Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
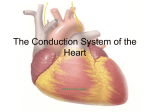
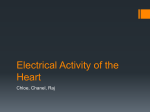
Physiology Chapter 10- Rhythmical Excitation of the Heart Abrevs: AP= action potential Fxn= function Vent= ventricular mv= millivolts inc/dec= increased/decreased b/m= beats per minute Notes Heart has it’s own system to: 1) Generate rhythmical electrical impulses to case rhythmical contraction of the heart muscle 2) Conduct these impulses rapidly through the heart AV node then transmits the signal His bundle R and L bundle braches (perkinje fibers) conduct signal throughout the heart Sinus Node= sinoatrial nodeWhat: specialized cardiac muscle (3x15x1mm) Where: superior posterolateral wall of R atrium, just below and lateral to sup vena cava opening Why: Generate impulse in the atria to travel to the AV node How: capable of self-excitation causes automatic rhythmical discharge and contraction Details: resting membrane potential: -55 to -60 compared to -85 to -90 in ventricular muscle. Sinus cell membranes are “leaky” to Na+ and Ca+ to neutralize some of the intracellular negativity Cardiac Muscle has 3 Types of membrane ion channels: 1) Fast sodium channels- opening causes inc of (+) chargerapid upstroke spike of the AP ( seen in ventricular m.) 2) Slow sodium-calcium channels- “plateau” of ventricular action pot. 3) Potassium channels- returns the membrane potential to resting lvl Sinus Node has same channels, but they have different fxns 1) Fast sodium channels- at -55mv, these are inactivated… they can not be opened 2) Slow sodium-calcium channels- only these can open=cause the AP therefore the atrial AP is slower to develop than the vent AP, and slower to repol Self –Excitation of Sinus Nodal Fibers -High extracellular [Na+] + already open Na+ channels= Na+ leaks into cell -causes slow rise of membrane potential (depol) btwn heartbeats -once this slow rise reaches -40mv threshhold, Na+/Ca+ channels are triggered and full depol occurs -leakiness causes the self-excitation -Repol -Na+/Ca+ channels close 100-150ms after opening -K+ channels open influx out of cell- stay open a little longer and cause hyperpolarization-carries the resting membrane potential to -50 to -60mv Spread of impulse through heart: -Sinus nodal fibers connect to atrial m. fibers (velocity of 0.3m/sec) Specialized conduction fibers (like perkinje fibers, but not as good) in 4 “bands” -Anterior interatrial band- carries impulse to L atrium (v=1m/sec) -3 add’nl bands carry impulse to AV node= Anterior, middle and posterior internodal pathways AV NodeWhere: posterior wall of the R atrium behind tricuspid valve What: allows for delay btwn atrial and vent contraction Total delay in node+bundle= 0.13s + 0.03s conduction time from SA to AV= 0.16s delay from SA node to vent fibers Why: fewer gap junctions btwn cells in the conducting pathway= inc. resistance -only allows one way conduction, AP cannot go from vents to atria -AP can only cross at the AV bundle, atria are otherwise insulated from vents by continuous fibrous barrier Ventricular conduction- Perkinje fibers -Very large (bigger than norm vent m. fibers) - transmit at 1.5 to 4.0m/sec = 150x faster than AV node & 6x faster than vent m. - highly permeable gap junc’s and few myofibrils, so mostly non-contractile tissue -splits into R and L bundle branches just beneath the endocardium along septum -the ends of the fibers penetrate about 1/3 of the way into the muscle mass until the become continuous with the muscle fibers. - total perkinje conduction time= 0.03s -muscle fibers continue the impulse at 1/6th the speed (0.3 to 0.5m/sec) -muscle fibers wrap around the heart in a double spiral, with fibrous septa btwn the spiraling layers…this doubles to the total conduction time from endocardium to epicardium - total time= about 0.06sec= vital to synchronous contraction of vents Control of Excitation and Conduction in the Heart If not stimulated by outside source, AV node and parts of perkinje system will discharge at their own rates: SA node- 70-80 b/m AV node= 40-60 b/m Perkinje fibers= 15-40 b/m SA node discharges the other tissues before they would themselves, so it resets their timer with each impulse, so to speak. SA node is the the pacemaker of the normal heart. Abnormal Pacemakers- Like in EKG lectures! :D Sometimes the other tissues gain a faster discharge rate than the SA node- they become the pacemakers… This can be the AV node, perkinje fibers, or other places in the atrial or vent. m Ectopic Pacemakers- pacemaker anywhere other than SA node -can cause abnormal sequence of contraction, can restrict pumping ability -AV node can take over if SA impulse is being blocked. -When AV block occurs (impulse not transmitted through AV bundle) -Atria contract regularily - Perkinje system kicks in to make vents. contract at 15-40 b/m -Acute A-V bundle block: 5-20sec delay before perkinje fibers being impulses Stokes-Adams syndrome-person faints the first 4-5 sec from lack of blood flow to brain; death can occur if delay is too long Innervation: Parasymp: (Vagus nerve) mostly in SA and AV nodes, little in atria, less in vents -uses ACh inc perm to K+ out of fiber= hyperpolarization (-65 to -70 !) -dec SA rhythm= slower HR -dec excitability of AV junc’l fibers; slows impulse to vents even more - Strong vagal stimulation can stop SA or AV excitation completely Ventricular Escape- perkinje fibers take over at 15-40 b/m Sympathetic: located opposite of para, mostly concentrated in vents. -uses Norepinephrine stims beta-1 adrenergic receptors (mech from here is “unclear” the guess is as follows:) inc perm of membrane to Na+ and Ca+ -raises resting potential in SA node (more excitable, causes higher firing rate) -makes AV node and junc’n more excitable too, which inc rate of conduction -raises perm to Ca+ in musce tissueinc in contraction strength -inc the rate of SA discharge -inc rate of conduction, and excitability in all portions of the heart -greatly inc. force of contraction all over heart -can inc HR x3 and inc contraction strength x2