed at a high posterior-lateral location, which was chosen as the site of latest endocardial LV depolarization as determined by NCM during RAA-intrinsic pacing. Baseline intrinsic activation was elicited by pacing from the RAA-intrins lead, and subsequently recorded. Single-site ventricular pacing was performed (DDD, 140 bpm, 0.5 ms, 5V, 100 ms AV delay) randomly from each location (Figure 1) with haemodynamic and NCM data collected after 5 min of consistent pacing. Biventricular pacing was performed using either the RVS (RVS-BiV) or the RVA (RVA-BiV) endocardial lead combined with the LV-epi lead (Figure 1). Pacing (140 bpm, 0.5 ms, 7V) was carried out randomly in both aforementioned BiV configurations and data were recorded following at least 5 min of consistent capture. Capture was verified by ECG morphology and haemodynamic analysis, and noted on NCM. Statistical analysis Repeated measures analysis of variance (ANOVA) was performed to determine the relative effects of pacing site or mode on the resultant electrical and haemodynamic parameters. When significance was indicated by ANOVA, a Fisher’s least squares post hoc test was performed, with a P-value of ,0.05 being considered significant. All values are reported as the mean+standard deviation. Comparisons were made between RAA-paced intrinsic activation and each of the various single-site and BiV pacing modes, and also between the RV and BiV pacing modes. Results Electrophysiologic data Mean baseline QRS duration was 47.5 + 5 ms and mean baseline endocardial TAD was 45.8 + 14 ms during RAA pacing rhythm (n ¼ 7). All pacing interventions resulted in significantly longer TADs and QRS durations when compared to those produced by intrinsic RAA pacing (P , 0.05; Table 1). It should be noted that both BiV pacing combinations produced significantly shorter LAD and QRS durations compared to their respective single-site counterparts (P , 0.05). Also, Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 Pacing protocol Single-site ventricular and biventricular pacing 1165 (Figure 2F). These two activation wavefronts also fused quickly on the posterior surface, progressed to the apex, around to the anterior surface, and then terminated basally at the septum. Haemodynamic data when compared to each single-site and BiV pacing mode, RVA pacing resulted in the longest TADs and QRS durations (P , 0.05). Figure 2 illustrates a typical isochronal activation map generated by each pacing mode. Similar to RAA-intrinsic pacing (Figure 2A), it was observed that RVS pacing (Figure 2B) produced a focal LV BO located in the mid-septal region of the LV endocardium that led to a single activation wavefront that propagated across the inferior portion of the LV and then traversed up the lateral wall. In contrast, depolarization from RVA pacing (Figure 2C) initiated in the apex of the LV and then travelled radially up the endocardium and terminated in the high basal region. The activation generated by pacing from the LV-epi position (Figure 2D) created a pattern opposite of that generated during RAA and RVS pacing. Conversely, both BiV pacing interventions elicited two near-simultaneous BO and their resulting depolarization wavefronts quickly converged. Specifically, RVS-BiV pacing produced a high-lateral BO, with the activation wavefront moving initially towards the anterior surface, then down the lateral wall to the apex, and finally up the septum to a basal-septal termination (Figure 2E). Right ventricular apex biventricular pacing resulted in two near-simultaneous BO, one high on the posterior-lateral wall and the other at a low septal location Regional cardiac mechanics Regional LV dysfunction was seen in the pace-activated LV myocardium as shown in Figure 4, especially during LV-epi and BiV pacing. The lateral wall crystal pair (4:5) exhibited the characteristic ‘hour glass’ shape (during LV-epi and both BiV) indicative of negative external work, while the septal crystal pair (3:6) showed a widened waveform (during LV-epi and RVA-BiV) caused by increased external work relative to normal myocardium. Discussion At the present time, less symptomatic patients without significant systolic dysfunction and AV block who require pacing support do not meet guidelines for CRT. As more patients with a wider range of symptoms are implanted with BiV systems and as patients are upgraded from dual to triple chamber systems, the effects of BiV pacing in a heart with preserved conduction need to be ascertained.41,42 Early implementation of CRT (NYHA functional class I or II) has been suggested as a means to prevent disease progression11,17,43,44 and there is current investigation into whether BiV is superior to conventional RV pacing in slowing the progression of HF.45,46 Provided the ability of CRT to reverse detrimental remodelling of the heart, pacing in a more structurally normal heart becomes of interest.47–50 The current study demonstrated the utility of endocardial electrical activation measurements, simultaneous with recordings of haemodynamic and mechanical parameters, to evaluate the sequelae of various pacing modes in an intact swine heart. Despite recently published reports focusing on the outcomes of CRT therapy, there remains a need to further investigate the mechanisms underlying the outcomes seen with CRT.2,51,52 Recently, Frias et al.53 performed pacing in AV block canines and compared acute AV sequential pacing to atrio-biventricular pacing performed from the RV (apex and outflow tract) and LV (apex and base). It was demonstrated that QRS durations shortened and LV performance improved with epicardial BiV pacing compared to standard single-site ventricular pacing. However, Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 Figure 1 (A) Diagram of the normal intrinsic conduction system, with its constituent parts labelled, depicting the natural electrical activation progression beginning at the sino-atrial (SA) node, progressing through the atria, to the atrio-ventricular (AV) node, through the bundle of His, down the bundle branches, and finally passing through the Purkinje fibres before dissipating into the myocardium. The endocardial electrical BO (as observed using noncontact mapping) is shown by the blue circle. (B) Pacing lead locations for the right atrial appendage (RAA-intrins), right ventricular septum (RVS), right ventricular apex (RVA), and left ventricular epicardial (LV-epi) leads. Lead locations and combinations are shown both in relation to the native conduction system, and also in anatomic positions. All RV leads were implanted endocardially. Intrinsic activation was elicited by pacing from the RAA-intrins. Single-site pacing was performed from the RVA and RVS locations, while BiV pacing included the addition of the LV-epi lead. (Rendered anatomic image used with permission from Medtronic, Inc., Minneapolis, MN, USA). A summary of the haemodynamic parameters is also presented in Table 1. Compared to RAA-paced intrinsic LV activation, RVA-BiV pacing was the only intervention that demonstrated a significant reduction in the maximum generated LV pressure and LV max þdP/dt, both indicators of systolic function (P , 0.05). No significant changes in systolic function were observed with either single-site pacing from the RV. Minimum LV pressure (min LVP) and maximum 2dP/dt, indicators of diastolic function, were not significantly affected regardless of pacing intervention. It is notable, however, that both systolic and diastolic function tended to be impaired more with BiV pacing than with single-site pacing, although these differences were not statistically significant (Figure 3, P ¼ ns). 1166 M.W. Kimmel et al. Table 1 Haemodynamic and left ventricular electrical activation data measured for each pacing site and modea max LVP (mmHg) min LVP (mmHg) max þdP/dt (mmHg/s) max 2dP/dt (mmHg/s) QRS (ms) TAD (ms) LAD (ms) RAA-intrins LV-epi RVA RVA-BiV RVS RVS-BiV 83.9 + 9.0 6.6 + 7.7 1272 + 285 21532 + 226 47.5 + 4.8 45.8 + 13.9 N/A 70.1 + 18.7 5.9 + 5.7 1077 + 194 21299 + 657 74.8 + 11.0* 58.3 + 3.7* 26.2 + 3.5 71.3 + 18.5 4.9 + 3.4 1077 + 135 21506 + 874 72.9 + 3.6*** 63.2 + 7.6*** 30.1 + 6.1** 62.6 + 23.1* 4.1 + 2.9 927 + 286* 21104 + 778 59.9 + 4.6* 52.7 + 6.3* 26.9 + 8.6 71.8 + 14.8 4.8 + 3.1 1101 + 177 21532 + 840 60.7 + 8.2*** 52.1 + 10.4* 41.5 + 4.7** 69.6 + 15.2 4.8 + 3.1 1045 + 180 21232 + 679 56.3 + 7.9* 53.9 + 6.0* 23.5 + 4.7 Figure 2 Isochronal maps showing propagation of left ventricular (LV) endocardial electrical activation. In these images, colour corresponds to relative activation time, with white representing the location of earliest electrical activity and blue or purple denoting the site of latest recorded activity. These three-dimensional LV reconstructions are shown both in anterior/posterior (AP) and posterior/anterior (PA) orientations. Diagrams are included depicting the pacing site (‘burst’ symbol) and activation progression corresponding to the following pacing locations: (A) right atrial appendage (RAA-intrins), (B) right ventricular septum (RVS), (C ) RV apex (RVA), (D) LV epicardial lead (LV-epi), (E) RV septum biventricular (RVS-BiV), and (F) RV apex biventricular (RVA-BiV). Blue dots indicate BO locations on the LV endocardial maps; green arrows signify normal fast conduction; solid red arrows indicate abnormal fast conduction; dashed red arrows indicate abnormal, transmural slow conduction. Atrial pacing location is indicated by amber ‘burst’ symbol, with amber arrows signifying atrial activation. As ventricular activation was examined in this study, atrial pacing was utilized in each case (except RAA pacing) to minimize the effects of intrinsic atrial activation on the ventricles. it should be noted that, compared to humans, canines have marked electrophysiological differences which may limit translational relevance to the clinical arena; specifically, Bowman and coworkers18,54 demonstrated that the electrophysiological parameters of the swine were more similar to those found in humans than those from canines. Electrophysiology The current study employed NCM to record endocardial electrical activation sequences during paced conditions and demonstrated RVS pacing to elicit depolarization that most closely mimicked the RAA-intrinsic waveform. Prinzen et al.55 reported that LV function is more dependent on Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 a Haemodynamics and electrical timing values resulting from pacing at the right atrial appendage (RAA-intrins), left ventricular epicardial (LV-epi), right ventricular apex (RVA), right ventricular apex biventricular (RVA-BiV), right ventricular septum (RVS), and right ventricular septum biventricular (RVS-BiV) pacing. Maximum and minimum left ventricular pressures (LVP) are given in mmHg, positive and negative pressure-time derivatives (dP/dt) are in mmHg/s, and electrical activation parameters [QRS duration (QRS), total activation duration (TAD), and local activation duration (LAD)] are in ms. All data are shown as mean+SD [*P , 0.05 vs. RAA-intrins pacing, **P , 0.05 vs. corresponding BiV pair]. Single-site ventricular and biventricular pacing 1167 max LVP, max þdP/dt, and max 2dP/dt values. Specifically, systolic performance was significantly impaired during both RVA-BiV (P , 0.05) and RVS-BiV (P 0.10) pacing compared to RAA-intrins pacing. This occurred even while QRS durations were at their shortest, highlighting the important role mechanical synchrony plays in haemodynamic performance. Regional cardiac mechanics Limitations the sequence than the synchrony of electrical activation, thereby highlighting the importance of such findings. The LV activation maps generated during RAA-intrinsic pacing paralleled the LV depolarization patterns found by Durrer et al.56 using multiple intramural electrodes and was similar to those reported by Cassidy et al.57 All pacing sites resulted in increased total activation durations. Myerburg et al. 58 determined that in the RV, electrical impulses can enter the Purkinje network from the lower septum as well as certain locations in the RVOT. This relationship is mirrored in the activation patterns recorded in the present study – RVS pacing resulted in an LV pattern that mimicked RAA-intrinsic pacing, while RVA pacing caused an LV pattern that initiated at the apex. The same relationship was reflected in overall ventricular activation timing, in that pacing from the RVA lead resulted in a longer TAD than did RVS pacing. This was likely due to transmural conduction across the septum that progressed more slowly than that along the intrinsic conduction system. While the LAD was longer for RVS pacing than RVA, once LV BO occurred, the chamber depolarized quicker, indicating preferential conduction. Study limitations include not optimizing the interventricular (V–V) pacing interval, pacing at a high, non-physiologic rate, and not studying the influence of pacing site in a chronic swine model. Simultaneous pacing at each lead location was performed during BiV pacing rather than optimizing the V–V timing, likely generating increased interventricular mechanical dyssynchrony. However, it has been reported that the majority of the improvement in CRT patients is attributed to the simple implementation of pacing, rather than optimization of V–V timing.65–69 By consistently pacing from the RAA in each situation, the pacing rate and AV delay were controlled to preclude the native rate from interfering with paced activation, as well as to prevent retrograde atrial activation.70 Native AV intervals ranged from 150 to 200 ms, and while a paced heart rate of 140 bpm is not considered optimal from a cardiac performance standpoint, this rate was necessary due to the elevated native heart rate of the swine during the study. Future studies are merited to investigate the effect of pacing rates, as well as A–V and V–V intervals. Before a direct application to the clinical setting can be ascertained, chronic animal studies need to be performed to elucidate whether or not these mechanisms are similar in the chronically paced heart. Haemodynamics Conclusion A trend for greater impairment of haemodynamic performance was associated with BiV pacing, as shown by decreased The results of this study suggest that acute BiV pacing in a structurally normal heart both prolongs LV endocardial Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 Figure 3 (A) Comparison of maximum positive change in left ventricular (LV) pressure generated during single-site (RAA-intrins, LV-epi, RVA, RVS) and biventricular (RVA-BiV, RVS-BiV) pacing modes (asterisk – P,0.05 vs. RAA-intrins pacing). (B) Comparison of maximum negative change in LV pressure generated during singlesite (RAA-intrins, LV-epi, RVA, RVS) and biventricular (RVA-BiV, RVS-BiV) pacing modes (RAA-intrins, right atrial appendage; LV-epi, left ventricular epicardial; RVA, right ventricular apex; RVA-BiV, right ventricular apex biventricular; RVS, right ventricular septum; RVS-BiV, right ventricular septum biventricular). Similar to published work, local dysfunction was observed in LV regions near the pacing sites59,60 as demonstrated by regional pressure-length loops shown in Figure 4. Prinzen et al.61 demonstrated in canines that total myocardial work is reduced by 50% in early-activated regions and increased by 50% in late-activated regions, as compared with normal electrical activation. This can be seen in the characteristic ‘hourglass’ shape of the lateral crystal pair trace (4:5) during LV-epi and both BiV pacing modes, and in the wide septal crystal pair trace (3:6) during LV-epi and RVA-BiV pacing. It stands to reason that in a healthy heart, any disruption or change in the electrical activation would result in suboptimal performance. As was found by Tyers,62 the greater the departure from intrinsic activation, the worse the haemodynamic performance. Specifically, BiV pacing is a greater departure from native excitation when compared to singlesite pacing, and should correspondingly impair function to a greater degree. Epicardial pacing effectively reverses this, further contributing to an abnormal activation sequence, especially in healthy myocardium.63 Similar to research published by Faris et al.,64 caution needs to be taken in deriving direct clinical application from the results of the present study, as healthy hearts were used. 1168 M.W. Kimmel et al. activation and induces systolic haemodynamic dysfunction, regardless of anatomic location of the RV pacing lead. Single-site pacing of the RV or LV within an otherwise healthy heart will likewise compromise haemodynamic performance. With the goal of maintaining a physiologic-like activation sequence and minimizing regional dysfunction, it is believed that pacing from a lead placed on the RV septum best maintains normal cardiac function in structurally normal hearts. Conflict of interest: M.W.K., N.D.S., and T.G.L. are employees and shareholders of Medtronic, Inc. Funding Funding was provided by Medtronic, Inc. (basic research contract), and the Institute for Engineering in Medicine and Department of Surgery, University of Minnesota. References 1. Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K et al. Heart disease and stroke statistics–2007 update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2006;115:e69–e171. 2. Saxon LA, De Marco T, Stevenson LW, Costanzo MR, Tomaselli GF, Young JB et al. Resynchronization therapy for heart failure. NASPE Expert Consensus Statement, 2003, 1–39. 3. Bleasdale RA, Frenneaux MP. Cardiac resynchronisation therapy: when the drugs don’t work. Heart 2004;90(Suppl. 6):vi2–4. 4. Seidl K, Rameken M, Vater M, Senges J. Cardiac resynchronization therapy in patients with chronic heart failure: pathophysiology and current experience. Am J Cardiovasc Drugs 2002;2:219–26. 5. Philippon F. Cardiac resynchronization therapy: device-based medicine for heart failure. J Card Surg 2004;19:270–4. 6. Berger T, Hanser F, Hintringer F, Poelzl G, Fischer G, Modre R et al. Effects of cardiac resynchronization therapy on ventricular repolarization in patients with congestive heart failure. J Cardiovasc Electrophysiol 2005;16:611–7. 7. Cazeau S, Bordachar P, Jauvert G, Lazarus A, Alonso C, Vandrell MC et al. Echocardiographic modeling of cardiac dyssynchrony before and during multisite stimulation: a prospective study. Pacing Clin Electrophysiol 2003;26:137–43. Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 Figure 4 Representative regional pressure-length loops for sonometric crystal segments depicted on LV schematic resulting from single-site (RAA-intrins, LV-epi, RVA, RVS) and biventricular (RVA-BiV, RVS-BiV) pacing modes. The area within each loop corresponds to regional stroke work. Early activated myocardium is designated by a ‘þ’ and late activated tissue by a ‘2’. Early-activated LV segments exhibited negative work (work done on not by the segment) while late-activated segments showed larger stroke work than normal [Ant, anterior crystal pair (1:2); Sept, septal crystal pair (3:6); Lat, lateral crystal pair (4:5); RAA-intrins, right atrial appendage; LV-epi, left ventricular epicardial; RVA, right ventricular apex; RVA-BiV, right ventricular apex biventricular; RVS, right ventricular septum; RVS-BiV, right ventricular septum biventricular). Single-site ventricular and biventricular pacing 32. Fung JW, Chan JY, Yip GW, Chan HC, Chan WW, Zhang Q et al. Effect of left ventricular endocardial activation pattern on echocardiographic and clinical response to cardiac resynchronization therapy. Heart 2007; 93:432–7. 33. Skadsberg ND, Coles JA, Iaizzo PA. Electrophysiologic assessment of right ventricular cardiac pacing sites employing non-contact electrical mapping. Int J Bioelectromag 2005;7:325–8. 34. Laske TG, Skadsberg ND, Hill AJ, Klein GJ, Iaizzo PA. Excitation of the intrinsic conduction system through his and interventricular septal pacing. Pacing Clin Electrophysiol 2006;29:397–405. 35. Kroll M, Kriebel T, Windhagen-Mahnert B, Franzbach B, Jux C, Zutz M et al. Origin of electrical activation within the right atrial and left ventricular walls: differentiation by electrogram characteristics using the noncontact mapping system. Pacing Clin Electrophysiol 2003;26:1970–8. 36. Paul T, Moak JP, Morris C, Garson A Jr. Epicardial mapping: how to measure local activation? Pacing Clin Electrophysiol 1990;13:285–92. 37. Weiss C, Willems S, Rueppel R, Hoffmann M, Meinertz T. Electroanatomical mapping (CARTO) of ectopic atrial tachycardia: impact of bipolar and unipolar local electrogram annotation for localization the focal origin. J Interv Card Electrophysiol 2001;5:101–7. 38. Kimber S, Downar E, Masse S, Sevaptsidis E, Chen T, Mickleborough L et al. A comparison of unipolar and bipolar electrodes during cardiac mapping studies. Pacing Clin Electrophysiol 1996;19:1196–204. 39. Anderson KP, Walker R, Fuller M, Dustman T, Ershler PR, Lux RL. Criteria for local myocardial electrical activation: effects of electrogram characteristics. IEEE Trans Biomed Eng 1993;40:169–81. 40. Potse M, van Dessel PF, Linnenbank AC, Grimbergen CA, van Hemel NM, de Bakker JM. Properties of unipolar electrograms recorded with a multielectrode basket catheter. J Electrocardiol 2004;37:1–10. 41. Achilli A, Sassara M, Ficili S, Pontillo D, Achilli P, Alessi C et al. Long-term effectiveness of cardiac resynchronization therapy in patients with refractory heart failure and ‘narrow’ QRS. J Am Coll Cardiol 2003;42: 2117–24. 42. Gasparini M, Mantica M, Galimberti P, Marconi M, Genovese L, Faletra F et al. Beneficial effects of biventricular pacing in patients with a ‘narrow’ QRS. Pacing Clin Electrophysiol 2003;26:169–74. 43. Donal E, Leclercq C, Linde C, Daubert JC. Effects of cardiac resynchronization therapy on disease progression in chronic heart failure. Eur Heart J 2006;27:1018–25. 44. Abraham WT, Young JB, Leon AR, Adler S, Bank AJ, Hall SA et al. Effects of cardiac resynchronization on disease progression in patients with left ventricular systolic dysfunction, an indication for an implantable cardioverter-defibrillator, and mildly symptomatic chronic heart failure. Circulation 2004;110:2864–8. 45. Curtis AB, Adamson PB, Chung E, John Sutton MS, Tang F, Worley S. Biventricular versus right ventricular pacing in patients with AV block (BLOCK HF): clinical study design and rationale. J Cardiovasc Electrophysiol 2007; [Epub ahead of print]. 46. Kindermann M, Hennen B, Jung J, Geisel J, Bohm M, Frohlig G. Biventricular versus conventional right ventricular stimulation for patients with standard pacing indication and left ventricular dysfunction: the Homburg Biventricular Pacing Evaluation (HOBIPACE). J Am Coll Cardiol 2006;47:1927–37. 47. Schuster P, Faerestrand S, Ohm OJ. Reverse remodelling of systolic left ventricular contraction pattern by long term cardiac resynchronisation therapy: colour Doppler shows resynchronisation. Heart 2004;90:1411–6. 48. Yu CM, Fung JW, Chan CK, Chan YS, Zhang Q, Lin H et al. Comparison of efficacy of reverse remodeling and clinical improvement for relatively narrow and wide QRS complexes after cardiac resynchronization therapy for heart failure. J Cardiovasc Electrophysiol 2004;15:1058–65. 49. Auricchio A, Abraham WT. Cardiac resynchronization therapy: current state of the art: cost versus benefit. Circulation 2004;109:300–7. 50. Erol-Yilmaz A, Verberne HJ, Schrama TA, Hrudova J, De Winter RJ, Van Eck-Smit BL et al. Cardiac resynchronization induces favorable neurohumoral changes. Pacing Clin Electrophysiol 2005;28:304–10. 51. Bradley DJ, Bradley EA, Baughman KL, Berger RD, Calkins H, Goodman SN et al. Cardiac resynchronization and death from progressive heart failure: a meta-analysis of randomized controlled trials. JAMA 2003; 289:730–40. 52. Leclercq C, Hare JM. Ventricular resynchronization: current state of the art. Circulation 2004;109:296–9. 53. Frias PA, Corvera JS, Schmarkey L, Strieper M, Campbell RM, Vinten-Johansen J. Evaluation of myocardial performance with conventional single-site ventricular pacing and biventricular pacing in a canine model of atrioventricular block. J Cardiovasc Electrophysiol 2003;14: 996–1000. Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 8. Linde C, Leclercq C, Rex S, Garrigue S, Lavergne T, Cazeau S et al. Longterm benefits of biventricular pacing in congestive heart failure: results from the MUltisite STimulation in cardiomyopathy (MUSTIC) study. J Am Coll Cardiol 2002;40:111–8. 9. Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 2001;344:873–80. 10. Cazeau S, Ritter P, Lazarus A, Gras D, Backdach H, Mundler O et al. Multisite pacing for end-stage heart failure: early experience. Pacing Clin Electrophysiol 1996;19:1748–57. 11. Daubert JC, Leclercq C, Donal E, Mabo P. Cardiac resynchronisation therapy in heart failure: current status. Heart Fail Rev 2006;11:147–54. 12. Abraham WT, Hayes DL. Cardiac resynchronization therapy for heart failure. Circulation 2003;108:2596–603. 13. Maessen JG, Phelps B, Dekker AL, Dijkman B. Minimal invasive epicardial lead implantation: optimizing cardiac resynchronization with a new mapping device for epicardial lead placement. Eur J Cardiothorac Surg 2004;25:894–6. 14. Dekker AL, Phelps B, Dijkman B, van der Nagel T, van der Veen FH, Geskes GG et al. Epicardial left ventricular lead placement for cardiac resynchronization therapy: optimal pace site selection with pressurevolume loops. J Thorac Cardiovasc Surg 2004;127:1641–7. 15. Auricchio A, Stellbrink C, Block M, Sack S, Vogt J, Bakker P et al. Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. The Pacing Therapies for Congestive Heart Failure Study Group. The Guidant Congestive Heart Failure Research Group. Circulation 1999;99:2993–3001. 16. Butter C, Auricchio A, Stellbrink C, Fleck E, Ding J, Yu Y et al. Effect of resynchronization therapy stimulation site on the systolic function of heart failure patients. Circulation 2001;104:3026–9. 17. Ellenbogen KA, Kay GN, Lau C-P, Wilkoff BL, eds. Clinical Cardiac Pacing, Defibrillation, and Resynchronization Therapy, 3rd edition. Philadelphia, W.B. Saunders; 2007. 18. Iaizzo PA. ed. Handbook of Cardiac Anatomy, Physiology, and Devices. Totowa, NJ: Humana Press; 2005. 19. Lambiase PD, Rinaldi A, Hauck J, Mobb M, Elliott D, Mohammad S et al. Non-contact left ventricular endocardial mapping in cardiac resynchronisation therapy. Heart 2004;90:44–51. 20. Ansalone G, Giannantoni P, Ricci R, Trambaiolo P, Fedele F, Santini M. Doppler myocardial imaging to evaluate the effectiveness of pacing sites in patients receiving biventricular pacing. J Am Coll Cardiol 2002; 39:489–99. 21. Leclercq C, Kass DA. Retiming the failing heart: principles and current clinical status of cardiac resynchronization. J Am Coll Cardiol 2002;39: 194–201. 22. Lundeen G, Manohar M, Parks C. Systemic distribution of blood flow in swine while awake and during 1.0 and 1.5 MAC isoflurane anesthesia with or without 50% nitrous oxide. Anesth Analg 1983;62:499–512. 23. Badke FR, Boinay P, Covell JW. Effects of ventricular pacing on regional left ventricular performance in the dog. Am J Physiol 1980;238:H858–67. 24. Urheim S, Edvardsen T, Torp H, Angelsen B, Smiseth OA. Myocardial strain by Doppler echocardiography. Validation of a new method to quantify regional myocardial function. Circulation 2000;102:1158–64. 25. Hoit BD, Shao Y, McMannis K, Gabel M, Walsh RA. Determination of left atrial volume using sonomicrometry: a cast validation study. Am J Physiol 1993;264:H1011–6. 26. de Forteza E, Armentano R, Biagetti M, Rodriguez Chatruc EM. Real-time pressure-volume diagrams for the evaluation of ventricular function. J Biomed Eng 1986;8:200–6. 27. Schilling RJ, Peters NS, Davies DW. Feasibility of a noncontact catheter for endocardial mapping of human ventricular tachycardia. Circulation 1999;99:2543–52. 28. Schilling RJ, Peters NS, Davies DW. Simultaneous endocardial mapping in the human left ventricle using a noncontact catheter: comparison of contact and reconstructed electrograms during sinus rhythm. Circulation 1998;98:887–98. 29. Schilling RJ, Peters NS, Davies DW. Mapping and ablation of ventricular tachycardia with the aid of a non-contact mapping system. Heart 1999; 81:570–5. 30. Gornick CC, Adler SW, Pederson B, Hauck J, Budd J, Schweitzer J. Validation of a new noncontact catheter system for electroanatomic mapping of left ventricular endocardium. Circulation 1999;99:829–35. 31. Fung JW, Yu CM, Yip G, Zhang Y, Chan H, Kum CC et al. Variable left ventricular activation pattern in patients with heart failure and left bundle branch block. Heart 2004;90:17–9. 1169 1170 63. Fish JM, Di Diego JM, Nesterenko V, Antzelevitch C. Epicardial activation of left ventricular wall prolongs QT interval and transmural dispersion of repolarization: implications for biventricular pacing. Circulation 2004; 109:2136–42. 64. Faris OP, Evans FJ, Dick AJ, Raman VK, Ennis DB, Kass DA et al. Endocardial versus epicardial electrical synchrony during LV free-wall pacing. Am J Physiol Heart Circ Physiol 2003;285:H1864–70. 65. Kass DA, Chen CH, Curry C, Talbot M, Berger R, Fetics B et al. Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation 1999;99: 1567–73. 66. Leclercq C, Faris O, Tunin R, Johnson J, Kato R, Evans F et al. Systolic improvement and mechanical resynchronization does not require electrical synchrony in the dilated failing heart with left bundle-branch block. Circulation 2002;106:1760–3. 67. Verbeek XA, Vernooy K, Peschar M, Cornelussen RN, Prinzen FW. Intraventricular resynchronization for optimal left ventricular function during pacing in experimental left bundle branch block. J Am Coll Cardiol 2003;42:558–67. 68. Auricchio A, Ding J, Spinelli JC, Kramer AP, Salo RW, Hoersch W et al. Cardiac resynchronization therapy restores optimal atrioventricular mechanical timing in heart failure patients with ventricular conduction delay. J Am Coll Cardiol 2002;39:1163–9. 69. Abraham WT, Leon AR, Hannon C, Prather W, Fieberg A. Results of the InSync Marquis clinical trial. Heart Rhythm 2005;2:S65. 70. Bowman TA, Hughes HC. Ventriculoatrial conduction in swine during cardiac pacing: animal model for retrograde conduction. Am Heart J 1984;108:337–41. Downloaded from http://europace.oxfordjournals.org/ at Pennsylvania State University on February 27, 2014 54. Bowman TA, Hughes HC. Swine as an in vivo model for electrophysiologic evaluation of cardiac pacing parameters. Pacing Clin Electrophysiol 1984;7:187–94. 55. Prinzen FW, Van Oosterhout MF, Vanagt WY, Storm C, Reneman RS. Optimization of ventricular function by improving the activation sequence during ventricular pacing. Pacing Clin Electrophysiol 1998;21:2256–60. 56. Durrer D, van Dam RT, Freud GE, Janse MJ, Meijler FL, Arzbaecher RC. Total excitation of the isolated human heart. Circulation 1970;41: 899–12. 57. Cassidy DM, Vassallo JA, Marchlinski FE, Buxton AE, Untereker WJ, Josephson ME. Endocardial mapping in humans in sinus rhythm with normal left ventricles: activation patterns and characteristics of electrograms. Circulation 1984;70:37–42. 58. Myerburg RJ, Nilsson K, Gelband H. Physiology of canine intraventricular conduction and endocardial excitation. Circ Res 1972;30:217–43. 59. Prinzen FW, Peschar M. Relation between the pacing induced sequence of activation and left ventricular pump function in animals. Pacing Clin Electrophysiol 2002;25:484–98. 60. Wyman BT, Hunter WC, Prinzen FW, Faris OP, McVeigh ER. Effects of single- and biventricular pacing on temporal and spatial dynamics of ventricular contraction. Am J Physiol Heart Circ Physiol 2002;282:H372–9. 61. Prinzen FW, Hunter WC, Wyman BT, McVeigh ER. Mapping of regional myocardial strain and work during ventricular pacing: experimental study using magnetic resonance imaging tagging. J Am Coll Cardiol 1999;33: 1735–42. 62. Tyers GF. Comparison of the effect on cardiac function of single-site and simultaneous multiple-site ventricular stimulation after A-V block. J Thorac Cardiovasc Surg 1970;59:211–7. M.W. Kimmel et al.