Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of catecholamine research wikipedia , lookup
Progesterone wikipedia , lookup
Polycystic ovary syndrome wikipedia , lookup
Sexually dimorphic nucleus wikipedia , lookup
Menstrual cycle wikipedia , lookup
Hormone replacement therapy (female-to-male) wikipedia , lookup
Xenoestrogen wikipedia , lookup
Mammary gland wikipedia , lookup
Hormone replacement therapy (menopause) wikipedia , lookup
Congenital adrenal hyperplasia due to 21-hydroxylase deficiency wikipedia , lookup
Adrenal gland wikipedia , lookup
Hypothalamus wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Breast development wikipedia , lookup
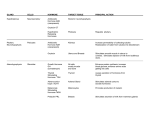
HYPOPHYSIS – PITUITARY HYPOPHYSIS REGIONS HORMONE Growth HormoneGH ACTH TSH FSH PARS DISTALIS EFFECT Stimulates protein synthesis and growth. Stimulates the adrenal cortex to produce the glucocorticoids. Stimulates the thyroid the produce and secrete thyroxin. In females, stimulates the development of follicles in the ovary and their production of estrogen. In males, stimulates spermatogenesis. In females, stimulates ovulation, the formation of the corpus luteum and the production of progesterone by the corpus luteum. LH (ICSH) MSH In males, stimulates the production of testoterone by the interstitial cells. In females, stimulates the production of milk by mammary gland. No known effect. ADH Stimulates the kidneys to retain water. Prolactin PARS INTERMEDIA PARS NERVOSA Oxytocin In females, stimulates contraction during parturition and milk ejection by the mammary glands. THYROID GLAND HORMONE Throxin Calcitonin EFFECT Controls the BMR (basal metabolic rate – cell respiration) Stimulates growth and development. Stimulates deposition of calcium into bone (by the osteoclasts). PARATHYROID GLAND HORMONE PTH EFFECT Promotes an increase in calcium ion concentration in the blood by activating the osteoclasts in bones and stimulating the kidneys to reabsorb calcium. PANCREAS HORMONE Insulin Glucagon EFFECT Stimulates cellular uptake of glucose and the formation of glycogen and fat Stimulates cellular hydrolysis (breakdown) of glycogen. Created by Jason C. Nielson on 11/27/99 Tri 1 ADRENAL GLAND HORMONE Aldosterone Cortisol Epinephrine Norepinephrine EFFECT Acts on the kidneys and their retention of Na+ (ultimate result is retention of water). Acts to make sugar available for cellular respiration during stress. “fight or flight” hormone causes increase in heart rate, heart output, blood pressure, respiratory rate, metabolic rate. THYMUS HORMONE Thymosin EFFECT Appears to be essential in the proper development of the immune system. PINEAL GLAND HORMONE Melatonin EFFECT Produced in greatest amounts at night, health food stores sell this as a sleep aid to minimize jet lag. May influence gonadal development. OVARY* HORMONE Estrogens EFFECT Secreted by the developing follicles – it influences maturation of the sex organs and development of secondary sex characteristics in females and effects growth of the endometrium of the uterus during the menstrual cycle. Progesterone Secreted by the corpus luteum – it influences the development of the endometrium. *see the pituitary hormones FSH and LH as they influence the production of the estrogen and progesterone TESTIS* HORMONE Testosterone EFFECT Secreted by the interstititial cells – in males it influences the development and maintenance of sex organs and development of secondary sex characteristics. * see the pituitary hormone LH for its effect on the production of testosterone and FSH for its effect on spermatogenisis Created by Jason C. Nielson on 11/27/99 Tri 1 HYPOPHYSIS – PITUITARY Hypersecretion of Growth Hormone: Gigantism in children and acromegaly in adults. Hyposecretion of Growth Hormone: Pituitary dwarfism – if the condition occurs during childhood, slows long bone growth. Those with this condition are usually under 4 feet in height but are normally proportioned. Hyposecretion of ADH: Diabetes insipidus – polyuria, polydipsia, severe ionic imbalances. THYROID GLAND Hyperthyroidism: Graves’s disease, considered an autoimmune disease, shows elevated metabolic rate, excessive perspiration, rapid, irregular heartbeat, nervousness and weight loss. Exopthalmos: protrusion of the eyeballs caused by edematous tissue behind the eyes. Hypothyroidism: Cretinism (infantile hypothyroidism) – slows stunted growth, thickened facial features, abnormal bone development and mental retardation. Myxedema – low metabolic rate, lethargy, weight gain, increase in body fluids. Goiter – abnormal growth of thyroid gland. PARATHYROID GLAND Hyperparathyroidism: Demineralization of bone resulting in possible bone deformity and fracture, and stones in the urinary tract. Hypoparathyroidism: Decreased plasma calcium levels which can lead to severe muscle tetany. PANCREAS Hyperinsulinism: Hypoglycemia – resulting in lack of glucose delivery to the brain causing disorientation, unconsciousness and even death (usually the result of an overdose of insulin). Hypoinsulinism: Type I Diabetes (insulin – dependent diabetes mellitus)- elevated glucose levels in the blood and urine. Over time diabetics experience vascular and neural problems. Secondarily, poor circulation may lead to gangrene, blindness, kidney damage and impotence. Type II Diabetes – while occurring later in life, the conditions and problems that accompany Type I diabetes occur here as well. Created by Jason C. Nielson on 11/27/99 Tri 1 ADRENAL GLAND Hypersecretion of corticosteroids: Cushing’s syndrome – change in carbohydrate and protein metabolism resulting in a puffy appearance. In extreme cases, change such as “buffalo hump” and “moon face” occur. Hypersecretion of epineephrine and norepinephrine: Hypertension, hyperglycemia, nervousness, sweating. Complete exhaustion occurs. Hyposecretion of glucocorticoids and mineralocorticoids: Addison’s Disease – hypoglycemia, sodium and potassium imbalance, dehydration, hypotension, and rapid weight loss. Death occurs with lack of treatment. THYMUS Not responsible for any effects of hypo or hyper secretion of thymosin. PINEAL Not responsible for any effects of hypo or hyper secretion of melatonin. OVARY Not responsible for any effects of hypo or hyper secretion of estrogen or progesterone. TESTIS Not responsible for any effects of hypo or hyper secretion of testosterone. Created by Jason C. Nielson on 11/27/99 Tri 1