Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cryptorchidism wikipedia , lookup
Hormonal contraception wikipedia , lookup
Triclocarban wikipedia , lookup
Endocrine disruptor wikipedia , lookup
Menstrual cycle wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Xenoestrogen wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Mammary gland wikipedia , lookup
Breast development wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Vasopressin wikipedia , lookup
Hyperandrogenism wikipedia , lookup
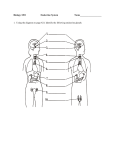
Affects almost every cell, organ, and function of the body The endocrine system is closely linked with the nervous system and the immune system Negative feedback mechanism Hormones ◦ Steroid: act inside the cell ◦ Peptide (protein): act on cell surface ◦ Amine: mechanism of action is same as that of peptide hormone Hormone levels in the blood are mostly maintained by negative feedback A stimulus or low hormone levels in the blood triggers the release of more hormone Hormone release stops once an appropriate level in the blood is reached Most common stimuli Endocrine glands are activated by other hormones Example: ◦Anterior pituitary hormones Figure 9.2a Changing blood levels of certain ions stimulate hormone release Humoral indicates various body fluids such as blood and bile Examples: ◦ Parathyroid hormone ◦ Calcitonin ◦ Insulin Figure 9.2b ◦ Nerve impulses stimulate hormone release ◦ Most are under the control of the sympathetic nervous system ◦ Examples include the release of norepinephrine and epinephrine by the adrenal medulla Figure 9.2c Table 9.1 (1 of 4) Table 9.1 (2 of 4) Table 9.1 (3 of 4) Table 9.1 (4 of 4) HYPOTHALAMUS Produces hormones (called factors) carried via blood in hypothalamic hypophyseal portal system to anterior pituitary. This hormones/factors are involved in normal feedback controls Releasing hormones (RH) cause increased secretion by the anterior pituitary Secondary effect on glands controlled by the pituitary Excess RH causes hypersecretion of other glands Inhibiting hormones (IH) cause decreased secretion by anterior pituitary Secondary effect on glands controlled by the pituitary Excess IH causes hyposecretion of other glands PITUITARY GLAND Located at the base of the brain. Directly affects the function of the other endocrine glands. Promotes growth of body tissues Hormone Secreted Growth hormone Main Functions growth of skeletal muscle, bone, cartilage increase protein synthesis stimulates lipolysis for ATP production reduces glucose use for ATP production increase release of stored glucose from liver raises blood glucose level (diabetogenic effect) triggers thyroid hormone release from thyroid Thyroid-stimulating hormone indirectly enhances basal metabolism of cells via thyroid activation stimulates glucocorticoid (cortisol) secretion from adrenal cortex Adrenocorticotropin hormone indirectly enhances "stress-response" via adrenal activation Prolactin Follicle-stimulating hormone Luteinizing hormone promotes milk production by mammary glands induces spermatogenesis in testes of males after onset of puberty induces 2o oocyte development in ovaries of females after onset of puberty stimulates growth of ovarian follicles (granulosa cells) stimulates estrogen production from ovaries enhances 2o oocyte maturation in ovaries induces ovulation maintains corpus luteum for first two weeks after ovulation stimulates testosterone production from testes Summary: The Hormones of the Pituitary Gland Figure 18–9 Hormone Secreted Oxytocin Antidiuretic hormone Main Functions stimulates uterine contraction (labor contractions) stimulates milk let-down reflex stimulates water retention by renal collecting ducts in kidneys inhibits sweat glands in skin stimulates vasoconstriction in skin (hence name "vasopressin") ANTERIOR PITUITARY •Hyperpituitarism •Hypopituitarism POSTERIOR PITUITARY •Diabetes Insipidus •SIADH (Syndrome of Inappropriate secretion of Antidiuretic Hormone) Children: GIGANTISM occurs in childhood before the closure of epiphyses of the long bones 7-8 Ft. tall, weak, lethargic Adult: ACROMEGALY ◦ occurs after the closure of epiphyses of the long bones o Bone and tissue deformity, enlargement of the viscera w/o an ↑ in height Excessive growth occurs in the feet, hands, nose, chin, visceral organs S/sx: large hands & feet, thickening & protrusion of jaw, arthritic changes, visual disturbances, diaphoresis, oily & rough skin, organomegaly, hypertension, dysphagia, deepening of voice Treatment: Emotional support Frequent skin care Pharmacologic & non-pharmacologic interventions for joint pains Pharmacotherapy ◦ Bromocriptine (Parlodel) to lower GH levels and prolactin levels. Prepare for radiation of pituitary gland or transphenoidal hypophysectomy It is characterized by excessive retention of water by the renal tubules Secondary to excessive secretion of ADH (with a subnormal serum osmolality) They cannot excrete a dilute urine Retain fluid---dilutional hyponatremia Often non-endocrine origin Bronchogenic CA malignant lung cells synthesize and release ADH Can also occur in pts. With severe pneumonia, pneumothorax and other lung disorders Head injury, Tumor, Infection, Surgery directly stimulate P.G. ◦ Some medications (e.g. vincristine, phenothiazines, tricyclic antidepressants, thiazide diuretics) Either directly stimulate the P.G. or Increase the sensitivity of the renal tubules to the circulating ADH S/Sx: Signs of fluid overload changes in LOC & mental status; weight gain (edema), HPN, tachycardia, hyponatremia (DILUTIONAL) Excessive retention of water is not accompanied by proportionate retention of sodium. Management: Eliminate the underlying cause Restrict Na and fluids as prescribed Bec. retained water is excreted slowly by the kidneys Monitor I & O and daily weight; Administer diuretics & monitor IV fluids carefully Furosemide (Lasix) Monitor fluid & electrolyte balance and replace loss as prescribed Meds: Demeclocycline (Declomycin) inhibits ADH-induced water reabsorption & produces water diuresis Monitor for possible nephrotoxicity USUALLY BENIGN But because of their location and effects on hormone production they produce life-threatening effects 3 principal types: ◦ Eosinophilic cells ◦ Basophilic cells ◦ Chromoprobic cells Clinical manifestations: ◦ EOSINOPHILIC TYPES: Develop early in life--GIGANTISM (7fT. TALL) Can bee too weak and lethargic and can’t hardly stand IF IT DEVELOPS DURING ADULT LIFE-ACROMEGALY ◦EOSINOPHILIC TYPES: (cont.) Severe headache Visual disturbances – Loss of color discrimination, diplopia, blindness in a portion of a field of vision. Decalcification of the skeleton, Muscular weakness, Endocrine disturbances (similar with hyperthyroidism) Clinical manifestations: ◦ BASOPHILIC TYPES: Gives rise to Cushing’s syndrome – hyperadrenalism features Masculinization and amenorrhea in females Truncal obesity HPN Osteoporosis Polycythemia Clinical manifestations: ◦CHROMOPHOBIC TYPES: 90% OF PITUITARY TUMORS PRODUCES NO HORMONES--destroys the rest of the Pituitary gland ---resulting in HYPOPITPUITARISM ◦ CHROMOPHOBIC TYPES: (cont.) Physical characteristics Obese and somnolent, Has fine, scanty hair, Dry soft skin, Pasty complexion, and Small bones HEADACHE, loss of libido and visual defects is common Other signs and symptoms: Polyuria, polyphagia, and dec. BMR and subnormal body temp DIAGNOSTIC EXAMS CT/ MRI SCAN Detects presence and extent of Pituitary Tumors Serum levels of pituitary hormones and hormones of target organs MANAGEMENT: Emotional support frequent skin care; pharmacologic & non-pharmacologic interventions for joint pains Pharmacologic mgt. BROMOCRIPTINE (PARLODEL) Dopamine Agonist lower GH levels and prolactin levels OCTREOTIDE (SANDOSTATIN) Synthetic analog of GH inhibit production/ release of GH Can be used preoperative to decrease tumor size and improve pt’s condition Prepare for radiation of pituitary gland or hypophysectomy Removal of pituitary gland TRANSPENOIDAL Hypophysectomy incision is made under the upper lip. Post-operative care: Monitor V/S, neurological status & LOC Elevate head of bed (To prevent cerebral edema) Monitor for increased intracranial pressure & any postnasal drip (RHINORRHEA) which might be CSF Post-operative care: Avoid sneezing, coughing & blowing nose Monitor for temporary diabetes insipidus ( due to removal of the pituitary gland which secretes vasopressin) Monitor I & O & water intoxication Administer antibiotics, analgesics, antipyretics, hormones & glucocorticoids if entire gland is removed (given to prevent crisis) DI – for several days ◦ Tx: vasopressin CSF leakage Visual disturbances Post-operative meningitis Pneumoencephalus (air in the intracranial cavity) SIADH ◦ Hyposecretion of growth hormone by the anterior pituitary gland causing deficiencies in both the pituitary hormones and the hormones of the target glands. ◦ Causes Trauma Tumor P.G. Or Hypothalamus (same effect) Vascular lesion Surgery / radiation of pituitary gland ◦ Panhypopituitrism (Simmond’s disease) total absence of all pituitary secretions. ◦ Sheehan’s syndrome due to postpartum pituitary necrosis It occurs in women with severe bleeding; hypovolemia and hypotension at the time of delivery. S/SX retarded physical growth premature aging hair loss low intellectual development (slow) poor development of secondary sex characteristics Hemianopsia / headache (if due to tumor) Weight loss, emaciation Hypometabolism DIABETES INSIPIDUS Hyposecretion of ADH & deficiency of vasopressin Causes: ◦ Head Trauma, Brain tumor, ablation/ irradiation of Pit. Gland ◦ Nephrogenic failure of kidney tubules to respond to ADH (hypokalemia, hypercalcemia) S/Sx: ◦ polyuria of 4-24 liters/day polydipsia ◦ s/sx of DHN dehydration ◦ Diluted urine (white-colored urine) Sp. Gr. of 1.004 or less; ◦ fatigue, postural hypotension ◦ Constipation Dx. Test: water deprivation test (no fluids for 4 to 18 hours no increase in urine concentration. Management: 1. Replace ADH Vasopressin replacement (desmopressin or DDAVP) Administered intra-nasally WOF HPN, nasal congestion Clofibrate anti-lipidemic has an antidiuretic effect on clients with diabetes insipidus. Chlorpropamide (Diabenese) and thiazide diuretics potentiate the action of vasopressin. Enhances reabsorption of water in the kidney promoting antidiuretic effect & regulates fluid balance 2. Adequate fluid replacement monitoring I & O with specific gravity 3. Provision of safe environment especially with decreasing LOC, wear Medic-Alert bracelet Stimulates melanocytes to produce melanin Inhibited by dopamine Secreted during: ◦ fetal development ◦ early childhood ◦ pregnancy ◦ certain diseases